
Novel management indications for conservative treatment of chylous ascites after gastric cancer surgery
2022-11-21 09:10:16PengFeiKongYongHuXuZhiHuaLaiMingZheMaYanTaoDuanBoSunDaZhiXu
World Journal of Gastroenterology 2022年42期
Peng-Fei Kong, Yong-Hu Xu, Zhi-Hua Lai,Ming-Zhe Ma, Yan-Tao Duan, Bo Sun, Da-Zhi Xu
Abstract
Key Words: Gastric cancer; Chylous ascites; Conservative treatment; Drainage tube
INTRODUCTION
Chylous ascites (CA) was first reported by Morton in 1691 and is defined as the leakage of milk-like fluid that contains high level of triglyceride (TG)[1,2]. Gastric cancer (GC) is one of the most common malignant tumors worldwide, and a standardized protocol for radical surgical resection has been widely accepted as a safe and effective treatment[3,4]. CA generally occurs following abdominal surgery, the incidence of postoperative CA ranges from 2.06% to 11.80% in GC patients[5-7], as a result of disturbance of the cisterna chyli or its major tributaries[8,9]. The increased incidence of CA is considered to be likely due to the increased number of cancer patients undergoing more aggressive surgical interventions in addition to laparoscopic surgery[10]. CA presents a challenge as a relatively common postoperative complication and impacts subsequent adjuvant treatments in GC. In addition,massive and prolonged CA may lead to infection, malnutrition and immunodeficiency[11].
To date, treatment options for CA have included dietary measures, use of pharmacological agents and surgical or percutaneous interventions. A high-protein and low-fat diet with medium-chain triglycerides is often recommended for patients with CA[12]. Patients who do not respond to dietary restriction should receive total parenteral nutrition (TPN), which bypasses the bowel and may thus reduce lymph flow[13]. Continuous low-pressure drainage and somatostatin also represent effective conservative treatment for postoperative CA[6,14]. CA can be cured by lymphangiography and adjunctive embolization techniques that include direct percutaneous injection of glue into the leakage site or into the surrounding lymphoid tissue[15]. Furthermore, the use of surgical measures to successfully treat CA has been reported in patients with cirrhosis and CA that is resistant to conservative therapy[1].
In this study, we retrospectively analyzed 53 patients with CA after GC surgery, aiming to explore the vital factors that influence CA treatment and recommend novel conservative treatment strategies for postoperative CA in GC.
MATERIALS AND METHODS
Patients
We retrospectively reviewed all patients with CA who had undergone surgery for GC at our institution from 1 March 2006 to 31 May 2021. Three investigators performed a thorough review of all available data from the Fudan University Shanghai Cancer Center (FUSCC) medical record system, using RED Cap electronic data capture tools. In this cohort, 53 patients were admitted for gastric resection and lymphadenectomy: 2 underwent palliative resection and 51 underwent radical gastric resection with curative intent. This study was approved by the FUSCC review board in accordance with Chinese bioethical regulations, and all enrolled patients signed informed consent forms.
Definitions
CA was defined as the presence of milky or creamy peritoneal fluid in the drainage tubes, at a volume of ≥ 200 mL/d and a TG levels ≥ 110 mg/dL[1,11]. Additionally, the chyle test was routinely performed if the milky peritoneal fluid was suspected to be CA[16]. Clinical and pathological data, including the age, gender, AJCC (American Joint Committee on Cancer) stage, surgical procedure, lymph node dissection, drainage tube (DT) removal, time of oral feeding, time to CA onset, drainage duration, and hospitalization duration were collected and analyzed. All patients with CA were managed conservatively; the conservative treatments included TPN, continuous low-pressure drainage, somatostatin,DT clamping, and a low-fat diet. The time to CA onset was defined as the interval between the surgical procedure and the appearance of CA. Delay DT removal was defined as a DT removal time > 16 d after surgery for all patients or patients discharge with DT. Additionally, white blood cell counts, body temperature measurement, and germiculture were performed to diagnose CA combined with infection.DT clamping is defined as physical closing of the abdominal DT, with a daily open drainage time of about 2 h.
Statistical analysis
Categorical variable analysis was performed using theχ2test or Fisher’s exact test, and continuous variables were compared using Student’s t test. We used univariate logistic regression models to evaluate the risk factors of delayed DT removal in GC patients with postoperative CA, and a Cox regression model was used to perform multivariable analysis to calculate relative risk. All values were categorized into groups according to medians. All results were considered clinically significant at aPvalue < 0.05. Statistical analyses were performed using SPSS software version 19.0.
RESULTS
Clinical characteristics of gastric cancer patients with postoperative chylous ascites
Between 1 March 2006 and 31 May 2021, 16074 GC patients were hospitalized in our department and 7081 patients underwent gastrectomy and lymphadenectomy. Of these patients, 53 underwent surgical resection for GC and developed CA. The main characteristics and patient selection are shown in Table 1 and Figure 1. The patients had an average age of 61.0 ± 11.3 years, a high ratio of male and advanced stage of disease (Malevsfemale: 77.40%vs22.60%, early stagevsadvanced stage: 39.6%vs60.4%), 51 underwent radical surgery, 43 underwent D2 lymph node dissection, and 13 were discharged with DT.The average oral feeding and CA onset times after surgery were 3.8 and 7.5 d, respectively. The average durations of DT drainage and postoperative hospitalization were 14.3 and 21.9 d, respectively.
