
Clinical and epidemiological features of pelvic fractures presenting to the emergency department in a tertiary health care hospital in south India: A retrospective study
2023-09-24 05:44GugulothRameshBabuYagadiSrilatha
Journal of Acute Disease 2023年4期
Guguloth Ramesh Babu ,Yagadi Srilatha
1Department of Emergency Medicine,Jawaharlal Institute of Postgraduate Medical Education and Research,Puducherry,India
2Department of Emergency Medicine,ESIC Medical College,Hyderabad,India
ABSTRACT Objective: To determine the clinical and epidemiological features of pelvic fracture patients presenting to the Emergency Department.Methods: This prospective observational study was conducted in a tertiary care center in south India.Causes of injury,types of pelvic fractures,the associated injuries,and outcome at the time of discharge were recorded.Results: A total of 140 patients were included in this study.Most patients were classified as type A (n=62),followed by type B (n=48) and type C (n=30).A total of 112 patients were injured due to road traffic accidents,followed by a fall from a height (n=23) and a fall from a heavy object (n=5).Most subjects had facial injuries (n=99,70.7%),followed by head injuries (n=51,36.4%).Five percent of the patients were expired,12% left against medical advice,and 83% were discharged.Conclusions:The incidence of pelvic fractures presenting to the Emergency Department is relatively high in India.Road traffic accidents are the primary cause of pelvic fractures and associated facial and head injuries.The outcomes demonstrate the need for improved prevention strategies and comprehensive management protocols to reduce mortality.
KEYWORDS: Pelvic fracture;Emergency;India;Road traffic accidents;Epidemiological
1.Introduction
Fracture is common in the Emergency Department.Pelvic or acetabular fractures are not very common (3%-9%)[1]as compared with fractures in other parts of the body.High energy forces are required to disrupt the pelvic ring,therefore,pelvic fractures have a significant association with other injuries[2].Pelvic fractures are often seen in 20%-25% of polytrauma patients[3].The main reason for death in patients with pelvic fractures is massive hemorrhage and patients with fatal pelvic fractures and associated injuries die after 2-3 days of trauma[4].Mortality is high in such patients,approximately 10%-16%[5].In the case of open pelvic fracture,mortality is much higher,reported as 50%[6].Trauma-associated comorbidities could affect daily life and increase the mortality rate.
The spectrum of pelvic injuries ranges from low-energy pubic rami fractures to high-energy unstable patterns.Most pelvic fractures are a result of low-energy falls but high energy injury like motor vehicle collisions could cause concomitant multisystem trauma.These injuries can result in hemodynamic instability due to vascular,visceral,or skeletal injury and chronic debilitating pelvic pain and deformity.Thus,timely and effective diagnosis and treatment are essential to save lives and minimize long-term sequelae.Early diagnosis in both prehospital and hospital settings and appropriate management could decrease the immediate and prolonged complications and improves the functional outcome of the patient.
After resuscitation,an examination of the whole body should be performed to check for open wounds or degloving injuries,specifically in the region of the perineum.A detailed neurological examination is needed as well.In most cases multidisciplinary approach is needed as pelvic injuries are commonly associated with visceral and vascular injuries.An initial anteroposterior pelvic radiograph is a part of the routine evaluation in any high-energy blunt trauma injury.Any suspicious detected findings need CT imaging.
Furthermore,evaluation of possible associated injuries is also important even though the greater proportion of pelvic fractures is not life-threatening.Mortality and functional outcome of pelvic ring injuries is determined by several factors,especially associated injuries.Comprehensive epidemiologic surveillance could provide sufficient information to medical staff to improve emergency management.The treatment of hemodynamically unstable patients with an unstable pelvic fracture remains controversial and often depends on the available facilities in the hospital.
In recent years,a considerable number of studies related to pelvic fractures have been done.However,the studies on epidemiological and clinical features of pelvic fractures are scanty in South India.This study is to identify the clinical and epidemiological profile of pelvic fracture patients presenting to the Emergency Department in South India.
