
Evaluation of optic nerve head vessels density changes after phacoemulsification cataract surgery using optical coherence tomography angiography
2023-06-17 06:51ZeHuiZhuYinYingZhaoRuiZouHanZouJiaYanFangPingJunChangYunZhao
Ze-Hui Zhu, Yin-Ying Zhao, Rui Zou, Han Zou, Jia-Yan Fang, Ping-Jun Chang,Yun-E Zhao
1Eye Hospital and School of Ophthalmology and Optometry,Wenzhou Medical University, Wenzhou 325000, Zhejiang Province, China
2National Clinical Research Center for Ocular Diseases,Wenzhou 325000, Zhejiang Province, China
3Eye Hospital of Wenzhou Medical University Hangzhou Branch, Hangzhou 310000, Zhejiang Province, China
Abstract● AlM: To evaluate optic nerve head (ONH) vessel density(VD) changes after cataract surgery using optical coherence tomography angiography (OCTA).
● KEYWORDS: phacoemulsification; cataract; optical coherence tomography angiography; vessel density; optic nerve head
INTRODUCTION
Phacoemulsification cataract surgery is the most widely performed ophthalmic procedure worldwide.Over 10 million people reportedly undergo cataract surgery every year,and this number is said to increase considering the increasing longevity of the global population[1].Detection of ocular blood flow has long been a topic of interest because ocular circulation can indicate the onset and progression of many ocular diseases, such as glaucoma and diabetic retinopathy,and also determine the effectiveness of surgical treatments and drug therapies[2-5].Intraocular pressure (IOP) may exceed 60 mm Hg during cataract surgery, which can lead to compromised optic nerve head (ONH) retinal blood flow[6].Many researchers are interested in the impact of cataract surgery on fundus blood flow, fluctuations in ⅠOP throughout the surgical procedure, and postoperative inflammatory reactions that could disrupt retinal circulation.Although most eyes do well after cataract surgery, the incidence of macular edema and nonarteritic anterior ischemic optic neuropathy are increased after phacoemulsification surgery[7-8]; however, the mechanism underlying these hemodynamic changes remains unclear[4,7-13].
Various advanced techniques have been used to measure changes in fundus blood flow after cataract surgery, including Doppler optical coherence tomography, laser speckle flowgraphy, and optical coherence tomography angiography(OCTA)[4,14].These three noninvasive techniques have been developed to measure retinal blood flow with high levels of resolution, repeatability, and reproducibility[15-17].OCTA employs the motion-contrast technique to visualize erythrocyte movement in both large and small vessels with few limitations.It provides qualitative and quantitative data on the vasculature in the retina and ONH[18].Furthermore, OCTA can measure vascular biomarkers and indicate significant relationships between glaucoma, blood flow, and capillary density in the retina and ONH[19].However, the factors affecting the quality of OCTA images require further investigation.
Quantitative OCTA measurements of eyes with cataract may be affected by refractive media opacification in many ways[20-22].First, opacification reduces the image quality and affects the measurement of retinal thickness and retinal vascular density.Second, it leads to the attenuation of light into the eye and affects the reverse scattering of light detected by OCTA devices, resulting in various image artifacts.Algorithms are constantly being improved in order to overcome these shortcomings[23-24].
Several recent studies have investigated retinal microcirculation changes after cataract surgery, most of which have focused on macular hemodynamic changes[12-13,25].One study that assessed the changes in ONH vessel density (VD) after phacoemulsification surgery showed an increase in ONH VD and a negative correlation between IOP and changes in VD at weeks 1 and 4[26].The other recent study reported increased inside disc capillary density of ONH but similar peripapillary vascular density after cataract surgery[27].
To obtain detailed information on vascular changes in the ONH after cataract surgery, we evaluated the changes in the VD and retinal nerve fiber layer thickness (RNFLT) of the ONH using OCTA and examined other potentially correlated factors.