Delayed drainage tube removal has an important influence on gastric cancer patients with postoperative chylous ascites
In our data, 40 patients (75%) had their DTs removed during the hospitalization period, and 13 patients(25%) were discharged with DT (Figure 2A). As shown in Figure 2B and Supplementary Figure 1, both postoperative (R2= 0.979,P< 0.001) and total hospitalization time (R2= 0.791,P< 0.001) had a significant positive association with DT removal time. Moreover, the median postoperative DT removal time of the patients discharged with or without DT was 30 and 16 d, respectively (Figure 2C and Supplementary Figure 2). We defined the patients’ DT removal time > the median time (16 d) or the patients discharged with DT as delayed DT removal, and the patients were categorized into either the delayed DT removal or normal group (Figure 2D). Comparing the delayed and normal groups, delayed DT removal significantly extended the total and postoperative hospitalization times, duration of antibiotic usage, and hospitalization costs in the GC patients (postoperative hospitalization duration:25.8 dvs15.5 d,P< 0.001; total hospitalization duration: 33.2 dvs24.7 d,P< 0.01; antibiotic usage: 10.8 dvs6.2 d,P< 0.01; hospitalization cost: ¥9.2 × 104vs¥6.5 × 104,P< 0.01) (Figure 2E).
Characteristic differences between the normal and delayed drainage tube removal groups in gastric cancer patients with postoperative chylous ascites