2.Patients and methods
It is a prospective observational study conducted in a tertiary care center in South India from April 2018 to March 2019.
2.1.Inclusion and exclusion criteria
All trauma patients with pelvic fractures who presented to the Emergency Department were included in the study from April 2018 to March 2019;there were no exclusion criteria.This is an exploratory study;hence all the patients with pelvic fractures presented to the emergency department were included in the study using a convenience sampling technique.
2.2.Ethical statement
The participants were provided with the information and given informed written consent.The research project JIP/IEC/2017/0435 and its research protocol were approved by institution’s ethics committee.
2.3.Study procedure
After identifying the pelvic fracture in trauma patients based on both clinical and radiological (X-ray) findings,the fracture was classified according to the Tile classification.Age,sex,cause of injury,types of pelvic fractures,the associated injuries,and outcome at the time of discharge were recorded.
2.4.Statistical analysis
The statistical analyses were conducted using IBM SPSS version 24.0.The measurement data exhibited a normal distribution and were described as mean ± standard deviation and categorical variables as frequencies.
3.Results
A total of 140 patients were included in this study.
3.1.Demographic and clinical characteristics
In our study,80% (112) were males and 20% (28) were females.Among the 140 participants in our study,the majority of patients (52.1%) belonged to the age group of 18 to 40 years.
A total of 40 patients had no shock,40 patients had class I shock,36 patients had class Ⅱ shock,14 patients had class Ⅲ shock,and 10 patients had class Ⅳ shock.
3.2.Types of fractures
A total of 93.5% of type A fractures were managed conservatively and the remaining 6.5% were managed surgically.A total of 79.2% of type B fractures were managed conservatively.Among type C fractures,50% were managed surgically.
According to the Tile classification,44.3% of patients belonged to Type A,34.3% to Type B,and 21.4% to Type C.On further subclassification of the patients in our study,17.1% had type A1 fractures,27.1% had type A2 fractures,18.5% had type B1 fractures,8.5% had type B2 fractures,7.1% had type B3 fractures,7.1% had type C1 fractures,2.1% had type C2 fractures and 12.1% had type C3 fractures (Table 1).In our study,two open pelvic fractures were seen among the 140 patients,which accounts for 1.4%.Only one patient with an open pelvic fracture underwent a defunctioning colostomy and another patient expired because of hemorrhagic shock,with a mortality rate of 50% in open pelvic fractures in our study.
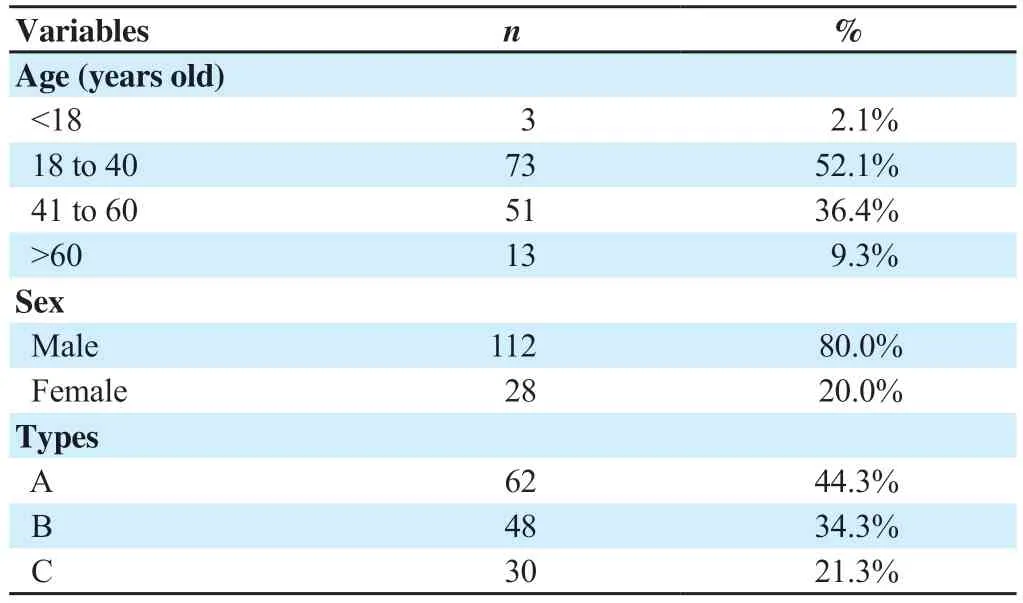
Table 1.Demographic and clinical characteristics (n=140).