SUBJECTS AND METHODS
Ethical ApprovalThis prospective study included 34 eyes of 27 patients who underwent uncomplicated phacoemulsification and intraocular lens implantation surgery at the Eye Hospital of Wenzhou Medical University(Hangzhou, China) from November 2020 to May 2021.Informed consent was obtained from all patients.The research protocol conformed to the Declaration of Helsinki and was approved by the Office of Research Ethics of the Eye Hospital of Wenzhou Medical University.This study was registered with ClinicalTrials.gov (No.NCT01848288).The Ethics Committee of Wenzhou Medical University approved this study (No.2020-208-K-190).
Inclusion and Exclusion CriteriaThe inclusion criterion was a confirmed diagnosis of age-related cataract that affected vision and activities of daily living, necessitating phacoemulsification and IOL implantation surgery.The exclusion criteria were: presence of diabetes mellitus or systemic hypertension, presence of retinopathies that may result in abnormal microvasculature (e.g., age-related macular degeneration, diabetic retinopathy, and any other retinal vascular disorder), presence of any kind of glaucoma or ocular hypertension, presence of ONH pathologies (tilted disc, drusen, optic disc edema, atrophy,etc.), history of laser or photodynamic therapy or ocular surgery, and lack of cooperation for repeated measurements.
Each study participant underwent a comprehensive ophthalmic evaluation, including best-corrected visual acuity (BCVA)testing, IOP measurement using a non-contact specular microscope (Tomey, EM4000, GmbH, Germany), slit-lamp microscope examination, and fundus photography, using a color fundus camera (CR-2 AF, Canon, Japan).The opacity of each lens with a cataract was assessed using the LOCS III grading system.The fundus photographs were graded from 0 to 8 according to the degree of turbidity of the refractive medium[28].
Imaging ProtocolONH scans, measuring 4.5×4.5 mm2,were obtained using the AngioVue system (Optovue RTVue-XR Avanti; Optovue Inc., Fremont, CA, USA) at baseline and 3mo after phacoemulsification to evaluate the changes in the ONH vasculature.Three sets of scans were obtained in one visit, and the measurements with the highest quality score (QS) were used in the subsequent analysis.Images with a QS of less than 6 and with artifacts caused by excessive eye motion, blinks, and segmentation errors were excluded.
The radial peripapillary capillary (RPC) area was defined as the region between the inner ring (diameter, 2 mm) and outer ring (diameter, 4 mm), and the inner disc area was outlined by the disc margin, as automatically detected from Bruch’s membrane opening.VD was defined as the percentage of area occupied by the vessels.Since both capillary and large vessels were used to calculate the regional density in various disc sectors, we recorded both capillary and large vessel densities in the whole disc, inside the disc, and sectoral areas(superior and inferior hemi-fields and superior, inferior, nasal,and temporal quadrants).Capillary density was evaluated after excluding the arterioles and venules, using an automated software[29].Since the AngioVue system does not report the density of large vessels, we calculated it manually using the following formula: large VD=all VD–capillary VD.The average overall RNFLT and the mean RNFLT values of the four quadrants (superior, inferior, nasal, and temporal quadrants) were also measured.
Surgical TechniqueAll surgeries were performed by the same experienced surgeon (Zhao YE) under topical anesthesia.Phacoemulsification was performed using phaco-chop technique at a bottle height of 90 cm for gravity-fluidics, using the CENTURION Vision System (Centurion, Alcon Surgical,Fort Worth, Texas, USA).The aspiration flow rate was set at 45 mL/min, and vacuum pressure was set at 450 mm Hg.
Statistical AnalysisThis study was designed as a selfcontrolled test to demonstrate the changes in ONH vascular density after uncomplicated cataract surgery.Sample size calculations were conducted before starting the study.The effect size was calculated according to published data on inside-disc ONH VD changes and expert opinions[26].The sample size was calculated for two-tailed tests, with a type-I error of 5%, a power of 95%, and an estimated loss rate of 20%.The results indicated the need for 25 eyes.Ⅰf the effect size was calculated using the total or peripapillary VD changes,the result would have been 20 or 15 eyes.