We present the characteristic differences between the normal and delayed DT removal groups in Figure 3, Table 2 and Supplementary Table 1. First, we evaluated the clinical characteristics and detected that there were no differences between the two groups regarding gender, age, tumor size or location,lymphadenectomy, and AJCC stage. Second, the treatment-related features were further explored. Of note, the patients in the normal group were more likely to undergo DT clamping than the delayed DT removal group (35.0%vs0%,P< 0.001). In addition, compared with the patients in the delayed group, ashorter duration of low-fat diet were slightly shared in the normal group patients (40.0%vs63.6%,P=0.082). Third, we estimated the DT drainage variation between the two groups. Obviously, the delayed DT removal group generally had a longer duration of DT drainage than the normal group; however, the CA onset time and maximum drainage volumes were not significantly different between the two groups.

Table 1 Clinical characteristics of gastric cancer patients with postoperative chylous ascites
Infection and antibiotic usage were key independent factors influencing the delay of drainage tube removal
As shown in Table 3 and Figure 4, the univariate analysis revealed that early postoperative intake (RR:2.22, 1.10–4.48,P= 0.031), postoperative infection (RR: 2.20, 1.21-4.61,P= 0.003), and antibiotic usage(RR: 0.45, 0.22–0.91,P= 0.009) were significantly associated with delayed DT removal in GC patients with CA. However, the baseline characteristics (age, gender, and AJCC stage), lymph node dissection,CA onset time, maximum drainage volume, postoperative albumin, postoperative hemoglobin, and DT clamping were not significantly associated with delayed DT removal (allP> 0.05). Furthermore,multivariate analysis demonstrated that postoperative infection (HR: 2.40, 1.63-4.14,P= 0.007) and antibiotic usage (HR: 0.86, 0.76-0.96,P= 0.009) were independent factors that influenced delayed DT removal in GC patients with postoperative CA.
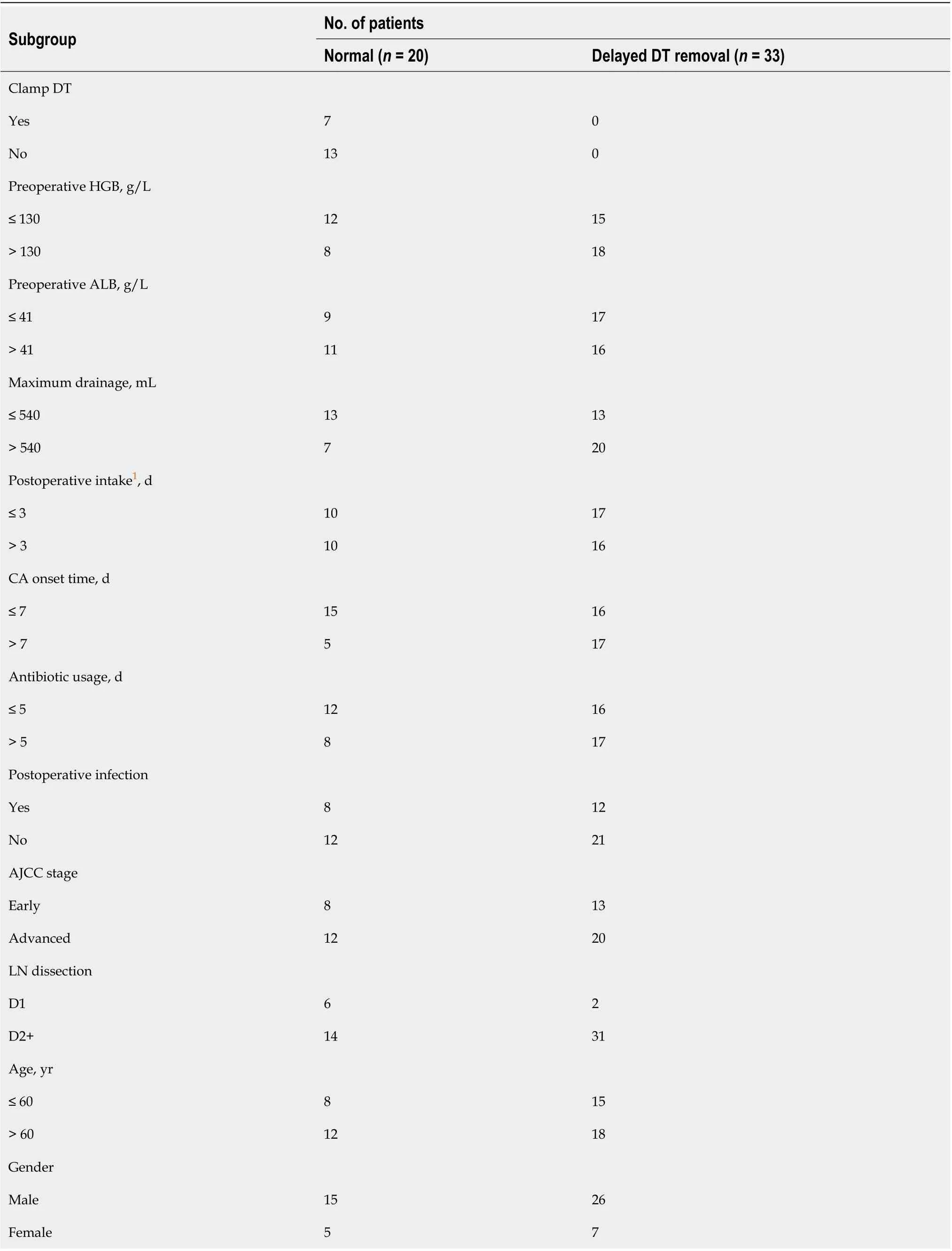
Table 2 Clinical characteristics differences between the normal and delayed drainage tube removal groups
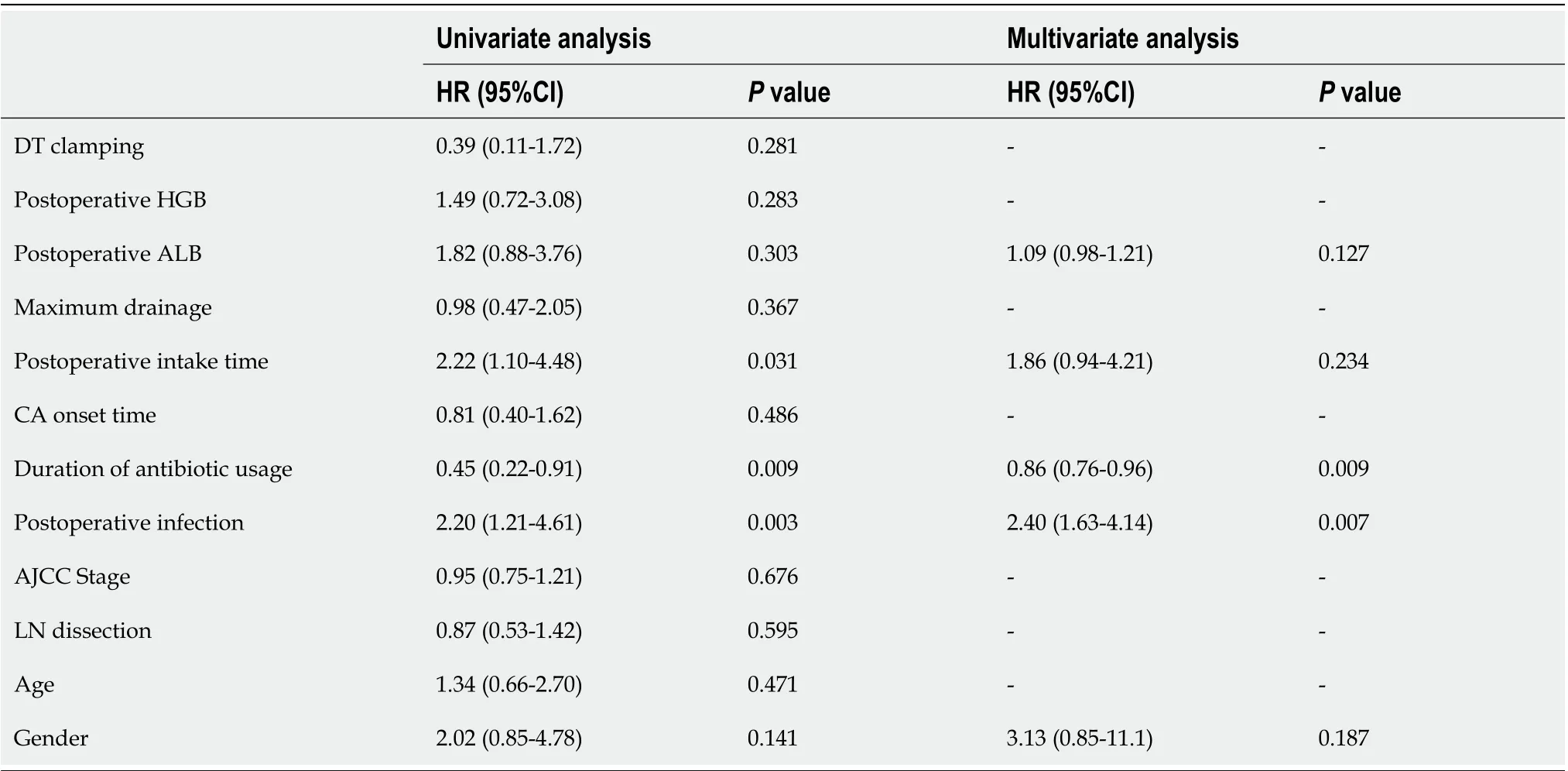
Table 3 Postoperative infection-related complications significantly affect gastric cancer patients with postoperative chylous ascites to remove abdominal drainage tubes in time
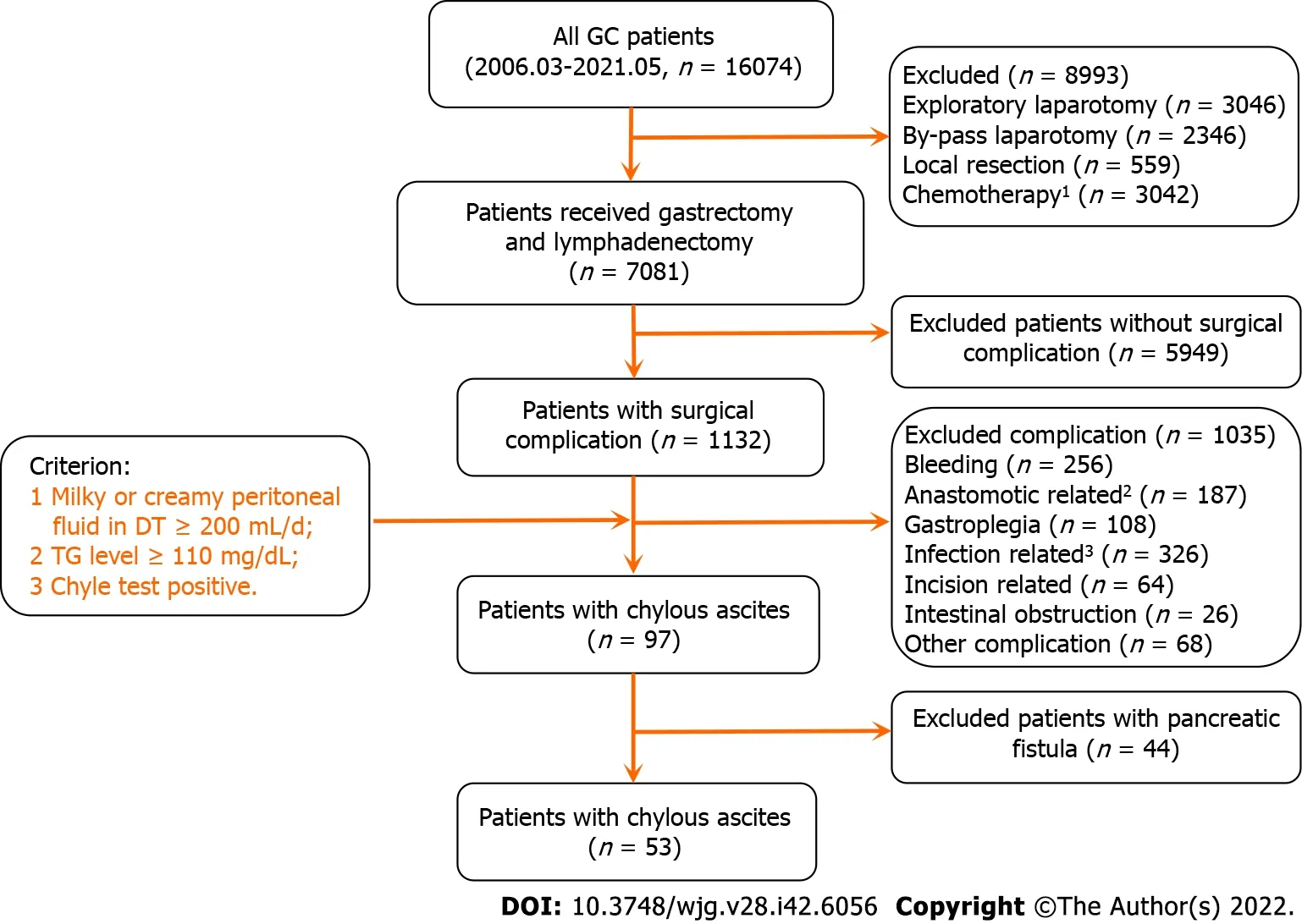
Figure 1 Flowchart of study included patients. 1Include the patients underwent neo-adjuvant, adjuvant, and palliative chemotherapy. 2Include the patients with anastomotic stenosis and fistula, except for the patients with anastomotic bleeding. 3The patients with all infection events except abdominal infection. GC: Gastric cancer; DT: Drainage tube; TG: Triglyceride.
