
Factors influencing the optimal selection of central venous access devices: A qualitative study of health care team members’perspectives
2022-11-05 11:59YunShengTinglnWuChunmeiFnHixiHoWeiGo
Yun Sheng ,Tingln Wu ,Chunmei Fn ,Hixi Ho ,Wei Go ,*
a School of Nursing and Rehabilitation,Shandong University,Jinan,China
b Department of PICCs Clinic,Qilu Hospital,Shandong Univerisity,Jinan,China
Keywords:Central venous catheterization China Hospital medical staff Qualitative research
ABSTRACT Objective:This study aimed to explore health care team members’ understanding of the factors influencing the optimal selection of central venous access devices (CVADs).Methods:The data of the study was collected using semi-structured interviews.Twenty-six hospital medical staff (four hospital manager,15 head nurses,7 nurse) with experience in peripheral or central catheterization from four regions (Northern China,Southern China,Northwest China,and Qinghai-Tibet China)in China were interviewed between June and October 2021.Content analysis was used to analyze the data.Results:The results revealed five themes and 14 sub-themes.Patients: concerns,resources,requirements,and evaluation (security concerns,support resources,life requirements,evaluation among patients);nurses: awareness,knowledge,and popularizing methods (awareness of intravenous therapy,understanding of professional knowledge,forms of popularizing methods);doctors: support and involvement (support for decision-making,involvement in intravenous work);hospital managers: authority,quality control and continuing education (management of catheterization authority,quality control of intravenous infusion,investment in continuing education) and environment: differences and commonalities (differences in social support,and current commonalities).Conclusion:Nurses and other healthcare team members’ understanding,selection,use,and recommendation of CVADs have an indirect effect on patients’ decision-making.Therefore,hospital managers and government departments can indirectly strengthen medical team cooperation and improve learning education in order to improve the safety of patients receiving intravenous infusions.
What is known?
· The use of central venous access devices (CVADs) has become increasingly popular in recent years,and their advantages have been recognized,but sometimes they are not utilized to their full potential.
· Patients and health care team members would benefit from selecting the most appropriate CVADs at the earliest opportunity,according to the Infusion Therapy Standards (INS) of Practice 2021.
· The patient’s perspective has been explored in existing studies,but most factors are difficult to change,such as the patient’s financial resources,insurance coverage,educational attainment,age,health knowledge,mentality,transportation,family members’ support,and daily life habits.
What is new?
· This study explored health care team members’ understanding of the factors influencing the optimal selection of CVADs,which are significant,and neglected perspectives.
· Though the final decision is made by patients,health care teams also play an important role in their decision,which may provide another indirect way for optimizing CVADs selection.
· Measures should be adjusted according to the influencing factors in each region and hospital.
1.Introduction
Intravenous infusion is an essential part of clinical practice.According to statistics [1],more than 90% of hospitalized patients require intravenous infusion treatment.As a necessary tool for infusion,billions of venous access devices(VADs)are inserted into patients every year [2].With the increase in the prevalence of tumors and chronic diseases,central venous access devices (CVADs)have attracted more attention,such as their efficacy for infusion chemotherapy drugs and intravenous hypertrophic solutions [3].
Peripherally inserted central catheters (PICCs),centrally inserted central catheters(CICCs),and CICC or PICC ports(Ports)are the main CVADs in clinical use.Due to the differences in study populations,observation index,and puncture sites,the data from different studies on the three types of infusion tools are not comparable.This study reached the following conclusions by analyzing several systematic reviews and randomized controlled trials:ports placement time and costs are higher,but maintenance costs are lower than PICCs and CICCs [4,5].The mechanical and long-term complications rate of ports is lower than that of PICCs and CICCs,but it does not seem to be cost-effective when there are complications [3,6].The indwelling time of PICCs is better than that of CICCs but may increase the incidence of thrombosis due to the influence of the catheter-to-vein ratio (CVR) [7].
