
Clinical observation of acupuncture combined with sitting-position knee-adjustment manipulations for patellofemoral arthritis
2022-12-28 07:53:08ZHANGKaiyong张开勇Peng刘鹏XUSiwei徐斯伟ZHANGBimeng张必萌ZHANHongsheng詹红生
ZHANG Kaiyong (张开勇), LⅠU Peng (刘鹏), XU Siwei (徐斯伟), ZHANG Bimeng (张必萌),ZHAN Hongsheng (詹红生)
1 SHⅠ’s Center of Orthopedics and Traumatology, Shuguang Hospital, Shanghai University of Traditional Chinese Medicine,Shanghai 201203, China
2 Ⅰnstitute of Traumatology & Orthopedics, Shanghai Academy of Traditional Chinese Medicine, Shanghai 201203, China
3 ZHAN Hongsheng Shanghai Famous Traditional Chinese Medicine Experience Research Studio, Shanghai 201203, China 4 Shanghai General Hospital, Shanghai 200080, China
Abstract
Keywords: Acupuncture Therapy; Manual Therapies; Tuina: Massage; Pain Measurement; Visual Analog Scale;Osteoarthritis, Knee; Patellofemoral Osteoarthritis
Knee osteoarthritis (KOA) is a widespread degenerative joint disease in the middle-aged and aged population. Its pathological features mainly include hyperostosis in the tibiofemoral and patellofemoral joints, subchondral bone degeneration, synovial proliferation, ligament laxity or contracture, and muscle atrophy[1]. KOA can be classified into three types, i.e.,simple tibiofemoral osteoarthritis (TFOA), simple patellofemoral osteoarthritis (PFOA), and a mix of the two. Due to the crucial mechanical role of tibiofemoral joint, the existing literature focuses more on TFOA,while the clinical study of PFOA is relatively lagging.Nevertheless, investigations have revealed a high prevalence and increasing incidence of PFOA among the aged[2-3]. For example, in China, almost 1/4 of the people aged over 50 years have PFOA, and the incidence is higher in females than in males[4].
PFOA usually happens before TFOA, and over half of those who suffer from knee pain have PFOA.Nevertheless, prompt treatment reduces KOA’s incidence[5].
Acupuncture can alleviate knee pain and improve knee joint motor function, with efficacy lasting for more than six months[6-9]. Besides, acupuncture can accelerate topical blood circulation, raise the pain threshold, and boost the healing of injuries[10-11].Knee-adjustment manipulations in a sitting position have been found effective in improving muscles around the knee joint and ligament balance, correcting force line, promoting blood circulation, and enhancing joint mobility in KOA[12-13].
This study observed the efficacy of acupuncture plus sitting-position knee-adjustment manipulations in treating PFOA. The report is summarized as follows.
1 Clinical Materials
1.1 Sample size estimate[12-14]
This trial was a test of superiority. We adopted this formula to estimate sample size:N= 2 × {(uα+uβ) ×σ/δ}2. Based on the previous research, we determinedα=0.05 andβ=0.10 took a one-tailedt-table withuα=1.645,uβ=1.282,δ=88.1,σ=186.0 (a comparatively larger standard deviation). When we applied these values to the formula, we obtainedN=76. The estimated sample size was 92 when the dropout rate was assumed to be 20%.
1.2 Diagnostic criteria
We made the diagnostic criteria of PFOA according to theGuidelines for the Diagnosis and Treatment of Osteoarthritis (2007)[15]. Anterior knee joint pain occurs while walking stairs or flexing-stretching the knee joint,or rub of the patellofemoral joint; X-ray examination reveals degenerative changes such as patellofemoral hyperostosis and subchondral osteosclerosis.
1.3 Inclusion criteria
Conformed to the diagnostic criteria for PFOA; aged 18-60 years; the joint disorders defined as mild-tomoderate, and the disease condition radiologically graded Ⅰ-Ⅱ (by Kellgren-Lawrence score)[16]; written informed consent and completed the trial as required.