Drainage tube clamping is a favorable method for the gastric cancer patients with postoperative chylous ascites
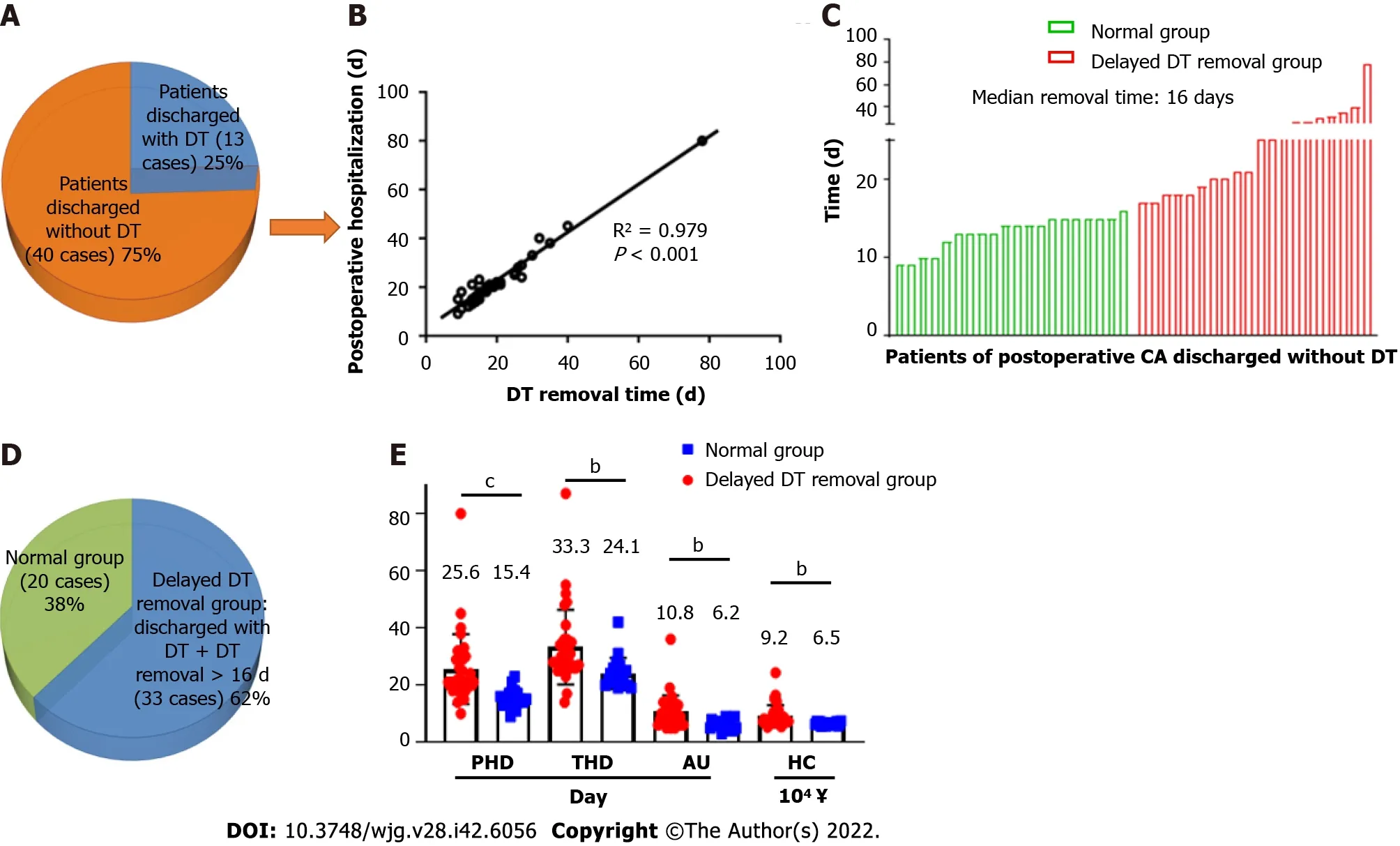
Figure 2 Delayed drainage tube removal has an important influence on gastric cancer patients with postoperative chylous ascites. bP <0.01. cP < 0.001. A: The status of drainage tube (DT) after discharged in gastric cancer (GC) patients with postoperative chylous ascites (CA); B: Postoperative hospitalization have a significantly positive correlation with the time of removal DT in GC patients discharged without DT; C: Time of removal DT in GC patients with postoperative CA who discharged without DT; D: The definition of delayed DT removal in GC patients with postoperative CA; E: Delayed DT removal obviously increase medical resources consumption and economic burden in GC patients with postoperative CA. GC: Gastric cancer; CA: Chylous ascites; DT: Drainage tube;PHD: Postoperative hospitalization duration; THD: Total hospitalization duration; AU: time of antibiotic usage; HC: Hospitalization cost.
In Figure 5A, we describe comprehensive treatment for GC patients with postoperative CA; the therapies included DT clamping, somatostatin, antibiotic, TPN, low-fat diet, and continuous low-pressure drainage. DT clamping was performed for seven patients during the hospitalization period when postoperative CA occurred, and the clamped DT patients had a shorter DT removal time than the normal and delayed removal groups (clamped DT groupvsnormal group, 11.8 dvs13.6 d,P= 0.047; clamped DT groupvsdelayed group, 13.6 dvs27.4 d,P< 0.001) (Figure 5B and Supplementary Figure 3).Moreover, similar clinical characteristics and treatment strategies were present in the three sub-groups(Supplementary Table 2). Our result further indicated that DT clamping significantly decreased total and postoperative hospitalization time, duration of antibiotic usage, and hospitalization costs in the GC patients with CA (Supplementary Figure 4). In Figure 5C, we dynamically observed the variation in daily drainage volume before DT removal (day 1 to day 7). Compared with the delayed removal group,start from day 3 before remove DT, the normal group and the clamped-DT group had relatively high drainage volumes. Additionally, the results of the drainage variation analysis indicated that 3 consecutive days of drainage volume less than 300 mL may be a suitable remove DT threshold in the GC patients with postoperative CA. Among two patients underwent DT clamping, computed tomography imaging of the abdomen showed that, after about 1 wk of DT clamping, the fluid in the abdominal cavity was reduced (Figure 5D).