Each type of CVADs has its advantages and limitations.In addition to rates of complication and the economic costs,the selection of infusion tools should be based on the health care team’s initial diagnosis,a review of alternative therapeutic routes,and a risk assessment of the various treatment modalities[8].In the past,Milford et al.[9] introduced the challenges and options for longterm vascular access in different resource settings,and Clare [10]described the selection process.Still,the limited aspects were all introduced from a quantitative perspective.Besides,intravenous infusion is mainly the responsibility of nurses.Most studies have focused on patients but weakened the views and opinions of nurses[11,12].Therefore,this qualitative study aimed to understand factors that influence the optimal selection of CVADs,as understood by multi-level and multi-regional nurses and other health care team members.
2.Methods
2.1.Study design
Descriptive qualitative research based on the philosophical basis of naturalistic inquiry was conducted[13,14].This study performed semi-structured,face-to-face interviews to understand health care team members’ experiences of factors that influence the optimal selection of CVADs.The reporting of this research followed the Consolidated Criteria for Reporting Qualitative Research (COREQ)[15].
2.2.Setting and participants
Purposive sampling combined with the principle of maximizing differences was conducted between June and October 2021.When recruiting participants,age,gender,region,education,hospital level,department,and years of intravenous experience were considered.Regions in China are classified into four regions:Northern China,Southern China,Northwest China,and Qinghai-Tibet China.The sample size was based on data saturation,i.e.when no new topics appeared during the analysis.The inclusion criteria were as follows: 1) official employment in a hospital;2) a specialist certificate in intravenous therapy;3) voluntary participation in this study.The exclusion criteria were that they had no experience with peripheral or central catheterization after obtaining their certificates.Before the formal interview,the researchers provided the interviewees with a detailed explanation by email and informed them that a recording pen would be used to record the interview.A total of twenty-six individuals responded positively,and two were considered rejects for not responding within seven days.
2.3.Data collection
The interviews were conducted by a head nurse (W.Gao) in a 3,500-bed university-affiliated medical center in China.The researchers (W.Gao,H.Hao) are experienced in placing catheters in patients undergoing surgery,chemoradiotherapy,or palliative care owing to their long-term work.Most researchers(Y.Sheng,T.Wu,C.Fan,W.Gao) had undergone systematic training in qualitative research during their postgraduation.The backgrounds of all the researchers(Y.Sheng,T.Wu,C.Fan,H.Hao,W.Gao)were similar to the participants.Thus,a trusting relationship could be established between them before the interview.
Data were collected via semi-structured in-depth interviews supplemented by reflective diaries and observations.After obtaining informed consent,the authors’ scheduled interviews with the participants at a time convenient for them.Despite the limitations of distance and COVID-19,researchers took notes on the working environment and cultural atmosphere through direct observation or video recording.The interviews were conducted face-to-face(n=9) or via video conference (n=17) in hospital offices or meeting rooms in a relatively quiet environment.The main questions were as follows: 1) Can you tell us the current basis for selecting CVADs? 2) Do you think it is optimal in most situations?3)What factors do you think to influencing the optimal selection of CVADs?4)Based on this,do you have any useful suggestions?Two graduate students recorded the content of each interview and made field notes on their facial expressions,actions,and body language.Interviews were conducted within 30-50 min.Only the participants and researchers were present during the interviews.Within 24 h of conducting each interview,the researcher transcribed the audio and recorded the opinions,confusion,and deviations by writing memos and reflective diaries to ensure the completeness and accuracy of the interview content.Finally,the data included 26 transcripts,with an average of 43 min and 7,130 words per coding.
2.4.Data analysis
Considering the interview differences by geographical and role factors,the interview texts were sorted according to the participants’roles and initials(hospital managers 1-4,head nurses 1-15,or nurses 1-7),and the regional information was noted.The data were coded independently by two researchers under the guidance of a professor with qualitative research experience.In case of a disagreement between them,the professor was consulted to reach a consensus.Researchers used the conventional content analysis method to analyze transcribed data and field notes [16].The three steps include 1) the preparation stage: reading the material repeatedly and immersing in data to get a sense of wholeness;2)the organizing stage: adopting inductive content analysis,including open coding,categorization,and conceptualization;3)the reporting stage:reporting the data analysis process and results.
