
Lived experiences with unmet supportive care needs in pediatric cancer: Perspective of Chinese children and their parents
2022-11-05 11:59LeiChengLingYuHaiyingHuangMingxiaDuan
Lei Cheng ,Ling Yu ,Haiying Huang ,Mingxia Duan
a School of Nursing,Fudan University,Shanghai,China
b Hemotology & Oncology Unit,Children’s Hospital of Fudan University,Shanghai,China
c Hemotology & Oncology Unit,Guangzhou Women And Children’s Medical Center,Guangdong,China
d Hemotology & Oncology Unit,Anhui Provincial Children’s Hospital,Anhui,China
Keywords:Children China Health services needs and demand Neoplasms Parents Qualitative research
ABSTRACT Objective:Unmet supportive care needs(SCNs) impact pediatric cancer patients and their parents.This study aimed to explore the unmet SCNs from the perspective of Chinese children with cancer and their parents through lived experiences.Methods:The data of this study was collected using face-to-face semi-structured interviews.The participants were recruited from the oncology units of three children’s hospitals in China’s cities(Shanghai,Guangzhou,and Hefei)from October 2020 to December 2021.Data were analyzed using Colaizzi’s sevenstep phenomenological analysis method.Results:Eight pediatric cancer patients and twenty-four parents were enrolled in the study.Four main themes and eight subthemes(both children’s and parent’s perspectives)were generated:1)meeting the ongoing needs along the cancer trajectory(can you tell me what comes next;our needs are growing);2)communicating with a family focus(they only talk to my parents;let each family member have a voice);3) providing care beyond the treatment (I am bigger than my body [the children’s needs for emotional consolidation and information about their prognosis];there are things beyond treatment);4) getting support from the community (I am not a monster [the children were unhappy about being treated differently];we want to connect with the resources near us).Conclusion:This study revealed multiple unmet SCNs from the perspective of Chinese children with cancer and their parents.The findings call for comprehensive and in-depth supportive care beyond treatment,integration of the family member voice in pediatric cancer care,and a coordinated pediatric cancer support mechanism in the Chinese healthcare system.
What is known?
· Pediatric cancer patients and their families experience unmet supportive care needs (SCNs) that may impact their physicalpsychosocial well-being.
What is new?
· This study revealed the multiple unmet SCNs from the perspective of Chinese children with cancer and their parents.
· There is a need for supportive care beyond treatment,integration of the family member voice,and a coordinated pediatric cancer support mechanism in the Chinese healthcare system.
1.Introduction
There are about 400,000 children and adolescents diagnosed annually with cancer all over the world [1].The estimated agestandardized incidence rate for pediatric cancer in China is 87.1 per million [2].Though mortality in pediatric oncology has significantly declined,the profound impact of cancer diagnosis and subsequent treatment cannot be overlooked.Reported challenges across the pediatric cancer continuum include but are not limited to treatment-related symptoms and side effects [3],psychological morbidity [4],challenged transition to adult medical care [5],impaired family function [6],social isolation [7],etc.However,these children’s and their families’varied needs are not always fully recognized and addressed in clinical practice throughout their cancer journey.
Supportive Care Framework for Cancer Care is a widely recognized theory used to examine patients’ unmet supportive care needs (SCNs),which is conceptualized to comprise physical,psychological,emotional,practical,informational,spiritual,and social elements[8].Identifying unmet SCNs,i.e.,the discrepancy between patients’ concerns and their care,facilitates the development of targeted patient-centered care interventions [9].Cancer patients are recognized as those with high levels of unmet needs [8].Systematic reviews (mostly on the adult population) have suggested high levels of concurrent unmet SCNs across different cancer types and stages on the cancer care continuum[9-11].However,there is limited research reporting evidence regarding the patients’ and families’ understanding and lived experiences related to unmet needs.