3.3.Causes of injury
Table 2 shows the distribution of causes of injury based on different types.A total of 112 patients were injured due to road traffic accidents,followed by a fall from a height (n=23) and a fall from a heavy object (n=5).Injuries due to road traffic accidents accounted for the most proportion of all types.
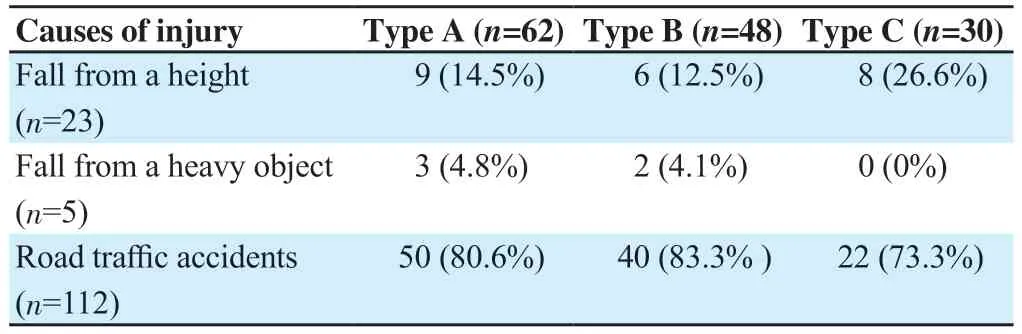
Table 2.Distribution of cause of injury based on types (n=140,n,%).
3.4.Associated injuries
Table 3 shows the associated injuries in the patients.A total of 89% of patients had associated injuries.Most subjects had facial injuries (n=99,70.7%),followed by head injuries (n=51,36.4%).Facial injuries accounted for the