2.5.Ethical considerations
This study was approved by the Shandong University Research Ethics Committee (Approval no.2021-R-036).All data remain confidential and will not be disclosed to individuals or organizations outside the study,and subjects have the right to withdraw from this study at any stage.All participants signed a consent form before participating in the study.
2.6.Trustworthiness
Lincoln and Guba [17] suggest that the quality of qualitative research should be judged by the four criteria of credibility,transferability,dependability,and confirmability.Credibility is related to the actual value of research.At the research design stage,the interviewees’ opinions of the research issues,the recruitment methods,and interview forms were obtained before the interview.After analysis,this study used member checks to ensure the codes accurately reflected their views.Transferability refers to applying the research results to the population or environment outside the specific research samples.A purposive sampling combined with the principle of maximizing differences ensured transferability during the participants’ collaboration.Dependability is related to consistency and audibility in the research process,and voice recordings and written transcripts recorded all activities.Confirmability focuses on the neutral attitude of values.All the researchers in this study did their utmost to remain neutral and regularly recorded their opinions,any confusion or uncertainty,and breakthroughs during the introspective survey.
3.Result
3.1.Participant’s demographic information
Our study participants were 26 participant aged 29-59 years,who had worked as hospital managers (n=4),head nurses(n=15),and nurses (n=7).The geographical region,covers Northern China(n=10),Southern China(n=12),Northwest China(n=2),and Southwest China (n=2).Participants’ characteristics varied widely.The demographic data of the participants are presented in Table 1.
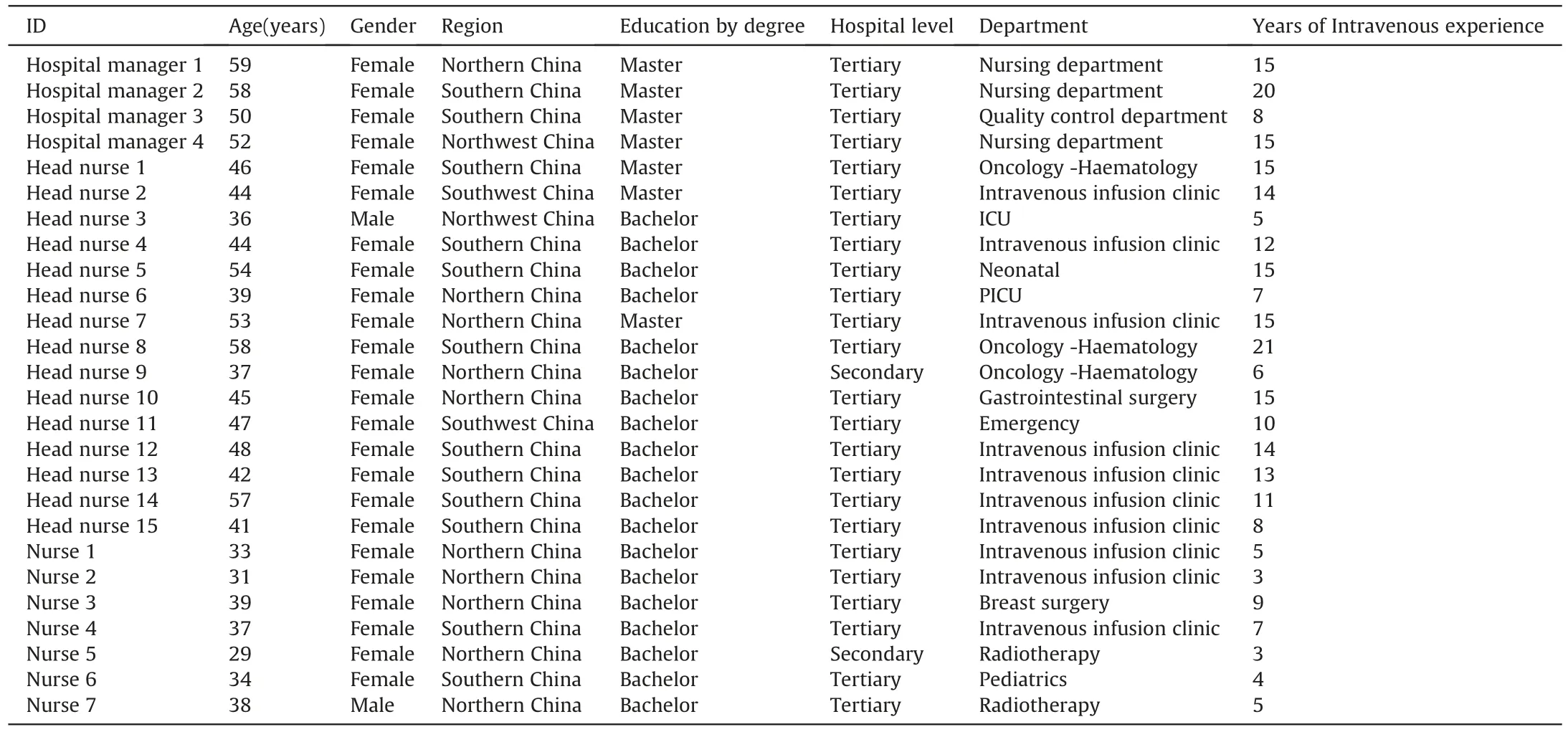
Table 1Demographic characteristics of the participants.
3.2.Themes and sub-themes
3.2.1.Patients: concerns,resources,requirements,and evaluation
Patients make the final decision for CVADs,and healthcare teams can only provide recommendations.There are many factors that patients need to consider before catheterization apart from the CVADs.Health care team members indirectly expressed patients’experiences in the following sub-themes:
3.2.1.1.Security concerns.CVADs are rarely known to patients until they are referred by a medical team.When faced with a large amount of medical information and extra expenses in a short time,doubts and concerns are authentic psychological reflections,especially for family members of children and the elderly with low educational levels.Several excerpts from the interviews are mentioned below.
“Compared with adults,catheter placement in children is more complex and dangerous.Parents,who are overprotective of their children,pose more questions about the safety of catheters and surgery.For example,‘Does anesthesia affect brain development?’‘A child’s heart is so small,will it puncture the heart?’”(Head nurse 6)
“CVADs,unlike drugs,do not have a noticeable effect on diseases.Many older adults with low educational levels hear about it for the first time before chemotherapy.Therefore,it is customary to doubt the function and safety of catheters.We want to explain it as clearly as possible,but not all patients can understand it.”(Head nurse 13)