Novel conservative therapeutic strategies for gastric cancer patients with postoperative chylous ascites
As the results mentioned above, we subsequently summarized the experiences of the GC patients with postoperative CA treatment in our department (Figure 6). First, the CA patients were divided into two sub-groups according to their postoperative infection status. Second, in the patients with infection,based on traditional treatments, antibiotic therapy was a vital supplement. Third, in the patients without infection, DT clamping was a viable option. Finally, for patients with 3 consecutive days of drainage less than 300 mL, DT removal might be the appropriate management.
DISCUSSION
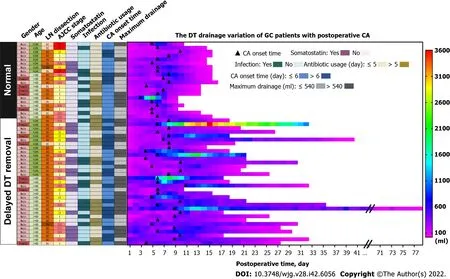
Figure 3 Overview of characteristic differences between the normal and delayed drainage tube removal groups in gastric cancer patients with postoperative chylous ascites. GC: Gastric cancer; DT: Drainage tube; LN: Lymph node; CA: Chylous ascites.

Figure 4 Exploration of multiple factors influence drainage tube removal in gastric cancer patients with postoperative chylous ascites.GC: Gastric cancer; DT: Drainage tube; LN: Lymph node; CA: Chylous ascites.
In this study, we retrospectively analyzed 53 cases of GC with postoperative CA at the FUSCC. Our results indicated that hospitalization duration was closely associated with DT removal time.Furthermore, postoperative infection and antibiotic usage were important independent factors that influenced delayed DT removal in GC patients with postoperative CA. Our study also implied that DT clamping was an appropriate method of postoperative CA treatment for patients without postoperative infection. More importantly, appropriate and lenient indications for DT removal can significantly reduce the duration of hospitalization.
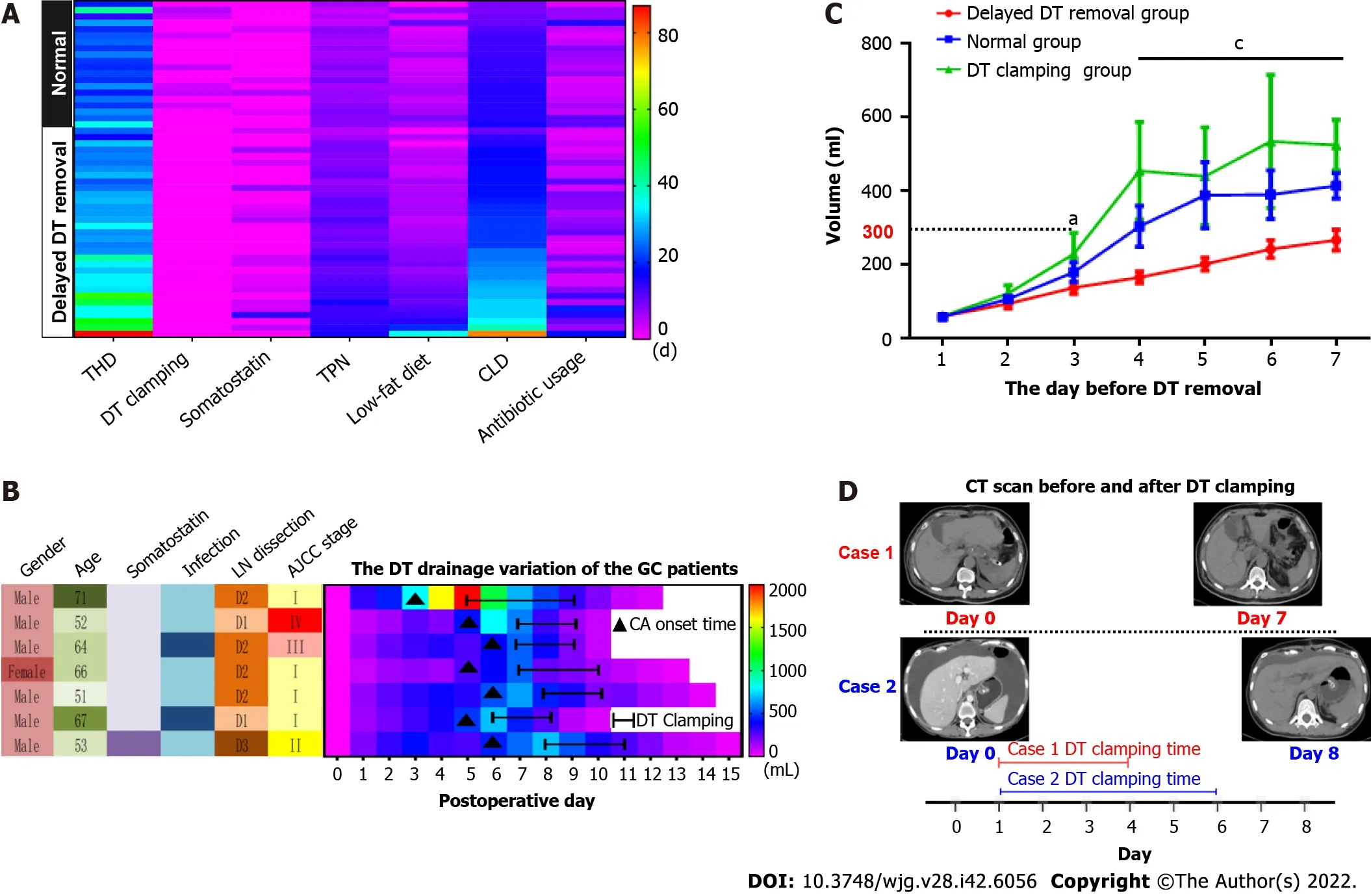
Figure 5 Drainage tube clamping is a favorable method for the gastric cancer patients with postoperative chylous ascites. A: Overview of overall treatment in the gastric cancer (GC) patients with postoperative chylous ascites; B: The drainage tube (DT) drainage variation of the GC patients underwent the treatment of DT clamping; C: The drainage of GC patients with postoperative chylous ascites in different groups before DT removal; D: Computed tomography scan indicate that the fluid in abdominal cavity was clearly reduced after the DT was clamped. THD: Total hospitalization duration; TPN: Total parenteral nutrition; CLD:Continuous low-pressure drainage; GC: Gastric cancer; DT: Drainage tube; CA: Chylous ascites; LN: Lymph node. aP < 0.05. cP < 0.001.
