
Recent advancements in noninvasive brain modulation for individuals with autism spectrum disorder
2023-01-21 04:42JessicaGriffJakeLanglieNathalieBencieZacharyCromarJeenuMittalIdilMemisStevenWallaceAlexanderMarcilloRahulMittalAdrienEshraghi
中国神经再生研究(英文版) 2023年6期
Jessica R.Griff,Jake Langlie,Nathalie B.Bencie,Zachary J.Cromar,Jeenu Mittal,Idil Memis,Steven Wallace,Alexander E.Marcillo,Rahul Mittal,Adrien A.Eshraghi,,
Abstract Autism spectrum disorder is classified as a spectrum of neurodevelopmental disorders with an unknown definitive etiology.Individuals with autism spectrum disorder show deficits in a variety of areas including cognition,memory,attention,emotion recognition,and social skills.With no definitive treatment or cure,the main interventions for individuals with autism spectrum disorder are based on behavioral modulations.Recently,noninvasive brain modulation techniques including repetitive transcranial magnetic stimulation,intermittent theta burst stimulation,continuous theta burst stimulation,and transcranial direct current stimulation have been studied for their therapeutic properties of modifying neuroplasticity,particularly in individuals with autism spectrum disorder.Preliminary evidence from small cohort studies,pilot studies,and clinical trials suggests that the various noninvasive brain stimulation techniques have therapeutic benefits for treating both behavioral and cognitive manifestations of autism spectrum disorder.However,little data is available for quantifying the clinical significance of these findings as well as the long-term outcomes of individuals with autism spectrum disorder who underwent transcranial stimulation.The objective of this review is to highlight the most recent advancements in the application of noninvasive brain modulation technology in individuals with autism spectrum disorder.
Key Words: autism spectrum disorder;behavior;cognition;neurostimulation interventions;noninvasive brain modulation;theta burst stimulation;transcranial direct current stimulation;transcranial magnetic stimulation
From the Contents
Introduction 1191
Search Strategy and Selection Criteria 1191
Transcranial Magnetic Stimulation 1191
Transcranial Direct Current Stimulation 1192
Theta Burst Stimulation 1193
Currently Funded Clinical Trials 1193
Conclusion and Future Directions 1194
Introduction
Autism spectrum disorder (ASD) is a spectrum of neurodevelopmental disorders characterized by social communication deficits and repetitive sensory-motor behaviors (Lord et al.,2018).The other associated features include abnormal responses to sensory stimuli,speech and language difficulties,and lack of social adaptation (Lord et al.,2018).It is estimated to affect approximately 1.5% of the population of developed countries (Lyall et al.,2017).The pathophysiology of ASD is complex and not fully understood but has been shown to have brain reorganization beginning during early childhood development.Neuroimaging studies have found that there is a pattern of overgrowth of brain volume,leading to brain underconnectivity in some regions coupled with over-connectivity within other regions (Anteraper et al.,2020;May and Kana,2020;Kim et al.,2021;Mann et al.,2021;Zhao et al.,2021).It is therefore hypothesized that the underlying etiology of ASD may be related to aberrant neuroplasticity (Courchesne et al.,2011;Desarkar et al.,2015;Wallace et al.,2015).
Treatments for children with ASD are primarily targeted towards behavioral interventions and improving sensory and motor skills (Schreibman et al.,2015;Weitlauf et al.,2017).However,in the last two decades,with greater understanding of the pathophysiology,therapeutic approaches aimed at reversing underlying neuroplasticity defects have been studied in the context of neuropsychiatric disorders including ASD.