In pediatric oncology,providing adequate supportive care is important to improve the quality of life in children with cancer[12].The perspective of children and their parents is most valued to assess unmet SCNs.Unlike clinicians who tend to solve somatic issues,children’s and parents’ unmet needs are closely linked to their daily experiences [13].Existing literature has highlighted high-level unmet needs in emotional support,communication,information supply,and psychological care reported by pediatric cancer survivors,family caregivers,and bereaved parents [14-16].A cross-sectional study investigated Indonesian parents of hospitalized children with cancer using the Supportive Care Needs Survey.This study found that the unmet needs of the parents were complicated,with needs in terms of information support being the highest [14].Likewise,a study conducted on a similar scale reported information needs as the highest unmet need for caregivers of childhood brain tumor patients in England.However,the cancer survivors reported that most unmet needs were mainly in the psychological domain (e.g.,anxiety,uncertainty,and depression)[15].Meanwhile,a qualitative study explored Australian bereaved parents’experiences and unmet needs for palliative and supportive care throughout their child’s illness.The findings highlighted the need to keep children engaged in the decision-making process and the delivery of sensitive developmental care [16].Nevertheless,there is still a lack of adequate evidence regarding the true understanding that this particular population has unmet SCNs through the lens of their own experiences.More qualitative data may facilitate a more in-depth understanding of this topic,which may urge the development of early intervention and service delivery in pediatric oncology.
Regarding the Chinese population,a recently published systematic review,guided by the Supportive Care Framework for Cancer Care,identified health systems and information as the most prevalent area of unmet SCNs reported by migrant and native Chinese adult cancer patients and caregivers [17].The authors suggest a lack of data from the patients’ and caregivers’ perspectives.Another study examined parents’perspectives on healthcare services during their children’s hospitalization.This study identified various unmet Chinese family needs,e.g.,warm and supportive attitudes,competent care,adequate information,a comfortable environment,and catering support[18].More evidence needs to be made available about the SCNs of Chinese children with cancer.Limited understanding of the views of patients and those close to them may hinder the provision of more responsive and adaptive care.Thus,this study aimed to capture the lived experiences of Chinese children with cancer and their parents relating to their unmet SCNs.
2.Methods
2.1.Study design
A descriptive qualitative study was conducted.A qualitative description assists a naturalistic perspective of the participants with insightful analyses of phenomena or experiences [19].This study follows the Consolidated Criteria for Reporting Qualitative Studies (COREQ).
2.2.Setting and participants
The participants were recruited from the hematology/oncology and surgical oncology units from three children’s hospitals in China’s cities(Shanghai,Guangzhou,and Hefei)from October 2020 to December 2021.The inclusion criteria for this study include children with a diagnosis of all types of pediatric cancer,active treatment,and the ability to speak Chinese.The participating hospitals admitted children aged between 0 and 14 years old.Thus for this study,the age requirement of child participants was between 8 and 14 years old.Pediatric participants who,in the opinion of their physician,were not mentally or verbally capable of participating in the interview were excluded.Parents were identified as the children’s main caregivers while accompanying the child in the hospital.Only one parent was allowed to be in the caregiver role under the hospital policy during the research period.In this study,children and parents were not recruited as dyads.Parents were still eligible to participate if the child did not meet the inclusion criteria.
2.3.Recruitment and enrollment
A trained senior nurse at each site served as the onsite focal person.The nurse initially approached the parents/guardians to determine whether they were interested in the study.The Principal Investigator then contacted the interested participants (parents and/or child) and verbally explained the purpose and protocol of the study.
2.4.Ethical considerations
Ethics approval was obtained from the Institutional Review Board of the Fudan University,School of Nursing(IRB#2019-02-06).The participants were assured that the interview would be voluntary and confidential and that they had the right to withdraw at any time.The child’s assent and the parent’s written informed consent were obtained before the interviews started.
