
Central venous catheterization-related complications in a cohort of 100 hospitalized patients: An observational study
2023-09-24 05:44ReenaSinghNaimishPatelNidhiMehtaGauravSinghNiravPatel
Journal of Acute Disease 2023年4期
Reena Singh ,Naimish Patel ,Nidhi Mehta ,Gaurav Singh ,Nirav Patel
1Department of Internal Medicine,Sri Aurobindo Institute of Medical Science,Indore-453555,Madhya Pradesh,India
2Department of Internal Medicine,G.C.S Medical College Hospital and Research Centre,Ahmedabad-380025,Gujarat,India
3Department of Cardiology,Sri Aurobindo Institute of Medical Science,Indore-453555,Madhya Pradesh,India
ABSTRACT Objective: To evaluate the complications of central venous catheterization (CVC).Methods: A prospective,observational study was conducted at a tertiary care center in India from December 2018 to September 2020.Critically ill patients (aged ≥18 years) in the intensive care unit undergoing CVC procedures were included in the study.Baseline demographics and detailed medical history were recorded.Chest X-rays and electrocardiography were performed on all the patients.Complications associated with CVC were recorded.Results: A total of 100 patients with the indication for central venous catheter insertion were included.The majority (81%) of the patients were inserted with CVC at the right internal jugular vein.Complications such as arterial puncture (2%),hematoma (4%),blood clot formation (4%),catheter kinking (3%),thoracic injury (1%),thrombophlebitis (6%),sepsis (9%) and nerve injury (1%) were reported.Conclusions:Though central venous access is preferred in management of critically ill patients,it has its risks.However,early recognition and prompt management of complications may reduce mortality and morbidity.Physicians and intensive care unit intensivists should be vigilant for central venous catheter-related complications.Suitable site selection,operator experience,and proper catheter maintenance are associated with optimal outcomes.
KEYWORDS: Central venous catheter;Complications;Central line;Central venous access;Critical care;Internal jugular vein
1.Introduction
Central venous catheterization (CVC) is an invasive medical procedure and is widely used for critically ill patients in surgeries where major blood loss or fluid shifts are anticipated[1].Types of central venous catheters include: (i) tunneled;(ii) non-tunneled;(iii) peripherally inserted;and (iv) implantable catheters.The choice and selection of the catheter among the available options depend mainly on the nature and duration of the intended treatment[2].Contraindications of CVC include severe coagulopathy or thrombocytopenia,an uncooperative or combative patient,or the area of cannulation being contaminated,burned,or traumatized.In addition,an inexperienced operator should not attempt central line venous access[3].The indications of CVC include central venous pressure monitoring,failure of other forms of venous access,parenteral nutrition,infusion of certain electrolyte salts,hyperosmolar fluids,vasoactive agents,cytotoxic agents,antibiotics,and hemodynamic status monitoring[4,5].
Despite its advantages,the insertion of a central venous catheter holds a significant risk of serious mechanical complications such as pneumothorax,hemothorax,arterial puncture,and hematoma[6].These complications are associated with the procedure of insertion or the catheter itself.More than 15% of patients who undergo the central venous catheter placement,experience one or more mechanical complications[7].Hence,the frequency of these mechanical complications plays an important role in determining the insertion site.The three common sites used for the CVC are internal jugular vein (IJV),subclavian vein,and femoral vein[8].The site with less thrombosis,lower infection rates,and fewer mechanical complications is considered the ideal site for catheterization[2].Previous studies have reported that femoral insertion is the least preferred site for central venous access due to thrombotic and infectious problems while IJV access (particularly right) is associated with a minimal rate of catheter malposition[4,9].When performed appropriately,the placement of a CVC is safe,productive,and potentially lifesaving.However,particular clinical pearls should be at the forefront of the operator’s mind when performing this procedure.Therefore,the present study was designed to evaluate the complications of CVC.
2.Patients and methods
2.1.Study setting and design
This was a prospective,observational study conducted at a tertiary care center in India between December 2018 and September 2020.
2.2.Inclusion and exclusion criteria
A total of 100 adult patients (aged ≥18 years) admitted to the intensive care unit and undergoing surgical procedures for central venous catheter insertion were included in the study.The patients with a localized skin infection in the neck,a history of neck surgery,post burns or traumatic scar contracture in the neck (altered anatomy),and any localized swelling in the neck were excluded.
2.3.Ethical statement
The study was approved by the institutional ethics committee of GCSMC (Approval number: GCSMC/EC/Dissertation/APPROVE/2018/0032) on date 16 September 2018.The written informed consent was obtained from all the patients.