These noninvasive brain stimulation techniques work in the following ways:transcranial magnetic stimulation (TMS) and repetitive transcranial magnetic stimulation (rTMS) induce changes in plasticity via a current passed through a wire coil generating a magnetic field that passes through the skull (Yang et al.,2020;Xie et al.,2021;Chang et al.,2022;Eldaief et al.,2022;Huang et al.,2022;Ward et al.,2022).These magnetic fields produce small electrical currents,which thereby activate neurons to release neurotransmitters.A modification to the rTMS is theta burst stimulation (TBS) which has been performed in different sequences including intermittent TBS (iTBS) and continuous TBS (cTBS) (Ding et al.,2022;Knehans et al.,2022;Mehta et al.,2022).TBS delivers rapid stimuli at lower intensities than TMS as well as shorter duration therapy sessions.Another mode of noninvasive brain stimulation includes transcranial direct current stimulation (tDCS),which applies weak electric currents passed through two electrodes instead of a coil,modulating resting membrane potentials and inducing neuronal excitability or decreasing excitability (Hodaj et al.,2022).
The objective of this review article is to discuss the most current literature regarding the utilization of different types of noninvasive brain stimulation technologies in individuals with ASD (Additional Table 1).It will also provide an overview of previous and ongoing clinical trials regarding the implications of TMS in ASD (Additional Table 2).We will highlight the recent advances in noninvasive brain stimulation in the treatment of ASD as new evidence demonstrates the therapeutic capabilities of this technology in both behavior and cognitive domains.
Search Strategy and Selection Criteria
A PubMed literature search was conducted using the keywords “rTMS”,“transcranial magnetic stimulation”,“TBS”,“theta burst stimulation,” “tDCS,”“transcranial direct current stimulation,” “autism spectrum disorder,” and“neurostimulation interventions.” Abstracts published between January 2017 and April 2022 were reviewed with original interventional research studies selected for inclusion.Articles’ reference lists were screened to locate additional articles.In addition,current clinical trials were found on ClinicalTrials.gov using the same keywords which yielded 29 relevant interventional studies with primary and secondary outcome measures.
Transcranial Magnetic Stimulation
Procedures of TMS
Nine recent studies found in the literature evaluated the effects of TMS on behavioral and cognitive dimensions in individuals with ASD.This procedure involves the generation of magnetic fields that penetrate the skull and induce neurons to fire action potentials (Figure 1;Chang et al.,2022;Eldaief et al.,2022).Specifically,repetitive TMS (rTMS) involves short,consistent frequency pulses applied over various portions of the cranium.The areas of brain stimulation include the dorsolateral prefrontal cortex (DLPFC),which plays a role in executive functions including working memory,planning,and abstract reasoning,and the inferior parietal lobe,which helps in the processing of emotions and language (Yang et al.,2019;Ambrus et al.,2020).Studies varied in the number of sessions and frequency of stimulation they used.For example,Casanova et al.(2020) treated patients with 1.0 Hz for 18 weekly sessions whereas Assadi et al.(2020) used 10 Hz 3 days per week for 3 weeks straight.Many different measurements were used to quantify the changes in behavior and cognition such as alpha and gamma waves with electroencephalogram (EEG) and the Aberrant Behavior Checklist (ABC).
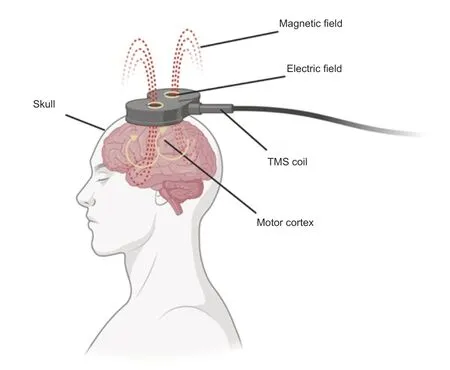
Figure 1|A schematic representation of transcranial magnetic stimulation (TMS).
Behavioral effects of TMS
The behavioral effects of TMS treatment were measured,largely based on the decrease of repetitive behaviors and modulation of characteristic symptoms of autism,such as decreased attentive capacity.An early study by Sokhadze(2017) showed that rTMS may induce neuromodulation by increasing parasympathetic tone,which has been associated with less repetitive behaviors.This study concluded that decreasing sympathetic arousal indices has a positive correlation with repetitive and stereotypical behaviors of autism.In a follow-up study by Sokhadze et al.(2018),children with ASD were stratified into control and experimental groups where the experimental groups received rTMS stimulation over the DLPFC for 6-,12-,and 18-week time courses.There was a significant improvement in motor response answers and a significant reduction in aberrant behavior ratings in both repetitive and stereotypical behaviors.Further,behavioral changes improved with an increasing number of sessions,finding that 18 sessions best facilitate cognitive control and attention (Sokhadze et al.,2018).