1.4 Exclusion criteria
Coupled with conditions that cannot tolerate acupuncture or Tuina (Chinese therapeutic massage)manipulations, such as cardio-cerebrovascular diseases and diabetes; knee joint dysplasia, arthritis induced by immune disorders, knee fracture, severe meniscus injuries, or limited joint function; skin lesions, swelling pain, or inflammatory reactions around the knee joint;with bleeding tendency; with other contraindications for acupuncture or Tuina manipulations.
1.5 Dropout and elimination criteria
Those who withdrew from the trial due to personal reasons; those who showed poor compliance and failed to follow the treatment protocol or presented significant adverse reactions; those who took other treatments or drugs not permitted by the trial, which would interfere with efficacy evaluation; with the disease condition deteriorated through the course of the trial and had to be admitted to a hospital.
1.6 Statistical methods
We used the SPSS version 23.0 software for statistical analysis. The measurement data that satisfied normal distribution and homogeneity of variance were expressed as mean ± standard deviation (±s) and checked by thet-test. Those not distributed normally were described as median (interquartile range) [M (IQR)]and checked by the nonparametric test. The enumeration data were expressed as case numbers or percentages and analyzed by the Chi-square test.P<0.05 indicated statistical significance.
1.7 General data
This study recruited 92 patients between July 2019 and June 2020 from the outpatient of Shanghai General Hospital. The statistical staff adopted the SPSS version 23.0 software to run complete randomization to generate random numbers. In ascending order,numbers 1-46 were allocated to the observation group,and 47-92 were allocated to the control group. The subjects were assigned to the corresponding group according to their recruitment sequence. The two groups were statistically equal in comparing their general data, suggesting comparability (Table 1).
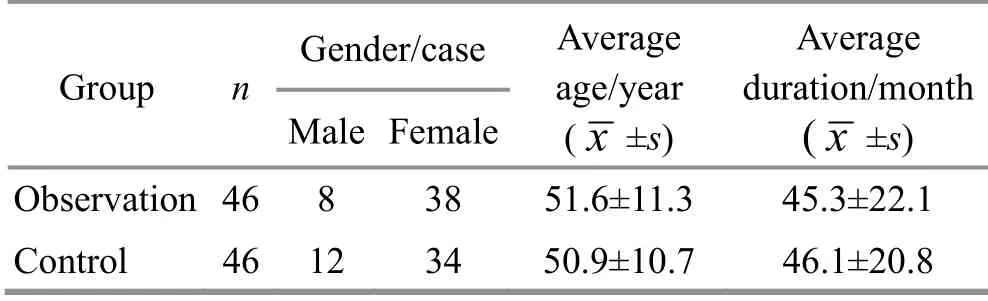
Table 1 Comparison of the general data
2 Treatment Methods
The two groups received the same exercise, daily life guidance, and joint-muscle training, including losing weight, necessary knee bracing, quadriceps training,and restricting knee joint weight-bearing.
2.1 Observation group
Patients in the observation group received acupuncture treatment and sitting-position kneeadjustment manipulations.
2.1.1 Acupuncture treatment
Points: Liangqiu (ST34), Yanglingquan (GB34), Xuehai(SP10), Neixiyan (EX-LE4), Dubi (ST35), and Yinlingquan(SP9) on the affected side[17].
Operation: The patient took a supine position with a cushion under the slightly bent knee (20-30°). After disinfecting the points with 75% alcohol cotton balls,the physician took sterile acupuncture needles of 0.25 mm in diameter and 40 mm in length to do the acupuncture treatment using the nail-pressing method.Liangqiu (ST34) and Xuehai (SP10) were perpendicularly punctured 15-20 mm in depth; Neixiyan (EX-LE4) and Dubi (ST35) were obliquely punctured to depths of 20-25 mm; Yinlingquan (SP9) and Yanglingquan (GB34)were also perpendicularly punctured, and the depth was 30-35 mm. After needle insertion, the physician evenly performed needling manipulations to obtain needling sensations (Deqi) and then retained the needles for 20 min.