2.4.Data collection and methodology
Baseline demographics and detailed medical history were recorded.Routine biochemical investigations including complete blood count,random blood glucose,urea,serum creatinine,and coagulation profile were measured.Electrocardiography (ECG) and chest X-ray were performed.Peripheral venous access was obtained.IJV cannulation was performed,and the observations were recorded.
Right IJV was cannulated first in all patients.In case of unsuccessful cannulation at the right IJV,the left IJV was cannulated.Carotid puncture was identified by the presence of a gush of bright red blood.If a carotid puncture occurs,the needle is withdrawn,and compression is applied for five minutes.After five minutes another attempt was made on the same side.If landmarks were obliterated by hematoma,CVC was performed on the other side.Hemothorax was identified clinically and confirmed with a chest X-ray and was treated by insertion of an intercostal drain.Intraoperatively,inability to aspirate dark blood from the catheter and absent or distorted central venous pressure (CVP) waveforms was considered as catheter kinking.Postoperative kinking was identified by chest X-ray.In the case of kinking,the catheter was removed,and another catheter was placed in situ.Migration of the catheter to the ventricle or extrathoracic site was considered as displacement of the catheter and was identified from the CVP waveforms and migration to extrathoracic site was identified from the chest X-ray.The presence of erythema and swelling at the catheter site was considered thrombophlebitis.In such patients,the catheter was removed.Limitation of neck movements was defined as the presence of pain on flexion,extension,and rotation of the neck.Postoperative examination was done to rule out compression to cranial nerves IX,X,XI,and XII if a hematoma had occurred which was considered a nerve injury.
2.5.Statistical analysis
Statistical analysis was carried out using Statistical Package for the Social Sciences (SPSS) Software version 25.0 (SPSS,Inc.,Chicago,IL,USA).Categorical variables were represented as frequency counts and percentages and continuous variables were described as mean and standard deviations.AP-value <0.05 was considered statistically significant.
3.Results
A total of 100 patients who underwent central venous catheter placement were analyzed.Patients within the age group of 46-60 years (39%) were predominant followed by 16-30 years (24%),61-80 years (22%),and 31-45 years (15%) patients.Right IJV was the predominant CVC site (81%),followed by left IJV (7%),right femoral vein (7%),and right subclavian vein (5%) (Table 1).Complications such as sepsis occurred in 9% of patients followed by thrombophlebitis (6%),hematoma (4%),and blood clot formation (4%) (Table 2).
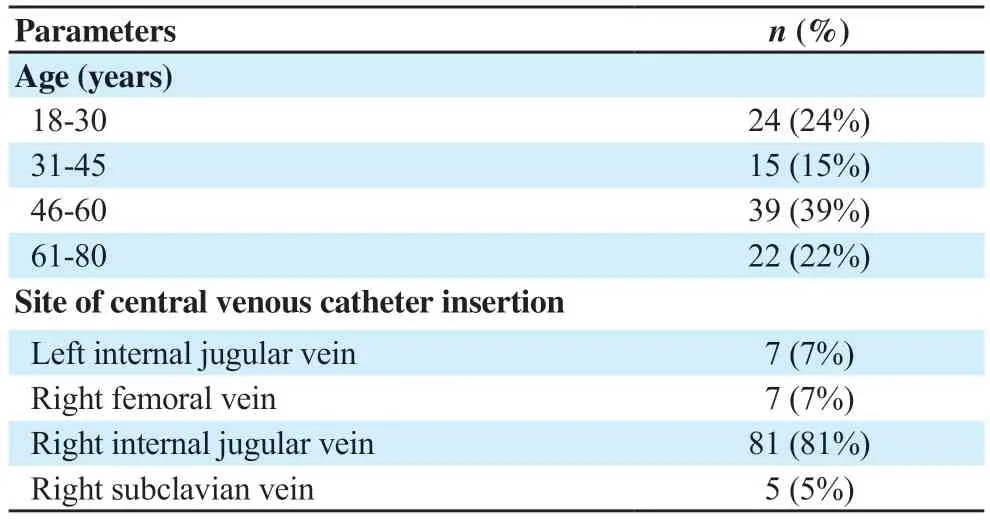
Table 1.Baseline demographic details and the site of central venous catheter insertion in the study population (n=100).