In addition to eliciting improvements shortly after TMS treatment,TMS has also shown promise as being a potentially long-lasting treatment for ASD.Gomez et al.(2017) demonstrated that noninvasive brain stimulation via rTMS for children 11–13 years of age significantly improved autistic symptoms,with results lasting for 6 months at follow-up with minimal degradation.These results highlight the possibility of lasting therapeutic effects of TMS on changing neuroplasticity in children with ASD.Studies with longer followup intervals are needed to fully establish the long-term effects of TMS on behavior modulation.
One of the biggest behavioral deficiencies in individuals with ASD is their reduced attention capacity.A study by Casanova et al.(2020) compared the effects of rTMS with 19 children with ASD matched to 19 age-matched neurotypical children.Researchers measured a significant reduction in gamma oscillations after treatment.Gamma waves play a role in attention selection and memory operations,so in context with this study,researchers deduced that rTMS can have an impact on improving attention capacity and memory(Casanova et al.,2020).In the experimental group with adolescents with ASD,the study also showed decreased scores in irritability and hyperactivity,signs that are often elevated in children with ASD (Casanova et al.,2020).
Cognitive effects of TMS
Cognitive deficits in ASD,including altered social behaviors,learning difficulties,and memory deficits,are common presenting symptoms of ASD and are often extremely challenging for those with ASD to overcome.Desarkar et al.(2021) studied the effects of rTMS on overall brain plasticity.In the first phase of the study,researchers compared long-term potentiation and long-term depression,two prototypes for plasticity,in individuals with ASD to neurotypical controls.Their results supported the understanding that those with autism have atypical plasticity.After an experimental group of individuals with ASD underwent a single treatment with rTMS,there was a significant change in long-term depression but no change in long-term potentiation.Researchers concluded that indeed there is a difference in hyperplasticity between individuals with ASD and neurotypical subjects,which can serve as an area of research for brain stimulation to correct for those differences(Desarkar et al.,2021).A study with children with low-functioning ASD who underwent rTMS treatment showed significant increases in the peak alpha frequency,a measure of cognitive preparedness,and a possible neural marker of cognitive function of autism in the frontal region,left and right temporal region,and the occipital region (Kang et al.,2019).
There have also been improvements in linguistics when the left inferior parietal lobe was targeted as well as resolution of social symptoms,imitation,and cognition (Yang et al.,2019;Assadi et al.,2020).Considering these cognitive disabilities are hard to overcome even with psychological therapy,it is important to recognize the potential value of rTMS since individuals were able to maintain improvements through the six-week follow-up period (Yang et al.,2019).Another study determined that expanding the region of stimulation can have an even greater effect on cognitive function.They targeted seven main brain regions (frontal,vertex,right and left temporal,right and left parietal,and occipital),and beta rhythm with magnetoencephalography was measured (Anninos et al.,2019).Beta rhythms are often associated with active,busy,or anxious thinking and active concentration (Anninos et al.,2019).A change in beta rhythms was noted in all subjects,and patients showed improvements in their clinical and cognitive symptoms (Anninos et al.,2019).These findings suggest the beneficial effect of rTMS treatment on cognitive function in ASD individuals.
Transcranial Direct Current Stimulation
Procedures of tDCS
tDCS is a similar approach to rTMS but involves the passage of electric current through the brain rather than a magnetic field (Figure 2).This technique can modulate neuronal membrane potentials,which modulates cortical tissue excitability (Woods et al.,2016;Hodaj et al.,2022).tDCS does not directly induce activity in resting neural networks,but instead,modulates spontaneous neuronal activity (Fritsch et al.,2010;Chase et al.,2020).tDCS involves the application of low current stimulation,often in the range of 1–2 mA via electrodes to the scalp (Kenney-Jung et al.,2019).The low voltage has been shown to alter the threshold of cortical neuronal firing,such that neurons near the anode (positive lead) become more likely to fire,and neurons near the cathode (negative lead) become less likely to fire (Nitsche et al.,2008;Amatachaya et al.,2014).When comparing efficacy between rTMS and tDCS,Gomez et al.(2017) found no significant difference in outcome measurements of treatment groups 6 months after stimulation treatment.