3.2.1.2.Support resources.The protective effects of catheters on blood vessels are well-recognized.However,patients with poor economic conditions often delay or refuse catheterization when faced with additional medical expenses.Some participants mentioned the following:
“Most of our patients live in the surrounding rural areas.Although the advantages of CVADs are recognized,the cost of catheterization and maintenance cause tremendous financial pressure on the patients,and we have to respect their decision.”(Nurse 4)
“We usually introduce the PICC or CICC ports to patients with PICCs contraindications.However,it is very expensive and only affordable to some families.” (Nurse 1)
The examination and treatment of diseases can be a timeconsuming process takes for families.Some patients have to forsake catheters because regular maintenance is a big challenge.One participant mentioned the following:
“It is too cold in winter,and the roads are full of thick snow.Considering that family members need to take weekly leave from work,many patients give up CVADs.”(Head nurse 7)
3.2.1.3.Life requirements.Patients need to sustain a catheter for a long time,and its potential impact on their quality of life becomes a core concern before catheterization.An interesting phenomenon emerged in the interviews concerning the hot and humid weather.Participants from Southern China mentioned it more frequently.Some examples are as follows:
“After unilateral breast cancer surgery,patients experience difficulty with limited arm movement.It is more difficult for patients to receive PICCs when they hear that their bilateral arm movements will be limited (sigh).”(Nurse 3)
“Summer,like a stove (laugh),is stuffy and hot.Patients with excessive sweating have many concerns about postcatheterization,such as ‘does it affect bathing’ and ‘does it require increased maintenance.’” (Nurse 4)
“In summer,the weather is hot,which is difficult and tormenting for patients with PICCs.”(Nurse 12)
Some patients,such as role-stressed young adults,feel that carrying CVADs,especially exposed PICCs,will reveal their role of being a patient,leading to social distancing by colleagues and potential job loss.One participant mentioned the following:
“As the primary source of family income,many young adults need to work in treatment intermissions after remission.They often pay attention to the exposed part first because they may receive questionable glances from their colleagues.Their job may also be lost.”(Head nurse 1)
3.2.1.4.Evaluation among patients.‘Butterfly effect’states that even a small deviation in nursing care can cause a chain reaction across the nursing service.Positive evaluations of CVADs by patients can effectively improve their compliance,whereas negative evaluations can have the opposite effect.Some examples of relevant responses are as follows:
“Patients quietly evaluate everything.In cases complications occur repeatedly,patients slowly reduce catheterization,which is very difficult to reverse.” (Head nurse 12)
“On admission,a patient refused catheterization and said,‘Why didn’t I get a catheter when the other patients were getting one?’A nurse replied that it was too expensive.She said that if others could afford it,so could she and that money was not a problem.”(Head nurse 10)
3.2.2.Nurses: awareness,knowledge,and popularizing methods
Nurses are mainly responsible for popularizing knowledge about CVADs.Their concepts,expertise,and simplified explanations of intravenous therapy influence patients’decisions regarding CVADs.The following sub-themes exemplify nurses’ experiences.