most proportion of all types,followed by head injuries,except for type C,intra-abdominal injury accounted for the second most.
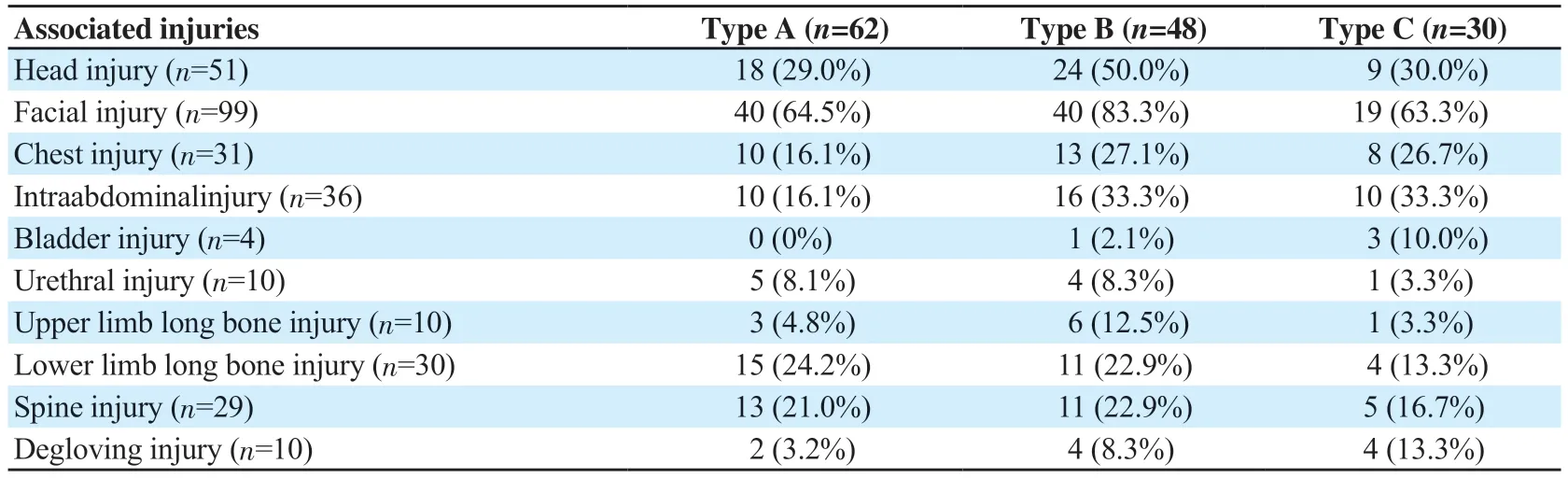
Table 3.Distribution of associated injuries based on types (n=140,n,%).
Table 4 shows the distribution of the associated injuries based on causes.Facial injury accounted for the most proportion of injuries due to road traffic accidents (n=91,81.3%),most patients due to fall from height had spine injury (n=16,70.0%),and most patients due to fall of a heavy object had an intraabdominal injury (n=4,80.0%).
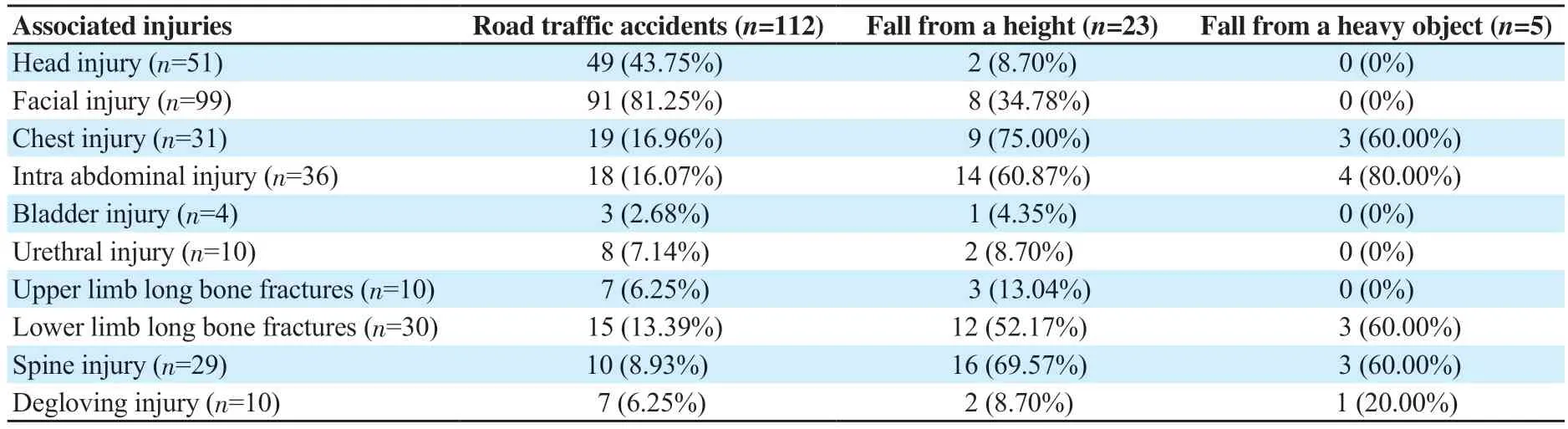
Table 4.Distribution of associated injuries based on causes (n=140,n,%).