2.1.2 Sitting-position knee-adjustment manipulations
The sitting-position knee-adjustment manipulations were performed following the acupuncture treatment.First, the patient was seated in a 45 cm high chair facing the doctor, who squatted or took a lower seat. Next, the doctor turned the patient’s foot on the affected side into the neutral position, ensuring a 90° angle between the calf and ground, pressed the lower patella edge upward with the thumbs, and encircled the popliteal fossa with the rest fingers. At the same time, the patient was asked to stand up and then sit down slowly.When standing up, the patient should keep the knee straight. The standing-up and sitting-down cycles were repeated three times, and the patient should try to complete them independently. This treatment was conducted every 2-3 d, 3 times a week for 8 weeks.
2.2 Control group
Patients in the control group took celecoxib capsules(State Food and Drug Administration Approval No.J20120063, Pfizer, USA) twice daily, 0.2 g per dose, for 8 consecutive weeks.
3 Efficacy Observation
3.1 Outcome measures
3.1.1 Symptoms score We developed the symptoms scoring standard based on theGuiding Principles for Clinical Study of New Chinese Medicines[18]. The severity of knee joint symptoms was scored and recorded before and after treatment: <10 points, mild; 10-18 points,moderate; >18 points, severe.
3.1.2 Pain score
We took the short-form McGill pain questionnaire(SF-MPQ) to describe pain intensity, including the pain rating index (PRI) score, visual analog scale (VAS) score,and present pain intensity (PPI) score. The PRI was scored in the range of 0-45 points, the VAS score ranged from 0 to 100 points, and the PPI was rated on a scale of 0-5 levels and scored 0-5 points accordingly. For the three measures, a higher score means more intensive pain.
3.1.3 Joint motor function score
The Lysholm knee scoring scale (LKSS)[19]was adopted to evaluate knee joint motor function. The LKSS score ranges from 0 to 100 points; the higher the score, the better the knee joint function.
3.2 Efficacy criteria
The efficacy criteria were made according to the
Guiding Principles for Clinical Study of New Chinese Medicines[18]and in consideration of the symptom score reduction rate. The symptom score reduction rate =(The symptom score before treatment - The symptom score after treatment) ÷ The symptom score before treatment × 100%.
Controlled: Knee joint function was normal, the pain was completely gone, and the symptom score reduction rate ≥85%.
Markedly effective: Knee joint motion was unlimited,the pain was gone, and the symptom score reduction rate ≥70% but <85%.
Effective: Knee joint function was slightly limited, the pain was substantially gone, and the symptom score reduction rate ≥30% but <70%.
Invalid: The improvements in knee joint function and pain were insignificant, and the symptom score reduction rate <30%.
3.3 Results
3.3.1 Comparison of the clinical efficacy
As Table 2 presents, the total effective rate was 87.0%in the observation group, higher than 63.0% in the control group, and the between-group difference was statistically significant (P<0.05).

Table 2 Comparison of the clinical efficacy Unit: case
3.3.2 Comparison of the pain score
We found no significant difference in the SF-MPQ scores between the two groups before treatment(P>0.05). After treatment, the PRI, VAS, and PPI scores dropped in both groups, all showing statistical significance (P<0.05). The three scores were lower in the observation group than in the control group,showing notable between-group differences (P<0.05).In addition, the post-treatment changes in the three scores were more significant in the observation group than in the control group, presenting statistical significance (P<0.05). The results suggest that both treatment protocols can reduce pain in the patients;however, acupuncture plus sitting-position knee adjustment manipulations can produce more significant efficacy than oral celecoxib capsules. The data are detailed in Tables 3-5.
3.3.3 Comparison of the LKSS score
There was no significant difference in the LKSS score between the two groups before treatment (P>0.05).After the intervention, the LKSS score rose markedly in both groups, showing statistical significance (P<0.05),and the score was higher in the observation group than in the control group, and the between-group difference was statistically significant (P<0.05). The post-treatment change in the LKSS score was also notably different between the two groups (P<0.05). The results indicate that the joint function shows more obvious improvements in the observation group than in the control group. The details are shown in Table 6.