2.5.Data collection
The semi-structured interviews were conducted by the first author,a doctoral degree-prepared nursing faculty member who was previously trained in interviewing children and adults.All the data collection procedures were completed in the hospital setting when the child came for treatment.The parent was allowed to stay with the child but not encouraged to interrupt or provide any explanation to their child during the interview session.The child’s interview would be carried out first if both the child and parents agreed to participate.
The interview guide was developed and guided by the Supportive Care Framework for Cancer Care.Participants were first asked an open-ended question about their general perception and experience since the cancer diagnosis.The interviewer then proceeded to cover each domain of the unmet SCNs with two questions:1)“During this process,were there any needs that you think were unmet in … (physical,psychological,emotional,practical,informational,spiritual,social care)?” followed by 2) “Could you further describe your experiences with these unmet needs?.” For child participants who might not fully understand the meaning or terms of the domains,there would be a layman’s explanation previously set by the research team (e.g.,physical care is the care performed on your body).This interview guide was piloted in the first two interviews to test the child participants’understanding of the topic and specific questions.
All interviews were audio-recorded.Field notes were taken during and after the interviews.Data collection and analysis were performed concurrently.The recruitment of participants continued until no additional data led to the generation of additional perspectives.
2.6.Data analysis
Data were analyzed using Colaizzi's seven-step phenomenological analysis[20].The process included familiarizing the data by reading through the transcripts,identifying significant statements relevant to the phenomenon,formulating meanings,clustering themes,describing the themes,condensing the described themes down to short statements that capture the essence of the phenomenon,and finally seeking verification of the themes through another review of the transcripts.Each transcript was analyzed by at least two researchers of the team (all females,three bachelor of science in nursing,and one doctoral degree prepared registered nurse,previously received training in qualitative data analysis method).The identified themes were shared and discussed across the team until a consensus was reached.Significant statements were extracted to develop emerging themes.
2.7.Trustworthiness
Throughout the analysis,the team members met regularly and tried to bracket their suppositions by reflexively discussing the potential data influencers from their perceptions and past clinical experiences.They used an audit trail to record the analysis process when data were compared across interviews with the reflective field notes.Meanwhile,detailed descriptions of the data were used to achieve transformability.
3.Results
3.1.Participants’ characteristics
Only two potential pediatric participants refused to participate for the reason of being “too tired”.Eight pediatric cancer participants (9-14 years old;5 males and 3 females) and twenty-four parent participants (30-54 years old;6 fathers and 18 mothers)were enrolled.Most patients were diagnosed with leukemia or brain tumors (Tables 1 and 2).The interviews took an average of 15-25 min for the children and 20-40 min for the parents.
3.2.Qualitative results
Four themes and eight subthemes(both children’s and parents’perspectives) were generated from the data.Table 3 shows how these themes correspond to the domains of the Supportive Care Framework for Cancer Care.

Table 1Demographic data of children.