3.5.Treatments
A total of 84.3% of patients were referred from other hospitals like district hospitals,primary health care centers,and nearby private hospitals.Most of these patients who were referred from other hospitals received initial treatment like primary airway management,fluid management,and pelvic binder application to stabilize the pelvis.A total of 79% of subjects did not receive primary treatment.A total of 28.5% of patients had no active fluid management,49.2% were treated with crystalloids,and 22.1% were with crystalloids and blood transfusion.
3.6.Outcomes
The median duration of hospital stay in those who underwent operative management was 20 days with an interquartile range (IQR) of 14 days.And,in those patients who received non-operative management,the median duration of stay was 2 days with an IQR of 4 days.Among the 7 patients who died,5 patients died due to delay in presentation to the hospital.Among the patients who died due to immediate complications of pelvic fracture,the average delay in resuscitation was 3 to 6 hours.
A total of 5% of patients were expired,12% of patients left against medical advice,and 83% of patients were discharged.Among these 123 discharged patients,21% of patients underwent surgical treatment and 79% of patients were managed conservatively.
One type A patient died due to abdominal bleeding,one type B patient died due to aspiration pneumonia,one type B patient died due to pulmonary embolism,one type B patient died due to severe head trauma,one type B patient died due to pelvic hemorrhage,and two type B patients died due to pelvic hemorrhage.
A total of 24 patients had class Ⅲ and class Ⅳ hemorrhagic shock.Among these 24 patients,16 patients responded to our fluid management,4 patients were transient responders,and 4 were nonresponders.Among the 4 transient responders,1 patient had a type B fracture with class Ⅲ hemorrhagic shock,and 3 patients had a type C fracture with class Ⅲ hemorrhagic shock.All these 4 patients were taken up for emergency surgery.All 4 non-responders died because of class Ⅳ hemorrhagic shock.
4.Discussion
Pelvic fractures are one of the most severe orthopedic injuries.Amongst all musculoskeletal injuries,pelvic fractures are a major cause of mortality and morbidity.They occur as a result of highimpact force and fortunately are not very common.Pelvic fractures,often resulting from high-energy trauma,pose a significant risk to patients’ lives if not promptly treated[7].Studies indicate a mortality rate of 19% for pelvic ring fractures,which rises to 37% among older patients with severe chest injury or hemodynamic instability[8].
The main reason for mortality is massive hemorrhage.Sunil and Shetty[9]and Holsteinet al.[4]reported a mortality rate of 8.9% and 4%,respectively,and in our study of 140 patients,the mortality rate was 5% (n=7).Among the 7 patients,3 patients died because of pelvic massive hemorrhage and the other 4 died because of extra pelvic causes and complications during a hospital stay.Gansslenet al.[10]showed 13.4% mortality in their epidemiological study and they indicated that the mortality was directly related to the extra pelvic injuries.The same was observed by Chueireet al.[11].They found that 7% mortality in their study,and the mortality had a significant relationship with extra pelvic trauma.
Open pelvic fractures are more dangerous than closed fractures as displacement is frequent in open fractures causing excessive bleeding and colorectal trauma.When there is an open pelvic fracture,mortality was high as 50% as reported in a study by Leenenet al.[6].In our study,2 open pelvic fractures were seen among the 140 patients,which accounts for 1.4%.Only one patient with an open pelvic fracture underwent a defunctioning colostomy and another patient expired because of hemorrhagic shock,with a mortality rate of 50% in open pelvic fractures in our study.A study done by Weaveret al.[12]reported only 1% of open pelvic fractures in 318 patients.An Indian-based study reported 8.9% of open pelvic fractures and among them,only 2 patients underwent defunctioning colostomy[9].A total of 5% of open pelvic fractures were reported in a study by Hermanset al.[13].All open pelvic fractures do not require colostomy.Selective colostomy based on wound location gives a better outcome and avoids unnecessary surgery[14].