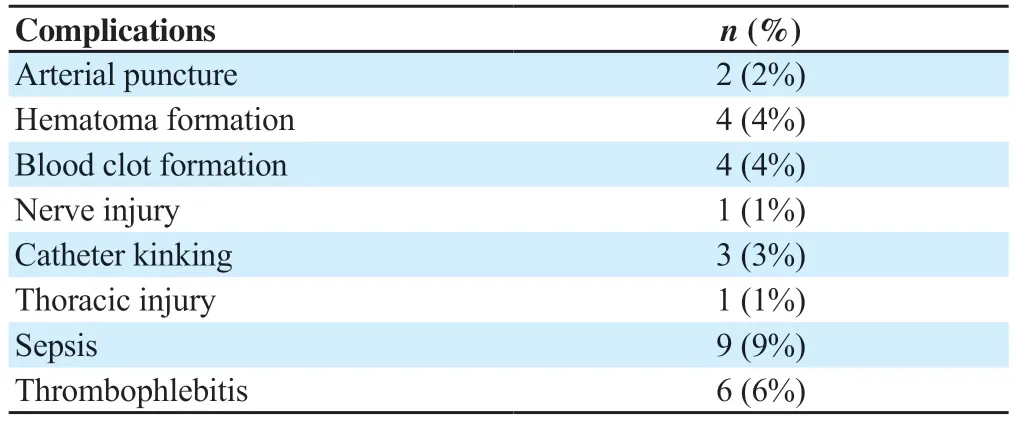
Table 2.Complications associated with central venous catheter insertion in the study population.(n=100).
4.Discussion
In this study,complications associated with CVC were analyzed.Our study demonstrates the clinical relevance and aspects of CVC among critically ill patients.The right IJV was demonstrated as the preferred site to place a central venous catheter because the right IJV drains immediately into the superior vena cava and the left IJV does not.In a review by Patelet al.,it was reported that the apex of the left lung is located at a higher level compared to the right lung.Due to the difference in these anatomical features,the left jugular central line has a higher risk of developing pneumothorax[2].Similarly,the results of a previous study by Bothaet al.reported that the IJV is slightly bigger on the right [(17.29 ± 1.07) mm]than on the left [(15.30 ± 0.25) mm]suggesting the placement of a central venous catheter on the right IJV as a safer site compared to the left IJV[5].Likewise,the results of a former study by Pikweret al.reported that the right IJV should be the preferred site for central venous cannulation to reduce the incidence of extrathoracic positioning[10].A meta-analysis by Sakurayaet al.demonstrated that peripherally inserted central venous catheters which are the substitutes of centrally inserted central venous catheters could be an effective approach to avoid clinically important complication risk in hospitalized patients.However,the lower certainty on the safety of peripherally inserted central venous catheters requires further evidence to clarify the preference for peripherally inserted central venous catheters over centrally inserted central venous catheters[6].Arterial puncture occurred in 2% of patients in our study population which was consistent with a former review by Bowdleet al.,where arterial puncture was reported to occur in about 4.2% to 9.3% of all central line insertions[11].The concern in the case of arterial puncture is whether to remove the catheter immediately with pressure or to leave it in place.Studies have demonstrated that leaving the accidental arterial catheter in place with a quick repair will be more beneficial than removing catheter with pressure[2].Hematoma was observed in 4% patients of in our study which was comparable to an earlier review by Kornbauet al.,where the hematoma formation was reported in about 4.7% of all central venous catheterizations[12].In our study,thrombophlebitis was reported in 6% of patients.The results of a previous study by Madanet al.reported that the factor responsible for the development of thrombophlebitis is the osmolality of the infused fluid[13].Sepsis occurred in 9% of patients,and it was predominant among all the other complications of our study population which may be due to central line infection.
The use of CVC is often crucial for providing necessary patient care.An improved understanding of CVC-related risks might help clinicians choose one approach over the other in specific clinical settings.Moreover,ultrasound guidance has been shown to significantly reduce the risk of complications associated with CVC.This study is limited to a smaller sample size.Hence,larger studies are warranted to understand the complications of CVC in detail and its efficacy in critically ill patients.
We found the incidence of various complications of the central venous line is similar to the available literature,but the incidence of catheter infection is a little bit higher in our hospital.Preventive measures and treatment of catheter-related infections should be given high priority for better outcomes.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Authors'contributions
Naimish P and GS designed and conducted the study.Nirav P and NM conducted data analysis and RS prepared and designed the manuscript,who also acts as the corresponding author of the manuscript.
 Journal of Acute Disease2023年4期
Journal of Acute Disease2023年4期
- Journal of Acute Disease的其它文章
- Biochemical indicators and the Peradeniya Organophosphate Poisoning scale in prediction and prognosis of organophosphorus poisoning: An observational prospective study
- Heparin-binding protein combined with human serum albumin in early assessment of community-acquired pneumonia: A retrospective study
- Clinical profile of febrile encephalopathy patients at a tertiary care hospital in India: A retrospective study
- Effects of long COVID-19 among young adults in Turkey: A crosssectional study
- Epidemiology of animal bite injuries in North of Fars province in Iran
- Clinical and epidemiological features of pelvic fractures presenting to the emergency department in a tertiary health care hospital in south India: A retrospective study