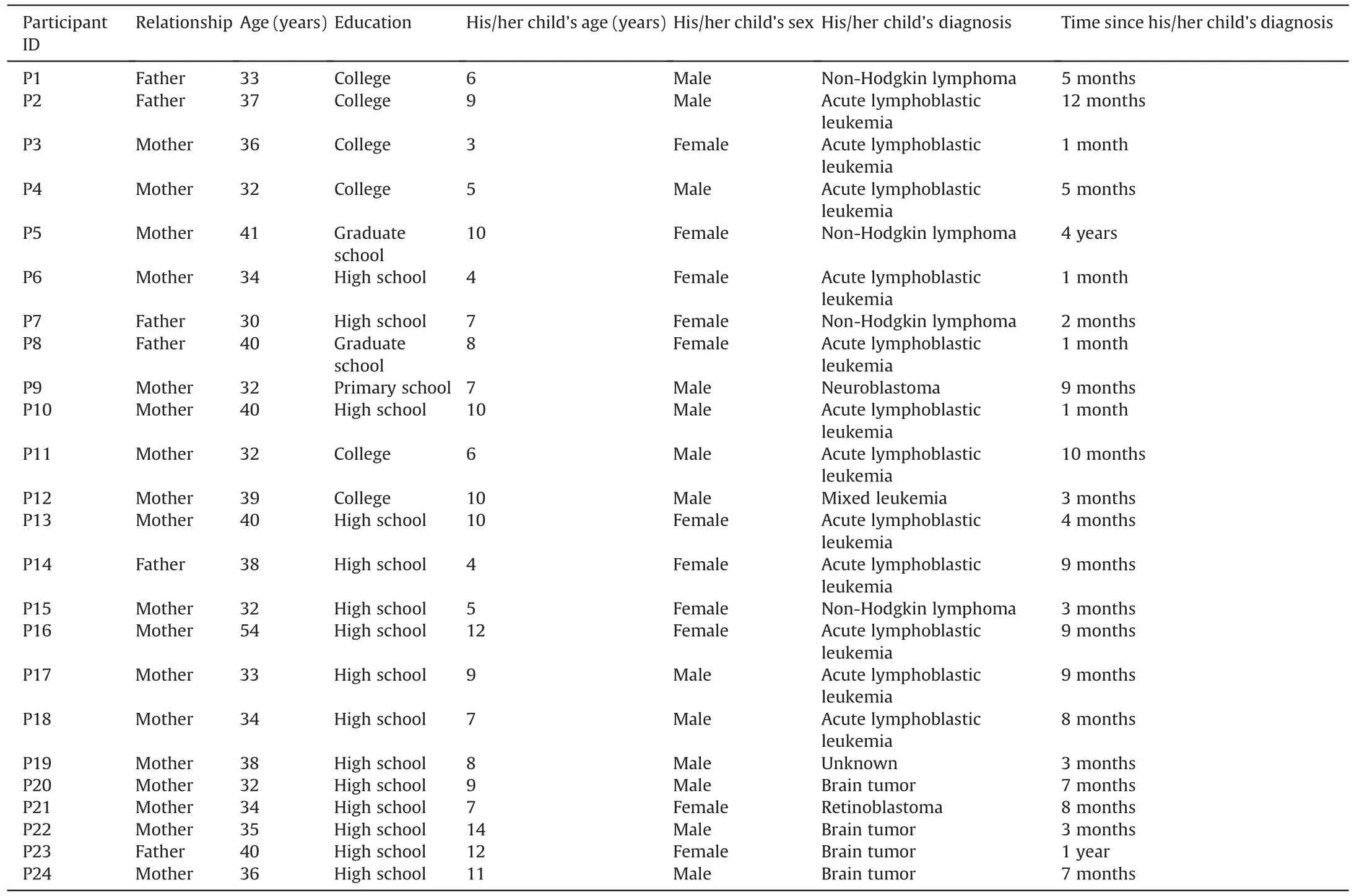
Table 2Demographic information of parents.