Even if the patient survives the initial event,there is excessive morbidity associated with these injuries.The common causes of morbidity include associated injuries,shock index,and prolonged hospital stay-related complications.These factors also cause a heavy burden on the sparse resources.
As the pelvic ring is in close relation with the vascular,neuronal,and visceral structures,associated injuries are often seen in pelvic fractures[15].A Netherlands-based epidemiological study reported that 84.3% of pelvic fracture patients had associated injuries[13].In our study,we found that 89% of patients had associated injuries.
In polytrauma patients,massive bleeding is the common cause of shock.It is very important to diagnose the patients in shock during the initial assessment itself because the chances of mortality are high if the diagnosis of shock is delayed.Early diagnosis and timely effective treatment are essential to save lives and minimize longterm sequelae.
In our study,28.6% of the patients did not have any signs of shock.A total of 28.6% of patients had class I hemorrhagic shock,25.7% of patients had class Ⅱ hemorrhagic shock,10.0% of patients had class Ⅲ hemorrhagic shock and 7.1% of patients had class Ⅳ hemorrhagic shock.No active fluid management was done in those patients who did not have any signs of shock.In patients with hemorrhagic shock,active fluid management was done.Out of the 140 patients,49.2% of patients received only crystalloids as the active fluid management and 22.1% of patients received both crystalloids and blood transfusion as the active fluid management.
The duration of hospital stay varies with the severity of the injury and the definitive treatment received by the patient.When the duration of hospital stay is high,there are chances of developing hospital-acquired infections,deep venous thrombosis,pulmonary embolism,and pulmonary complications like aspiration pneumonia.In our study,the median duration of hospital stay in those who underwent operative management was 20 days with an interquartile IQR of 14 days.And,in those patients who received non-operative management,the median duration of stay was 2 days with an IQR of 4 days.In a study done in the Netherlands,the mean length of stay was 20 days overall,and the mean length of stay in the ICU was 5.5 days[13].
Epidemiological studies of pelvic fractures will provide sufficient information to the medical staff to improve emergency management.Early diagnosis of pelvic fractures in trauma patients,in both prehospital and hospital settings,and appropriate management of stable and unstable pelvic fractures with early management of the associated injuries will reduce the immediate and late complications and improve the functional outcome of the patient.
The population affected is mainly young adult males,who are active members of society and hence,the impact on society is much more.In our study,80% (112) were males and 20% (28) were females.A study done in the Netherlands showed male predominance in 61.1% of cases[13].A Brazilian study showed gender distribution with 57.5% of male patients and 42.5% of female patients[15].
Among the 140 participants in our study,the majority of patients (52.1%) belong to the age group of 18 to 40 years.A total of 2.1% of patients belong to less than 18 years of age,36.4% of patients belong to the age group of 41 to 60 years and 9.3% of patients belong to more than 60 years of age.Similar results were observed by Sunil and Shetty[9],who reported 79% of their patients to be in their 2nd to 4th decade.In a study done by Garget al.[16]among 50 patients,80% of the patients belong to the age group of 18 to 45 years.
Pelvic fractures are a result of high-velocity or high-impact trauma.Hence,road traffic accidents were the most common cause of injury in our study.Fall from height was seen in 16.4% of patients and all of a heavy object in 3.6% of patients.On the whole,in our study,the most common cause of injury was road traffic accidents.We classified these injuries as per Tile classification.Type A fractures were most common which were seen in 44.3% of patients,which was followed by type B (34.3%) and then type C (21.4%) fractures.Gansslenet al.[10]an epidemiological study also found that type A fractures were more common,with 54.8% type A cases,followed by type B and then type C fractures.Chueireet al.[11]reported 55% of type A fractures,30% of type B fractures,and 15% of type C fractures in their study.Freitaset al.[17]analyzed the evolution of pelvic ring fractures in the past decade,where they found type A fractures as the most frequent,followed by type B and then type C.