3.2.2.1.Awareness of intravenous therapy.At present,there is high work pressure and a shortage of nurses [18].Nurses are more inclined to solve existing problems than assess potential risks when facing additional workloads.Some examples are as follows:
“Nurses have to complete many medical orders for different patients every day.If the skin around the puncture site is normal,then the VADs of the day before will be re-selected so that we can move to the next patient faster.”(Nurse 7)
“Many nurses regard CVADs as the last choice for intravenous therapy.In other words,CVADs are placed after a patient’s blood vessels have experienced multiple puncture failures.This poses a significant challenge to its service life.” (Head nurse 14)
Nurses,who are most familiar with patients’ vascular conditions,might leave the decisions to the doctors and passively complete their orders,ultimately missing the best time for catheterization.One participant mentioned the following:
“Nurses,who are most familiar with patients’ vascular conditions,should establish a sense of ownership and take the initiative to replace unreasonable VADs to protect the patient’s blood vessels in time.” (Hospital manager 3)
3.2.2.2.Understanding of professional knowledge.Due to the lack of professional expertise,nurses might make wrong judgments regarding patients’ diagnoses and various treatment modalities.Some participants mentioned the following:
“The knowledge in books can only provide a preliminary understanding of diseases.Nurses often encounter many stimulant drugs for the first time before treatment,and sometimes it is too late for temporary catheterization.”(Nurse 6)
“Not only specialized knowledge but also general knowledge.The intravenous teams spend a lot of time evaluating patients’ conditions.”(Nurse 4)
New technologies and methods for CVADs are continuously being developed.However,some nurses do not update their knowledge about technological developments and continue to work using their existing professional knowledge.One participant mentioned the following:
“In the past,PICCs needed to be repeatedly adjusted with the help of chest X-rays.The workload was so burdensome that we would give up before making a choice.During this advanced study,I have systematically studied the Intracardiac Electrocardiogram(IC-ECG)technology,hoping to provide patients with a more reasonable choice in the future.” (Nurse 5)
3.2.2.3.Forms of popularizing methods.Health education aims to guide patients in choosing the most appropriate VADs.Primarily,a combination of paper materials and oral communication is used to impart information in a simple but abstract manner.However,patients often cannot completely understand it and discontinue catheterization.They shared their experiences as follows:
“We usually have face-to-face communication with patients.Yunnan is the province with the most ethnic minorities in China.Many older patients can only speak dialects,which is indeed a challenge for us.”(Head nurse 15)
“We are making a vivid virtual simulation platform for CVADs.In the past,many patients had difficulty understanding our explanation and we could not achieve the purpose of health education.”(Head nurse 1)
3.2.3.Doctors: support and engagement
Patients’decisions are mainly influenced by doctors.Therefore,effective communication between them can increase the appropriateness of their choice.In addition,doctors are chiefly responsible for CICCs and Ports,and intravenous infusion work requires the involvement of doctors.The following sub-themes exemplify doctors’ values from nurses’ perspectives.