Statistical analysis was performed using SPSS 19.0 (SPSS Inc., Chicago, IL, US).The Kolmogorov-Smirnov test was used to confirm normal distribution of the variables.Continuous data were expressed as means±SDs or as medians with range values.Comparisons between the included and excluded eyes were analyzed using a dependent samplet-test or Wilcoxon signed-rank test, whereas comparisons of preand postoperative data of the same eyes were made using the matched pairst-test or Wilcoxon signed-rank test.Spearman’s correlation analysis was used to demonstrate the correlation between RPC density changes and large VD changes in various sectors.The rate of VD change was calculated according to the sum of the VD before and 3mo after surgery divided by the preoperative VD.Correlations between the rate of VD change and QS change, postoperative BCVA, fundus photography grading, and postoperative peripapillary RNFLT were also assessed using Spearman’s correlation analysis.Statistical significance was set atP<0.05.
RESULTS
In this prospective study, 34 eyes of 27 patients were included in the final analysis (Figure 1).As presented in Table 1, 24 eyes were excluded because of inadequate preoperative image quality (QS: 3.53±1.1).There was a significant difference in preoperative BCVA between the included and the excluded eyes (0.43±0.16 and 0.71±0.08, respectively,P=0.002).The median LOCS III scores of the included eyes were C2, N2, and P2, which were less severe than those of the excluded eyes (C3,N2, P2).The fundus photography grades of the included eyes were significantly lower than those of the excluded eyes (2 and 4, respectively;P<0.001).No differences were found in age or sex between the two groups.
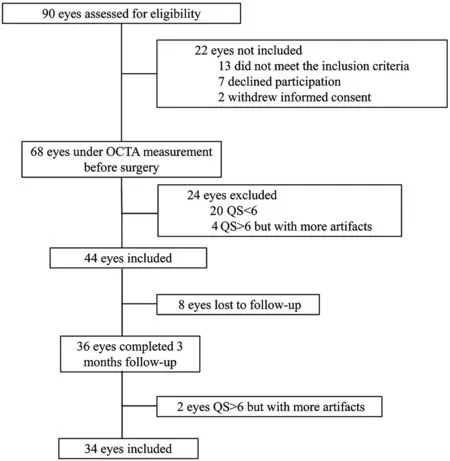
Figure 1 Study design flow diagram OCTA: Optical coherence tomography angiography; QS: Quality score.

Table 1 Comparison of characteristics in the included and the excluded patients before surgery
A follow-up analysis was conducted on the 34 included eyes.There were statistically significant improvements in the BCVA and QS after cataract surgery (allP<0.001), as shown in Table 2.The QS of postoperative scans had improved for all,except three eyes—the QS remained the same (QS=8) for two eyes, and it decreased from 9 to 8 for one eye.The mean preoperative IOP was 12.6±4.3 mm Hg, and no reduction in IOP was observed after surgery (P=0.987).

Table 2 Comparison of pre- and post-operative different parameters in the included eyes
The inside-disc RPC density of the ONH showed a statistically significant increase at postoperative month 3 (47.5%±5.3%)compared to the preoperative density (50.2%±3.7%,P=0.007;Table 2, Figure 2).All VD of the inside-disc area showed a significant increase to 60.47%±3.10% (P=0.001) from the preoperative VD of 57.87%±4.30%.In terms of large VD,an increasing pattern was observed in peripapillary areas(both superior hemi-field and inferior hemi-field, allP<0.05).However, decreased RPC density was found in the inferior and superior quadrants (from 52.8%±4.7% to 51.0%±4.2%and from 51.1%±4.2% to 49.2%±3.6%,P=0.019 and <0.001,respectively).There was no difference in average ONH vascular densities of the peripapillary regions.The average RNFLT increased from 108.7±12.8 μm to 111.7±11.6 μm (P<0.001),and the mean sectoral RNFLTs in the four quadrants also increased 3mo after surgery (allP<0.05).