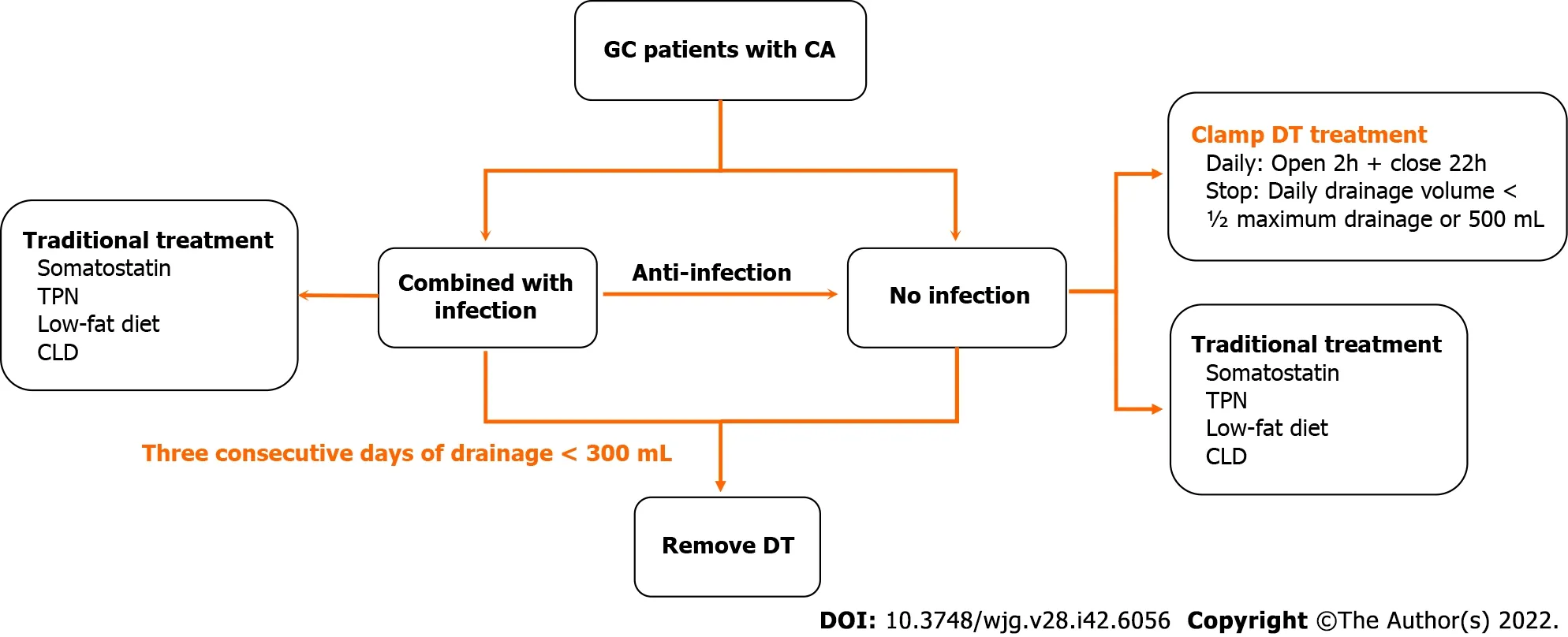
Figure 6 Novel conservative therapeutic strategies for gastric cancer patients with postoperative chylous ascites. TPN: Total parenteral nutrition; CLD: Continuous low-pressure drainage; GC: Gastric cancer; DT: Drainage tube; CA: Chylous ascites.
In most of the GC patients, postoperative CA cannot be discharged at a routine time and have a significant impact on subsequent adjuvant treatment[6,7]. Normally, patients are discharged within 7 d after undergoing GC surgery and most start adjuvant treatment within 30 d at our center. However, in the 53 patients with postoperative CA in our study, the average postoperative hospitalization duration was 21.9 d, and 8 patients’ postoperative hospital stays were longer than 30 d. As previously reported,lymphadenectomy was a key influencing factor in GC patients with postoperative CA[5,9]. As shown in Supplementary Table 3, the clinical characteristics of patients with CA tended to be consistent among those who underwent variety of lymphadenectomy, similar with previous studies that CA was found to be a rare complication even for gastric carcinoma patients undergoing D3 dissection[5,17].