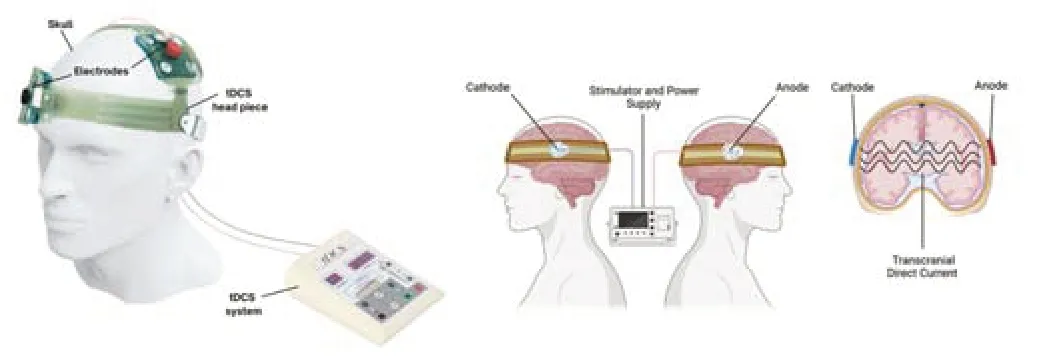
Figure 2|Topographical representation of transcranial direct current stimulation(tDCS).
Multiple measurement scales have been proposed to calculate the neuromodulation induced by tDCS.The ABC and Childhood Autism Rating Scale can be used to evaluate autism severity at baseline of treatment and at follow-up after tDCS treatment (Amatachaya et al.,2014).The Autism Treatment Evaluation Checklist evaluates the effectiveness of the treatment from the viewpoint of the caregiver (Geier et al.,2012).To measure a child’s psychosocial function,a proxy of cognitive ability,the Children’s Global Assessment Scale was used.Common autistic behaviors were measured through the Autism-Spectrum Quotient questionnaire,a measure of autism spectrum traits.The Test of Adolescent Social Skill Knowledge can be used to test social skills while a verbal fluency test can be utilized to assess language capabilities.
To modulate neuroplasticity and induce observable behavioral changes,the temporoparietal junction,which plays a role in social functioning,and the inferior frontal gyrus were stimulated (Bitsch et al.,2018).Cognitive function is targeted through the DLPFC and the anterior cingulate cortex,which functions in many physiological roles including blood pressure and heart rate monitoring,and the amygdala,which assists in the interpretation of fear and emotion.Researchers also looked at the inferior frontal cortex,which functions in the processing of speech and language in Broca’s area,to see if language modulation was possible (Dick et al.,2019).Finally,to measure motor effects,researchers have stimulated the primary motor cortex,which functions in the production of skilled and fine movements (Dick et al.,2019).
Behavioral effects of tDCS
To observe the potential and various modulating effects of tDCS through the aforementioned procedures,researchers proposed a study in which stimulated the right temporoparietal junction or the inferior frontal cortex.Nobusako et al.(2017) observed that there was an immediate increase in imitation inhibition and perspective taking.This modulation of behavior and cognition was a significant finding and long-term follow-up should be initiated to determine if the treatment is still beneficial over time.