Table 3 shows the correlation between the change in RPC density and large VD.There was a moderately negative correlation between the change in RPC density and a large VD in the inside-disc area, superior hemi-field, and inferior hemifield (r=-0.419, -0.370, and -0.439;P=0.017, 0.044, and 0.015,respectively).
The correlation analyses of the measurement parameters are presented in Table 4.There were no statistically significant correlations between the rate of change in RPC and all other parameters including QS change, fundus photography grading,postoperative BCVA and postoperative peripapillary RNFLT(allP>0.05).Similarly, no statistically significant correlations were established between these parameters and all inside-disc VD (allP>0.05).
DISCUSSION
Many studies have reported that noninvasive OCTA, which entails a convenient image acquisition process and the capacity to quantify biometric indices, could be widely used in ocular pathology detection.In the current study, we compared the changes in ONH VD, including capillaries, all vessels, and large vessels, before and after uncomplicated cataract surgery, to identify a potential correlation between VD change and other parameters.
Since the image quality of OCTA was affected by signal strength and artifacts, we excluded images with poor scan quality (QS of <6) and manually excluded images with noticeable artifacts.The included participants had early/moderate-stage cataracts or media opacities.Our followup time point was set at 3mo after surgery primarily for the following reasons: 1) the OCTA image quality may be disrupted by surgery-induced corneal edema 1d and 1wk aftersurgery; 2) postoperative inflammation almost diminishes after 3mo of recovery; 3) previous studies showed an increasing trend of VD, but did not address whether it would minimize to the preoperative level[26].
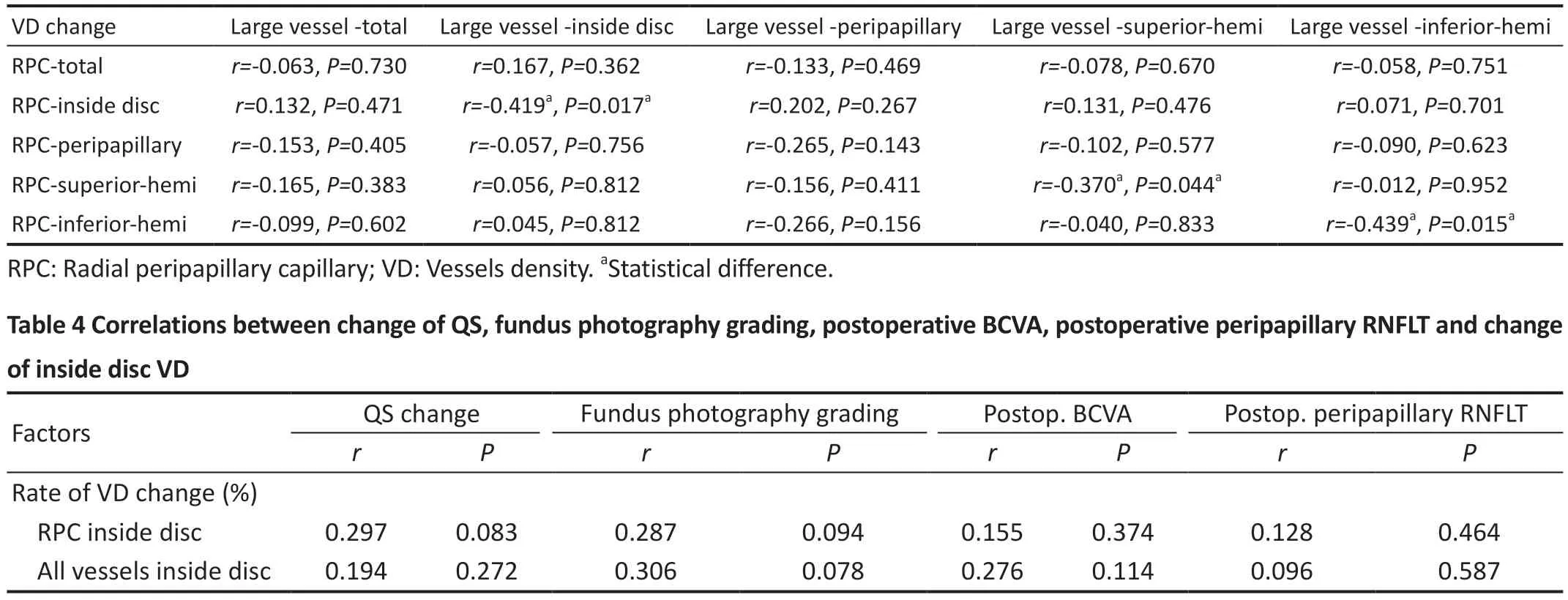
Table 3 Correlations between RPC density change and large VD change
Cataract surgeons closely monitor the IOP throughout the entire cataract procedure, which may temporarily increase to above 60 mm Hg—the retinal artery perfusion pressure.While increases in IOP are usually temporary, the long-term impact of elevated IOP could surpass perfusion pressure,leading to a decrease in ocular blood flow and causing harm to the ONH[6].Many cataract patients who have been diagnosed with optic nerve pathologies such as glaucoma and atrophic optic nerve are at a higher risk of experiencing optic nerve damage during surgery.In addition, two large data studies conducted in South Korea and the USA have both reported an increased risk of anterior ischemic optic neuropathy in healthy eyes following cataract surgery[8,30].However, current theories cannot clearly explain the pathogenesis and require further investigation.