Table 3 Comparison of the PRI score before and after treatment ( ±s) Unit: point

Table 3 Comparison of the PRI score before and after treatment ( ±s) Unit: point
Note: PRⅠ=Pain rating index; compared with the same group before treatment, 1) P<0.05.
Group n Pre-treatment score Post-treatment score Difference value Observation 46 24.76±8.30 12.13±5.961) 12.63±5.22 Control 46 24.69±7.24 15.74±6.881) 8.96±5.50 t-value 0.040 -2.690 3.288 P-value 0.968 0.009 0.010
Table 4 Comparison of the VAS score before and after treatment ( ±s) Unit: point

Table 4 Comparison of the VAS score before and after treatment ( ±s) Unit: point
Note: ⅤAS=Ⅴisual analog scale; compared with the same group before treatment, 1) P<0.05.
Group n Pre-treatment score Post-treatment score Difference value Observation 46 63.30±19.25 27.70±14.611) 35.61±10.04 Control 46 63.04±18.97 39.41±13.861) 23.63±10.57 t-value 0.065-3.946 5.573 P-value 0.948 <0.001 <0.001
Table 5 Comparison of the PPI score before and after treatment ( ±s) Unit: point

Table 5 Comparison of the PPI score before and after treatment ( ±s) Unit: point
Note: PPⅠ=Present pain intensity; compared with the same group before treatment, 1) P<0.05.
Group n Pre-treatment score Post-treatment score Difference value Observation 46 3.20±0.81 1.80±0.451) 1.39±0.68 Control 46 3.09±0.81 2.09±0.661) 1.00±0.60 t-value 0.644 -2.392 2.929 P-value 0.521 0.019 0.040
Table 6 Comparison of the LKSS score before and after treatment ( ±s) Unit: point

Table 6 Comparison of the LKSS score before and after treatment ( ±s) Unit: point
Note: LKSS=Lysholm knee scoring scale; compared with the same group before treatment, 1) P<0.05.
Group n Pre-treatment score Post-treatment score Difference value Observation 46 53.35±14.51 71.24±13.66 -17.91±8.18 Control 46 52.78±14.47 60.52±14.05 -7.74±6.47 t-value 0.180 3.709-6.614 P-value 0.858 <0.001 <0.001
4 Discussion
The chief target in treating PFOA is to ease pain,delay progression, improve and recover knee joint function, and enhance patients’ quality of life. The staged therapy for PFOA involves oral and external medications, rehabilitation, minimally invasive treatment, and surgery. Celecoxib is recommended by expert consensus to treat PFOA as its gastrointestinal adverse reactions are minor.
As we age, Qi-blood deficiency, liver-kidney insufficiency, and tendon and bone malnutrition will gradually arise, with subsequent loss of the tendon-bone balance, manifesting as knee pain and difficulty flexing and extending the joint. Hence,Qi-blood deficiency and imbalanced tendons and bones are the core pathophysiological feature in the development of PFOA.
It is the key to limbering tendons, activating collaterals, and supplementing Qi and blood in treating PFOA. Liangqiu (ST34) is the Xi-Cleft Point of the Stomach Meridian and is used to treat knee pain, low back pain, cold pain, numbness, difficulty bending the knee, etc. Xuehai (SP10) is an essential point for Qi-blood transportation and inpouring and can adjust and supplement Qi and blood. Yanglingquan (GB34) is one of the Eight Influential Points corresponding to tendons and is often used to treat tendon and bone diseases. Yinlingquan (SP9) can treat knee joint pain as the He-Sea Point of the Spleen Meridian. Also, Neixiyan(EX-LE4) and Dubi (ST35) are two points mainly used to treat knee pain. These points were used jointly to regulate and replenish Qi-blood, smooth and comfort tendons, and activate collaterals.