Pelvic fractures are commonly associated with other high-impact injuries.In our study,70.7% of the patients were having facial injuries,which were the most commonly associated injuries seen.36.4% of patients had associated head injury,25.7% of patients had associated intra-abdominal injury and 22.1% of patients had associated chest trauma.A study by Demetriadeset al.[18]showed the incidence of associated abdominal trauma in severe pelvic injury as 30.7%.Another study done by Sunil and Shetty[9]showed that 29.5% had associated abdominal injuries.Yanget al.[19]have done a study in Taiwan over 12 years and reported that the most commonly associated injuries were orthopedic fractures of lower limbs seen in 21.5% of patients.In our study,facial injuries were the most commonly associated injuries followed by head injuries.This high incidence was because of the improper use of helmets and nonadherence to traffic rules by young adults while driving.
In our study,long bone injuries were more common in lower limbs,seen in 21.4% (n=30) of patients.Among 30 patients,17 patients were having a shaft of femur fracture,which was the most frequent long bone injury associated with the pelvic fracture.
Hertzet al.[20]concluded in their study that bladder injuries are rare with pelvic fractures and may have significant sequelae.In the same study,they found only 6.8% of patients had bladder injury.In our study,bladder injuries were seen in 2.8% of patients.The same percentage (2.8%) was reported in a study by Barrattet al.[21].In our study,7.14% of patients had a urethral injury which is similar to a study done in India by Sunil and Shetty[9],where 10.2% of patients had a urethral injury.
Patients with pelvic fractures need urgent resuscitation and delay in extrication and transport to the hospital can be detrimental to their survival and outcome.A total of 84.3% of patients were referred from other hospitals like district hospitals,primary health care centers,and nearby private hospitals.Most of these patients who were referred from other hospitals received initial treatment like primary airway management,fluid management,and pelvic binder application to stabilize the pelvis,which might have resulted in relatively good outcomes for the patient,even though they presented late to our institute.
Among the patients who died due to immediate complications of pelvic fracture,the average delay in resuscitation was 3 to 6 hours.This delay is mainly because of poor transport facilities.Among the 7 patients who died,5 patients died due to delay in presentation to the hospital.
In our study,most of the patients underwent non-operative management as the mainstay of treatment.A total of 17(12%) patients out of the 140 left against medical advice and the remaining 123 patients got definitive treatment.Among these 123 patients,21% of patients underwent surgical treatment and 79% of patients were managed conservatively.These results are comparable with the studies done by Pereiraet al.[15]and Gansslenet al.[10].
A total of 93.5% of type A fractures were managed conservatively and the remaining 6.5% were managed surgically.A total of 79.2% of type B fractures were managed conservatively which was similar to the results of the study done by Hermanset al.[13],where 73.5% of type B fractures were managed conservatively.Among type C fractures,50% were managed surgically.
Our study has some limitations.The long-term outcome and complications could not be assessed as the patients were followed up only till the time of discharge and the true incidence and prevalence could not be calculated as the study was hospital-based.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Authors'contributions
GRB: Conceptualization,resources,methodology,writing,and draft;YS: Validation,formal analysis,writing,review,and data curation.
 Journal of Acute Disease2023年4期
Journal of Acute Disease2023年4期
- Journal of Acute Disease的其它文章
- Biochemical indicators and the Peradeniya Organophosphate Poisoning scale in prediction and prognosis of organophosphorus poisoning: An observational prospective study
- Heparin-binding protein combined with human serum albumin in early assessment of community-acquired pneumonia: A retrospective study
- Clinical profile of febrile encephalopathy patients at a tertiary care hospital in India: A retrospective study
- Effects of long COVID-19 among young adults in Turkey: A crosssectional study
- Epidemiology of animal bite injuries in North of Fars province in Iran
- Central venous catheterization-related complications in a cohort of 100 hospitalized patients: An observational study