In the present study, the VD of the capillaries and all the vessels in the peripapillary ONH region were similar at pre- and postoperative stages.The postoperative increase in RPC density and overall VD was observed only inside the optic disc compared to the preoperative value.Few studies have evaluated VD changes in the ONH region after cataract surgery[22,26,31].Zhouet al[22]found that the increase in peripapillary VD lasted for 1mo after cataract surgery.Karabulutet al[26]reported an increase in VD in the total, inside-disc, and peripapillary ONH regions 4wk after cataract surgery using the AngioVue system; however, there was no difference between in the values at baseline and 1-week follow-up visit.The difference between our results and those listed above may be due to the different time points of the follow-up visits.A recent study by Tanet al[31]showed similar postoperative peripapillary VD compared to preoperative value between Ⅰnfiniti system and Centurion phacoemulsification system 3mo after cataract surgery.We found several studies that focuses on macular vasculature changes, most of which revealed an increasing trend in the density of macular vessels after cataract surgery.However,the time point is still key.Jiaet al[25]observed a gradual increase in macular blood flow during the first month after cataract surgery in normal Chinese people, but Pilottoet al[11]reported that macular perfusion nearly reached the baseline level 3mo after surgery.Cataract surgery might induce bloodaqueous barrier breakdown and stimulate the release of inflammatory cytokines; the inflammatory response might still exist 3mo postoperatively, considering that in our patients, the inside-disc area seemed more sensitive than the peripapillary region of the ONH.
Large vessels were automatically identified by thresholding theen facemean projection of OCT reflectance, and the capillary density was computed after excluding these large vessels[29].Using the algorithm built into the AngioVue system, we calculated the large VD and found an increased value of large VD in the peripapillary ONH region.However,RPC density in the superior and inferior quadrants was significantly lower 3mo after cataract surgery, contrary to our expectation.Notably, the VD value offered by OCTA did not equate to the absolute VD density.Our results demonstrated a negative correlation between RPC density and large VD changes in the superior and inferior hemi-fields.Considering the above mentioned facts, we propose the following hypothesis: some large vessels were identified as capillaries automatically by the OCTA algorithm owing to lens opacity and re-identified as large vessels after lens extraction.The superior and inferior quadrants had higher densities of arterioles and venules than the nasal and temporal quadrants,so a false decrease in the RPC density was observed in the former two quadrants.To our knowledge, this is the first study to consider RPC density, including all vessels,even large ones.Our study may also help remind clinical ophthalmologists and other researchers of the difference between reported data and actual fundus vascular density.