Mahmoodifar and Sotoodeh (2020) investigated changes in motor skills.All children practiced motor training to improve balance skills,and the experimental group also received tDCS stimulation.Results showed that both groups had significant positive impacts on balance (Mahmoodifar and Sotoodeh,2020).In addition,participants who received both tDCS and motor skill training performed significantly better than those who only received motor skill training (Mahmoodifar and Sotoodeh,2020).The combination of brain stimulation and motor exercises seems to show a great potential for improving motor performance in children with ASD.Hadoush et al.(2020)expanded upon these findings by demonstrating an improvement in Autism Treatment Evaluation Checklist scores.These changes correlated with a decline in autistic symptoms in the treatment group with no significant change in the control group (Hadoush et al.,2020).D’Urso et al.(2021) in an open-label pilot study of 7 individuals with ASD showed a 25% mean reduction in global severity of symptoms derived from the ABC after receiving daily sessions of right cerebellar lobe stimulation.Interestingly as well,this study highlights the reduction in the severity of tics in a patient with ASD and a concurrent tic disorder (D’Urso et al.,2021).These multiple studies suggest that tDCS can have a significant effect on modulating motor and behavioral skills.
A subsequent study measured the changes in brain metabolites before and after ten individuals with ASD received tDCS for 5 consecutive days.Researchers found significant changes in several metabolites(N-acetylaspartate,myoinositol,and choline) which positively correlated to improvement in the social subsection of Autism Treatment Evaluation Checklist (Auvichayapat et al.,2020).These findings suggest that the observed behavioral changes are due to changes in neuronal signaling,elucidating some of the physiology underlying tDCS stimulation.
In addition to proposed changes in neurochemicals,researchers have also observed changes in EEG readings after receiving tDCS that reflect readings that are similar to those of neurotypical subjects.Mismatch negativity (MMN)is the measurement of waveform changes from auditory event-related potentials which have been shown to be decreased in individuals with ASD.Sun et al.(2022) found that after receiving tDCS,individuals with ASD had a decrease in MMN latency and an increase in MMN amplitude which is more in line with average MMN measurements.These EEG changes also correlated with changes in the ABC scale.However,there were no statistical differences between the experimental and control groups after 1 month (Sun et al.,2022)indicating the modulations have a brief therapeutic effect.
Cognitive effects of tDCS
As cognitive deficits commonly plague children with ASD,studies have been performed to determine the effect of tDCS in modifying and improving cognition.Kang et al.(2018,2022) and Zhou et al.(2020) measured changes in EEG,mapping increased brain complexity,and the reconfiguration of dynamic network communities.English et al.(2018) provided evidence for the modulation of attention deficits through right-hemisphere stimulation in low-functioning individuals with ASD.Esse Wilson et al.(2018a) captured positive changes in verbal fluency but did not see a difference in social behaviors between those treated with tDCS and those in the control group at first.To further evaluate changes in social behaviors,Esse Wilson et al.(2018b)presented a case study of an 18-year-old,high-functioning ASD patient who underwent tDCS treatment to improve social behaviors.Immediately after treatment,the patient showed improvement in social functioning and increased interest in social interactions,which was maintained at a 2-month follow-up.The patient’s anger and frustration over social disappointments had also markedly decreased during immediate follow-up.In a larger study on the effects of tDCS on social cognition,Donaldson et al.(2018) showed that there is a complex relationship between individual social traits and the neurological changes induced by tDCS.Differences caused by cathodal and anodal stimulation on Autism Spectrum Quotient Switching and Social scores were analyzed.Researchers concluded that the interventions may have opposing outcomes depending on initial levels of individual Autism-Spectrum Quotient domain scores (Donaldson et al.,2018).These studies demonstrate the possibility for cognitive and social improvement with tDCS treatment;however,it is difficult to deduct conclusive evidence from isolated case reports and small cohort studies.
Theta Burst Stimulation
Procedures of TBS
Intermittent TBS (iTBS) is another TMS technique that has been tested in the context of neuromodulation and improvement of ASD symptoms.iTBS is a patterned repetitive transcranial magnetic stimulation,which has been shown to have success in long-term potentiation effects of cortical excitability(Figure 3;Desforges et al.,2022;Mao et al.,2022;Pabst et al.,2022).When comparing TBS to rTMS,TBS is able to produce 20 minutes of suppressive effects after only a 20-second span of uninterrupted bursts,equating to 300 pulses (Li et al.,2014).Therefore,this methodology is potentially more convenient for patients receiving brain stimulation treatments.