3.2.3.1.Support for decision-making.Intravenous infusion is not a familiar field for doctors and their knowledge of CVADs is not necessarily accurate.However,doctor-patient communication is still the most effective way to change patients’decisions;therefore,nurses need to seek the support of doctors.Some participants mentioned the following:
“Doctors’ professional knowledge and communication skills are better than ours,so patients have more trust in them.However,sometimes doctors are so busy that they do not have time to talk to patients about it (CVADs).” (Nurse 2)
“We have done intravenous therapy for 20 years,and half of that time was spent communicating with doctors.Patients trust CVADs more when doctors support us,and we can work more effectively.”(Head nurse 8)
3.2.3.2.Involvement in intravenous work.In addition to the widely used PICCs and CICCs,the emergence of ports provides a new option for patients receiving long-term intravenous therapy.However,some participants reported that catheterization qualifications affected the use of ports,which were unpopular in their hospitals.Some participants mentioned the following:
“Surgeons feel that ports surgery is not enough to bring novelty to their profession and provide satisfaction.…We have not come across one doctor who could do this work with us.”(Head nurse 14)“Catheters are inserted by interventional doctors,which has caused many unknown problems in our maintenance and use process.We hope that they can also be involved in continuous care.” (Head nurse 9)
3.2.4.Hospital managers:authority,quality control,and continuing education
The management of CVADs is a multidisciplinary and continuous observation work that requires hospital managers to develop unified definitions of catheterization authority and quality control indices and provide opportunities for continued education.The following sub-themes exemplify their experiences of managers.
3.2.4.1.Management of catheterization authority.The management of CVADs administration is not unified but mainly includes centralized catheterization in clinics and independent catheterization in departments.The former lacks a comprehensive understanding of patients’diseases and the latter often has fewer options,all of which affect the optimal selection of CVADs.The following excerpts support this statement.
“Our hospital adopts a centralized catheterization model,which makes it challenging to completely understand the needs of patients.This model is equivalent to handing over the selection decision to nurses in charge who are not familiar with CVADs.As a result,unreasonable selections have increased.” (Hospital manager 1)
“Our department only has PICCs,but sometimes patients may be more suitable for ports.If the collaboration between departments is poor,single CVADs will be used repeatedly.” (Head nurse 8)
3.2.4.2.Quality control of intravenous infusion.The reporting and handling of adverse events play a warning role in transforming the concept of intravenous therapy.At present,hospitals mostly use non-continuous quality follow-up indicators,which provide weak warnings about the idea of intravenous therapy.The following excerpts support this statement.
“We have a quality control team for intravenous infusion,but few people have experience with catheterization.Furthermore,the quality control indicators are discontinuous,mainly focus on complications reported,patient satisfaction survey.” (Hospital manager 4)
“Infusion risk management should be included in routine assessment work and given the same importance as falls and pressure injury to attract everyone’s attention and proactive assessment.This way can lead to the most appropriate selection of VADs.”(Hospital manager 3)
3.2.4.3.Investment in continuing education.The optimal selection of CVADs is based on a comprehensive understanding of new technologies and concepts.However,managers do not emphasize on continued education and provide few learning opportunities.Additionally,traditional learning methods are less effective.Some participants mentioned the following:
“Our most common method includes group observation of teachers during catheterization,which does not have a good learning effect.It is possible to cross the border with virtual simulation technology and establish a learning platform with excellent development prospects.” (Hospital manager 2)
“We hope to have some continuing education courses about intravenous therapy every year.This kind of opportunity is very less.” (Nurse 5)
3.2.5.Environment: differences and commonalities
The influence of environmental factors is unbalanced and uncontrolled,and mainly includes differences in social support and other irresistible common factors,such as COVID-19 and consumables prices.The environmental factors experienced by health care team members will be illustrated under each sub-theme in the form of quotations.