Our results clearly indicated that hospitalization duration is mainly dependent on the time of DT removal in GC patients with CA. A multi-center prospective study recommended the criterion for DT removal be drainage flow between 500 and 1000 mL/d[6]. In fact, we previous performed relatively rigorous standards for DT removal in the patients with CA. Usually, while the volume of drainage less than 100 mL/d, the DT removal will be truly considered. Although all the patients’ DTs were removed until the flow volume less than 300 mL/d, and the delayed removal group preferred to perform a significantly high criterion. Therefore, we have a sufficient reason to conclude that, after excluding the influence of postoperative infection, early DT removal is a better choice in GC patients with CA.Moreover, our study found that postoperative infection and antibiotic usage were vital independent factors that influenced delayed DT removal in patients with CA, and clearly clarified anti-infection were an effective supplemental therapy for conservative treatment of postoperative CA. Similarly, Luet al[7]reported the patients with CA had a certain higher level of postoperative white blood cell counts than the other patients in GC.
Previously, the primary treatment for CA was conservative therapy, which mainly involved TPN,continuous low-pressure drainage, somatostatin, and a low-fat diet[18]. Recently, DT clamping has been presented as a potential alternative for patients with CA in other malignancies[19]. In this study, the DTs of 7 patients were clamped until the daily drainage was less than 500 mL/d (or ½ the maximum drainage). After DT clamping, the flow amount was significantly reduced, and the patients were successfully discharged without DT. For the reason of clamping DT facilitates DT removal, previous research has demonstrated absorption and lymphatic drainage increase along with the interstitial hydrostatic pressure[20]. Furthermore, DT clamping could help to evaluate the feasibility of DT removal by conveniently simulating the removal and conversion back to drainage[21]. Several studies have suggested DT clamping as an important alternative, and the detailed suggestion was daily drainage ranging from 1000 to 1500 mL[6,22]. However, a consensus on the threshold of drainage volume for DT clamping has not yet been reached. Therefore, determination of an appropriate criterion for DT removal and DT clamping is urgently needed for GC patients with postoperative CA.
There are certain limitations to our study. First, due to the retrospective study design, it was difficult to individually balance a variety of influencing factors; thus, various biases were unavoidable. Second,despite routine chyle test and TG were measured, the definition of CA is slightly less rigorous. In particular, CA with co-infection cannot fully rule-out the influence of pancreatic and anastomotic leakage, and other infection-related complications. In addition, small-volume CA (i.e., daily drainage volume ranging from 30 to 200 mL) was not considered in this study.
CONCLUSION
In conclusion, postoperative infection and antibiotic usage were vital independent factors that influenced delayed DT removal in GC patients with CA. Appropriate and lenient standards for DT removal can significantly reduce the duration of hospitalization. Furthermore, DT clamping might be a recommend alternative for conservative treatment of postoperative CA.
ARTICLE HIGHLIGHTS
Research results
Fifty-three patients underwent surgery for GC and experienced postoperative CA during the study period. Postoperative hospitalization and DT removal time showed a significant positive association (R2= 0.979,P< 0.001), while delayed DT removal significantly extended total and postoperative hospitalization times, antibiotic usage duration, and hospitalization cost. In addition, postoperative infection and antibiotic usage were independent factors for delayed DT removal.
Research conclusions
Postoperative infection and antibiotic usage were vital independent factors that influenced delayed DT removal in GC patients with CA. Appropriate and lenient standards for DT removal may significantly reduce the duration of hospitalization.
Research perspectives
DT clamping could be recommended as an alternative for conservative treatment of postoperative CA.
ACKNOWLEDGEMENTS
We thank Dr. Xuan Li for statistical advising and review of the manuscript.
FOOTNOTES
Author contributions:Kong PF and Xu YH contributed equally to this work; Xu DZ designed the research study;Kong PF, Xu YH, Lai ZH and Sun B performed the research; Kong PF, Xu YH, Ma MZ and Duan YT analyzed the data and wrote the manuscript; all authors have read and approve the final manuscript.
Institutional review board statement:The study was reviewed and approved by Ethics Committee of Fudan University Shanghai Cancer Center Review Board [Approval No. FUSCC-D-2021-164].
Informed consent statement:All study participants provided informed written consent prior to study enrollment.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:Dataset available from the corresponding author at xudzh@shca.org.cn. Participants gave informed consent for data sharing.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Ming-Zhe Ma 0000-0001-8858-0983; Da-Zhi Xu 0000-0002-2265-1272.
S-Editor:Gong ZM
L-Editor:A
P-Editor:Yuan YY
 World Journal of Gastroenterology2022年42期
World Journal of Gastroenterology2022年42期
- World Journal of Gastroenterology的其它文章
- COVID-19 associated liver injury: A general review with special consideration of pregnancy and obstetric outcomes
- Role of radiomics in the diagnosis and treatment of gastrointestinal cancer
- Computed tomography perfusion in liver and spleen for hepatitis B virus-related portal hypertension: A correlation study with hepatic venous pressure gradient
- Clinical value of predictive models based on liver stiffness measurement in predicting liver reserve function of compensated chronic liver disease
- Angiogenesis and immune checkpoint dual blockade: Opportunities and challenges for hepatocellular carcinoma therapy