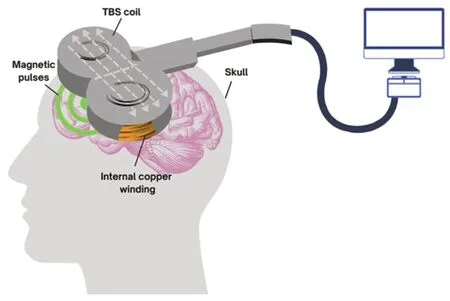
Figure 3|A schematic representation of theta burst stimulation (TBS).
Behavioral effects of TBS
As iTBS is a relatively new treatment,there have been mixed results reported.Abujadi et al.(2018) stimulated the right DLPFC using iTBS and showed improvement in obsessive-compulsive behaviors,reduced errors on the Wisconsin Card Sorting Test,and reduced time in the Stroop test.The results indicate that iTBS might be effective in mitigating some of the neurological deficits of ASD (Abujadi et al.,2018).However,it is impossible to draw definitive conclusions from this study because of the small sample size (n=10) with no randomization.There was also no neurophysiological correlate examined,so there is no quantification of physiologic changes in the brain due to iTBS treatment.A second study used iTBS to target the posterior superior temporal sulcus or bilateral DLPFC but found no significant improvements in Wisconsin Card Sorting Test (Ni et al.,2017).More recently,Ni et al.(2021)used iTBS over the bilateral posterior superior temporal sulci in adults with ASD and found an immediate change in parent-rated Autism Spectrum Quotient scores.However,researchers acknowledged that variations in baseline impairments and medications might have impacted the results (Ni et al.,2021).Differences in methodology could explain the varied results among these studies.There is limited data on iTBS in ASD,which emphasizes the need to further evaluate the efficacy of this technique in this patient population.
Currently Funded Clinical Trials
The overwhelming positive reports of various noninvasive technologies in individuals with ASD published in the literature have prompted an increase in clinical trials designed to further investigate the potential therapeutics related to TMS,DCS,and TBS to improve the lives of those with ASD and their caregivers.A search on this topic on ClinicalTrials.gov yielded 29 interventional studies with primary and secondary outcome measures designed to evaluate behavior and cognitive modulation of ASD with noninvasive brain stimulation(Additional Table 2).Out of the 29 studies,there are 7 crossover studies,7 single group assignment studies,and 14 parallel assignment studies.The studies range from no blinding (10/29) to quadruple blinding.All 29 studies have autism as an inclusion diagnosis and seven include another condition as well.The interventional techniques across trials vary: TMS (5/29),tDCS (9/29),rTMS (12/29),cTBS (1/19),and iTBS (2/29).
The outcomes of the trials were categorized into four broad categories–social deficits,behavioral deficits,cognitive deficits,and emotional deficits.The clinical trials were all similar in their goal of modulating abnormal behavior and cognition associated with ASD;however,they greatly differ in their protocols and outcome measurements.The most frequently reported outcome measures were functional magnetic resonance imaging (7/29),the Social Responsiveness Scale (7/29),and the ABC (4/29).Unfortunately,the fundamental differences of each trial do not allow for direct comparison of results among other trials limiting corroboration of results.A more standardized approach would be beneficial as it would allow for a greater understanding of the therapeutic capabilities of each stimulation technique which will ultimately benefit those with ASD and their caretakers.Many trials are also in their beginning phases.Published results from trials are limited considering the novelty of noninvasive brain interventions in individuals with ASD.
One randomized pilot study (NCT02311751) used rTMS and measured changes in executive functioning through the Cambridge Neuropsychological Test Automated Battery Spatial Working Memory tasks and Behavior Rating Inventory of Executive Functioning.Individuals with severe functioning deficits in the experimental group demonstrated improved executive functioning when compared to the sham group (Ameis et al.,2020).These preliminary results highlight the feasibility and acceptability of rTMS in the treatment of working memory performance.Another interventional pilot study (NCT02939560) studied the effectiveness of rTMS on alleviating depressive symptoms in adults with Major Depressive Disorder and ASD measured with the Hamilton Depression Rating Scale as well as reducing core symptoms of ASD and changes in brain connectivity.Researchers found a remarkable reduction in depressive symptoms and some improvement in core autism symptoms (Gwynette et al.,2020).Most clinical trials on this topic are underway and results are not publicly available. From the data that has been published,results have demonstrated positive changes in several domains of symptoms of ASD.Long-term studies are awaited to see how these modulations changed over time.