3.2.5.1.Differences in social support.The differences in social support are mainly reflected in the distribution density of maintenance sites and the introduction of medical items,which mostly occur in areas far from cities.The participants mentioned the following:
“During the interludes of chemotherapy when patients return to their homes,they do not know where to go for maintenance or are unable to maintain good quality.When they revisit the hospital,they are forced to extubate.In general,catheterization also fails.”(Head nurse 3)
“The price of CVADs has been more easily accepted by patients in recent years due in part to regional policies.However,the supply of catheters is insufficient due to the distance and inconvenient transportation.” (Head nurse 2)
3.2.5.2.Current commonalities.Patients’ decisions are closely related to the cost incurred by the catheters.Ports are more expensive and less reimbursed than other CVADs,leading to their limited popularity.
“The ports are self-paid.The butterfly needle used in the later period is also self-paid.Patients think that the chemotherapy only lasted 6-8 cycles,more than half a year is over,so the ports were abandoned.” (Head nurse 11)
In addition,medical treatment has become problematic in recent years,owing to the intermittent influence of COVID-19.The following excerpts support this statement.
“Due to the influence of COVID-19 in recent years,it has become difficult for patients to seek medical treatment.Patients are hesitant to carry CVADs because of maintenance frequency and treatment uncertainty.”(Head nurse 5)
4.Discussion
In 1998,Barton et al.[19] proposed at the World Congress on Vascular Access (WoCoVA) that the patients will have a vascular access plan that meets their needs upon admission.Subsequently,the European Society of Parenteral and Enteral Nutrition (ESPEN)[20] and Infusion Nurses Society (INS) [8] also mentioned that selection of the most appropriate VADs is necessary to avoid potential risks to patients,medical staff,and medical institutions.As early as 1998,Freytes et al.[21]focused on the selection of VADs and found that 45%of respondents decide to use VADs depending on the drugs used instead of the status of patients’ veins at the beginning of therapy.Previous studies [22,23] have shown that CVADs have superior advantages over peripheral intravenous catheters(PIVCs),but they are less commonly used,so this study focused on CVADs rather than all catheters.The initial hypothesis of this study was based on these studies.That is,the advantages of CVADs are gradually recognized,but sometimes they are not adopted.Therefore,this study further explored the factors that influence the optimal selection of CVADs.Through interviews with 26 hospital medical staff,it was found that the healthcare team,particularly nurses,also plays an important role in patients’ decision-making,although there were slight differences across regions and hospitals,which may provide an additional means to improve CVADs selection.
Doubts and concerns about the safety of CVADs affect patients’decision-making,which is mainly influenced by a lack of awareness and knowledge.Berger et al.[24] showed that only 52.7% of patients knew about their PIVCs,and CVADs were worse.Ai et al.[11]adopted a qualitative study to understand the hindrances of regular care in leukemia patients,similar to this study’s results from the health care team members’ perspective.First of all,CVADs’ placement and maintenance costs range from several hundred to several thousand dollars [4].As a result of enormous medical and transportation costs,patients delay or refuse CVADs,especially in less developed areas of Qinghai-Tibet China,and Northwest China.It is recommended that relevant departments increase the reimbursement ratio,especially for remote areas and low-income families,to reduce the economic burden on patients.Secondly,CVADs bring inconvenience to daily life,but it seems that the strange eyes of others are more worrying for patients[25].Shim et al.[26]showed that patients with stigma were three times more likely to lose a job than others,and exposed PICCs further aggravate this risk.The above suggests that healthcare teams should consider both therapeutic and psychological needs,and ports can be recommended when necessary because they offer unique psychological benefits[27].