During the sitting-position knee-adjustment treatment, patients actively move the knee. During standing up, the quadriceps contract to effectively increase muscle force and strengthen joint stability,similar to the purpose of kinesiotherapy in physical therapy[20]. The sitting-position knee-adjustment manipulations are rooted in the tendon-bone theory of traditional Chinese medicine, biomechanics, and modern rehabilitation. It combines the patient’s active movements and the physician’s targeted adjustments to achieve a dynamic balance amongst the joint, muscles,and ligaments, help modulate knee muscle tone, and reduce the concentration of stress in the knee joint.During treatment, the patella moves between femoral condyles, facilitated and adjusted by the physician’s force, which can help the patellofemoral joint’s movements back to the normal track, lessen the potential wear and tear on the joint surface, and recover the joint’s dynamic and static functions[21].
The results here demonstrate that acupuncture combined with sitting-position knee-adjustment manipulations wins over oral celecoxib capsules in reducing pain and improving joint motor function and is a practical approach for PFOA. Furthermore, this integrated treatment is easy-to-operate and has no adverse reactions, thus worth applying and promoting.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by the Clinical Key Discipline Constructing Project of “Orthopedics of Chinese Medicine”in Shanghai Priority (上海市重中之重临床重点学科建设项目“中医骨伤科学”, No. 2017ZZ02024);New Cross Discipline of Traditional Chinese Medicine“Ergonomics of Tendons and Bones” in Shanghai (上海市中医药新兴交叉学科“工效筋骨学”); High-peak High-plateau Ⅰnnovative Orthopedics Chinese Medicine Team Project of Shanghai University of Traditional Chinese Medicine High-peak Creating-top Action Plan (上海中医药大学高峰造尖行动计划高峰高原创新中医骨伤团队项目); Three-year Development Project for Traditional Chinese Medicine of Shanghai (2018-2020 Year): Shanghai School of Traditional Chinese MedicineⅠnheritance Project [上海市进一步加快中医药事业发展三年行动计划 (2018 年-2020 年)海派中医流派传承工程, No. ZY(2018-2020)-CCCX-1009]; National Science and Technology Major Project for Major New DrugⅠnnovation of Ministry of Science and Technology of the State (国家科技部重大新药创制国家科技重大专项, No.2015ZX09101021); Projects of National Natural Science Foundation of China (国家自然科学基金项目, No.81704103, No. 81774340, No. 81973874, No. 81973875);2019 Scientific and Technological Project of Songjiang District of Shanghai (2019 年度上海市松江区科技攻关项目, No. 19SJKJGG29).
Statement of Informed Consent
Ⅰnformed consent was obtained from all individual participants.
Received: 23 February 2021/Accepted: 17 November 2021
猜你喜欢
现代中医药(2023年3期)2023-05-23 07:24:20
陕西中医药大学学报(2023年3期)2023-05-22 13:20:44
Chinese Physics B(2022年4期)2022-04-12 03:44:22
青年文学家(2022年32期)2022-02-13 10:55:10
——生态学
黄山学院学报(2021年5期)2021-11-06 02:10:56
佛山科学技术学院学报(自然科学版)(2021年4期)2021-08-31 02:32:16
佛山科学技术学院学报(自然科学版)(2021年3期)2021-06-15 02:42:52
水动力学研究与进展 B辑(2017年1期)2017-03-09 09:09:36
江西社会科学(2016年4期)2016-12-01 04:36:09
新高考·高一物理(2014年1期)2014-09-18 03:13:36
 Journal of Acupuncture and Tuina Science2022年6期
Journal of Acupuncture and Tuina Science2022年6期
- Journal of Acupuncture and Tuina Science的其它文章
- Efficacy of electroacupuncture for patients with dry eye syndromes: a randomized controlled trial
- Clinical observation of Tiao Shen Tong Du Tuina in promoting neuropsychological development of premature infants
- Clinical observation of acupuncture and moxibustion for functional dyspepsia due to Yang deficiency of the spleen and stomach
- Clinical study of acupuncture combined with medication for the elderly with Alzheimer disease
- Effects of herbal cake-partitioned moxibustion on the expression of thyroid autophagy-related factors LC3B and Beclin-1 in rats with autoimmune thyroiditis
- Effects of Tuina on serum creatine kinase and skeletal muscle mitochondria in delayed onset muscle soreness model rats