There are published trials on the clinical effects of transcranial stimulation in individuals with ASD being completed on an international scale.Prillinger et al.(2021) have published a study protocol that will investigate the psychological and behavioral changes in male adolescents with ASD who undergo 10 sessions of tDCS over the left prefrontal cortex.A pilot study from China found significant score reductions in Childhood Autism Rating Scale and the Children’s Sleep Habits Questionnaire when subjects underwent tDCS treatments to the DLPFC for 3 weeks (Qiu et al.,2021).However,a pilot study in New Zealand looked at adolescents and young adults with ASD who underwent high-definition-tDCS over the right ventrolateral prefrontal cortex and no significant changes in cognitive flexibility or behaviors (Parmar et al.,2021).
Conclusion and Future Directions
Overall,the various noninvasive brain stimulation modalities which have been explored in this article show great promise as possible neuromodulators for the treatment of ASD symptoms.Preliminary results from randomized pilot studies suggest that there are many positive effects,which warrant the continuation and development of more trials to fully understand the therapeutic nature of noninvasive brain stimulation in individuals,both children and adults,with ASD.
There are no standardized protocols for administering the various brain stimulating technologies,including the location of stimulation,and there are also no uniform outcome measures amongst studies making it impossible to compare methods and results directly.Nevertheless,the multitude of stimulation protocols and tracked outcome measures indicate that there is a wide realm of possible treatments for the variable expressivity of ASD symptomatology.In addition,studies published thus far have small sample sizes with minimal follow-up.To recognize the true benefits of noninvasive brain stimulation in individuals with ASD,all of the above criteria need to be met which will enable researchers to corroborate their findings.
From the perspective of the patients,it is important for these treatments to be as accessible as possible.Protocols that require daily treatments for extended periods may act as a barrier for patients and their families to receiving the proper brain stimulation.Therefore,keeping the patients’ best interests at the forefront can serve to guide the research of treatments for ASD.In addition,efforts should be done to reduce the costs associated with noninvasive brain modulation enhancing accessibility so that more patients can benefit from this technology.
Acknowledgments:We are grateful to Dr.Valerie Gramling (College of Arts and Sciences,University of Miami,Miami,FL,USA) for critical reading of the manuscript.
Author contributions:All authors contributed to conceptualizing,writing,reviewing,editing and proofing the manuscript,and approved the final version of the manuscript.
Conflicts of interest:The authors declare no conflicts of interest.
Availability of data and materials:All data generated or analyzed during this study are included in this published article and its supplementary information files.
Open access statement:This is an open access journal,and articles are distributed under the terms of the Creative Commons AttributionNonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.
Additional files:
Additional Table 1:A summary of recent studies using noninvasive brain stimulation in individuals with autism spectrum disorder.
Additional Table 2:A summary of clinical trials investigating the effects of noninvasive brain stimulation in individuals with autism spectrum disorder.
- 中国神经再生研究(英文版)的其它文章
- Neuro faces of beneficial T cells: essential in brain,impaired in aging and neurological diseases,and activated functionally by neurotransmitters and neuropeptides
- Profiling neuroprotective potential of trehalose in animal models of neurodegenerative diseases:a systematic review
- Cdk5 and aberrant cell cycle activation at the core of neurodegeneration
- Vicious cycle of lipid peroxidation and iron accumulation in neurodegeneration
- Cell-based therapeutic strategies for treatment of spinocerebellar ataxias: an update
- Do tau-synaptic long-term depression interactions in the hippocampus play a pivotal role in the progression of Alzheimer’s disease?