Several VADs options are available in clinical practice,and nurses need to act as patient advocates to ensure proper catheter selection is made.To provide the most appropriate recommendations,nurses should spend more time on continuous education,including drug characteristics,disease characteristics,and intravenous infusion tools,which have been mentioned in previous studies [28,29].Furthermore,our study participants,especially those from large medical centers,suggested nurses should improve their catheterization authority by using the puncture advantage.A study by Davis et al.[30] also showed that the effect of nurse-led PICCs was better than that of doctors.Thus,it may be feasible for nurses to broaden the scope of catheterization.
Expanding catheterization authority puts more pressure on nurses,and obtaining doctors’ support and engagement is always the preferred way.Cao et al.[31] further showed that a judicious application of a multi-disciplinary team (MDT) can effectively improve the quality of nursing.In addition to intravenous therapy specialist nurses,the MDT includes personnel in the ultrasound,imaging,interventional,infection,vascular surgery,pharmacy,and equipment departments.Hospital managers should ensure that health care teams work together and look for a leader who is not limited to nurses,which will benefit the establishment of MDT.
Traditional training methods use simulated humans,which lack clinical validity.According to a study by Saks et al.[32],62%of the training content will be applied to clinical work quickly after professional training,but only 34%of the core content will be left after one year.In this study,many participants also reported a problem with knowledge confusion.Virtual simulation technology has the characteristics of visualization,interaction,and authenticity [33].Combining this technology to create a virtual reality(VR)platform will perfectly meet the needs of intravenous therapy training.Additionally,CVADs popularity is affected by transportation,maintenance sites,and other environmental factors.Through a combination of network services and door-to-door services,it will become feasible for nurses to provide home maintenance services to these discharged patients.
5.Limitations
There are some study limitations.Firstly,the purposive sampling method was used to select hospital medical staff from different regions in China.The findings should be cautioned because healthcare systems are different in other countries.Secondly,intravenous therapy involves many disciplines,and this study cannot explain the views and suggestions of personnel in other fields.Nevertheless,nurses are the primary users and beneficiaries of CVADs,which makes this study very valuable in clinical settings.
6.Conclusions
Several catheters are available in clinical practice.Establishing optimal CVADs before treatment is beneficial for both patients and health care teams.The findings indicate that optimal CVADs selection is not limited to the factors related to patients alone and that healthcare teams also play a significant role in their decisionmaking.Nurses should be recognized by doctors and hospital managers while strengthening their learning,which would further optimize the selection of CVADs.
Funding
This work was supported by Practice Teaching research project of Shandong University (No.2021Y240).
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
CRediT authorship contribution statement
Yuan Sheng:Conceptualization,Methodology,Investigation,Data curation,Writing-original draft.Tinglan Wu:Data curation,Methodology,Writing -review &editing.Chunmei Fan:Data curation,Methodology,Writing -review &editing.Haixia Hao:Data curation,Supervision,Visualization.Wei Gao:Conceptualization,Methodology,Investigation,Supervision,Writing-review&editing.
Declaration of competing interest
The Authors declare that there is no conflict of interest.
Acknowledgements
The authors would like to acknowledge all participants for their understanding and support of this study.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.09.006.
 International Journal of Nursing Sciences2022年4期
International Journal of Nursing Sciences2022年4期
- International Journal of Nursing Sciences的其它文章
- Effects of equine-assisted interventions on older adults’ health: A systematic review
- Multicenter application of a nursing workload measurement scale in adult hospitalization units
- Exploring social movement concepts and actions in a knowledge uptake and sustainability context: A concept analysis
- Palliative care needs and symptom burden in younger and older patients with end-stage renal disease undergoing maintenance hemodialysis: A cross-sectional study
- Lived experiences with unmet supportive care needs in pediatric cancer: Perspective of Chinese children and their parents
- Development and validation of a nomogram for predicting the risk of pressure injury in adult patients undergoing abdominal surgery