Previously, axial length, age, and IOP were considered to be the factors affecting fundus blood flow[32].In the current study,the increasing ONH RPC density and overall VD could not be explained by these three factors, as they were the same before and after surgery.In previous studies, OCTA measurements were strongly correlated with image quality; even mild-tomoderate cataracts had an influence on the vessel images.Studies have shown that media opacity influences OCTA scan quality, leading to underestimation of VD[22,33].We attempted to determine the correlation between VD change and other parameters but found no statistically significant correlations between QS change, fundus image grade, postoperative BCVA, and changes in both RPC density and overall VD,with one of the reasons being the small sample size.Another reason could be that some inflammatory factors increase blood flow even 3mo after surgery.
It is universally known that RNFLT increases after cataract surgery[22,34-35], which was observed in the present study.A positive correlation between RNFLT and VD in the general population has been established in previous studies[36-37].However, in our correlation analysis of the association between VD change and postoperative RNFLT, we found no significant correlation.This finding could be attributed to postoperative inflammation.We know that the trauma of surgery leads to the disorder of cellular energy metabolism,which causes an increase in free radicals and prostaglandin levels, subsequently damaging the aqueous humor barrier,leading to the aggregation of inflammatory factors in the aqueous humor and vitreous cavity.This might have been due to the high sensitivity of glial cells, such as perivascular Müller cells, to inflammatory factors, which increase the permeability of the vessels in the corresponding retinal localization[22].The current study included follow-up examinations 3mo after surgery because we assumed that the inflammatory reaction would have reduced to a relatively low level by that time; however, the duration of the inflammatory response induced by cataract surgery remains unclear.
We acknowledge the following study limitations: 1) The postoperative measurements were recorded only at 3mo; thus,the long-term trend of VD changes could not be determined;2) Data on surgical parameters, such as cumulative dissipated energy, aspiration time, and fluid usage, were not collected.The correlation between surgical parameters and VD changes remains unclear.However, with an experienced surgeon and in the cases of mild-to-moderate cataracts, these factors may have little impact; 3) The data of VDs in the total and peripapillary regions and superior and inferior hemi-fields of the ONH were limited.
In conclusion, in patients with mild-to-moderate cataracts and image QS of not less than 6, the 3-month-postoperative RPC density and overall VD in the peripapillary ONH region were similar to their respective preoperative values, except for the inside-disc area, which exhibited an increase in these values.The decreased RPC density in the superior and inferior hemi-fields may not be clinically meaningful, which barely correlated with an increased large VD.
ACKNOWLEDGEMENTS
Foundation:Supported by Natural Science Foundation of Zhejiang Province (No.LQ19H120001).
Conflicts of Interest:Zhu ZH, None; Zhao YY, None; Zou R,None; Zou H, None; Fang JY, None; Chang PJ, None; Zhao YE, None.
 International Journal of Ophthalmology2023年6期
International Journal of Ophthalmology2023年6期
- International Journal of Ophthalmology的其它文章
- Preliminary proteomic analysis of human tears in lacrimal adenoid cystic carcinoma and pleomorphic adenoma
- Assessment of the effects of intrastromal injection of adipose-derived stem cells in keratoconus patients
- Stability of neodymium:YAG laser posterior capsulotomy in eyes with capsular tension rings
- Comparison of the efficacy and safety of ultrasonic cycloplasty vs valve implantation and anti-VEGF for the treatment of fundus disease-related neovascular glaucoma
- Volumetric fluid analysis of fixed monthly anti-VEGF treatment in patients with neovascular age-related macular degeneration
- Time in range as a useful marker for evaluating retinal functional changes in diabetic retinopathy patients