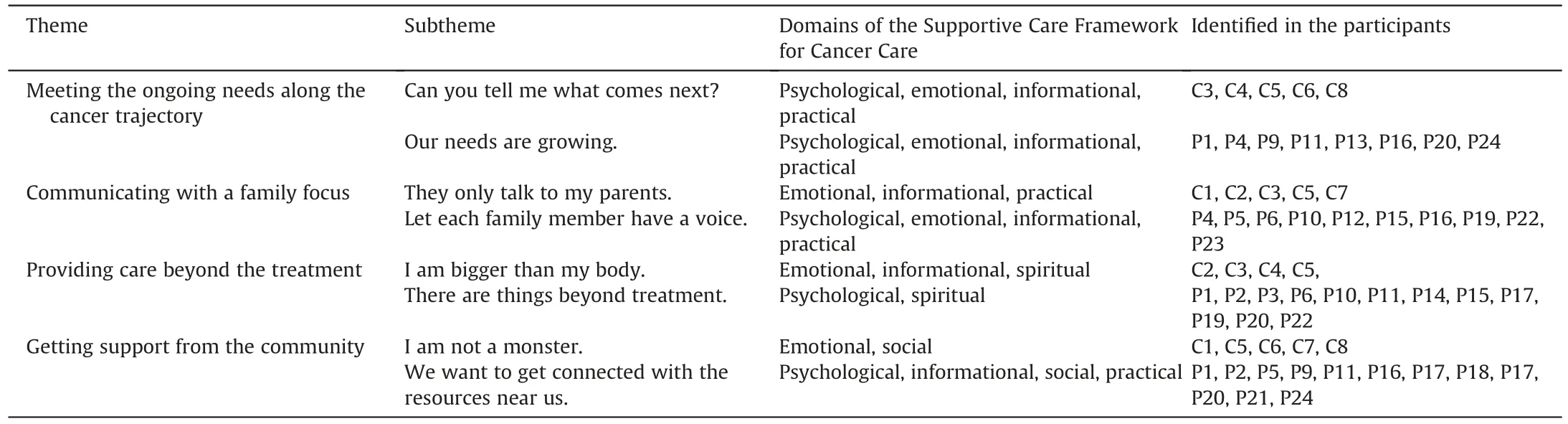
Table 3Themes and subthemes that emerged from interviews and domains of the Supportive Care Framework for Cancer Care.
3.2.1.Theme 1: Meeting the ongoing needs along the cancer trajectory
The participants perceived the changing nature of various needs along their respective cancer trajectories.Their unmet needs were related to their experiences at each stage,from diagnosis to intense treatment,maintenance therapy,and survivorship.Their needs were“ongoing”as they proceeded with treatment,impacted by the child’s physical and psychosocial status.Both child and parent participants conveyed their anxiety about the uncertainty of the cancer journey,which impaired their ability to meet their ongoing needs.
3.2.1.1.Subtheme 1: Can you tell me what comes next?.The child participants described the multiple needs impacted by their disease and treatment and were frustrated by the unpredictable nature.
“I cried a lot.It was overwhelming.I do not want to get back to…‘Ouch’when I was in the procedure room.And,when I was about to go to the room.Then,nausea and vomiting with chemo.Moreover,I was tired right after that.It was one by one.You ask me what I need.Well,sometimes I need comfort,sometimes I need pain relief,sometimes I need good sleep … but I never know what I need next.”(C3)“I got used to the process.At first,you have chemo;then you get uneasy and tired,then wait for the next round.However,if you catch a cold or develop an even worse thing,then it becomes unpredictable.How long to go to the next round? More meds and more procedures?… Can you tell me what comes next?” (C4)
3.2.1.2.Subtheme 2:Our needs are growing.The parent participants mainly explained the complexity and expansion of their various unmet needs across the cancer trajectory.
“When I look back,our unmet needs were changing all the way.In the first month,my only hope was that any magic meds could help my son’s pain.Then,bad luck!We experienced each adverse effect mentioned by the doctors,especially mucositis,which made him cry all the time and impacted his nutrition.I hate this.Our needs are growing big at each stage.” (P9)
“We need more help dealing with the impact of cancer and chemo,first pain,then fatigue,uncertainty,and fear.Our needs were complex and grew bigger along the way.As parents,we would do better if we had more information and caring skills.Moreover,she(their 12-year -old girl) needs more space for self-reconciliation.She was angry at first,mad at cancer,us,the nurses,and herself.It was like a process of acceptance and healing;our daughter needed more emotional and spiritual support.” (P16)
3.2.2.Theme 2: Communicating with a family focus
The participants called for family-centered communication.From the children’s and parents’perspectives,they must have their voices heard and bring each family member into their daily treatment conversation and decision-making process.
3.2.2.1.Subtheme 1: They only talk to my parents.The child participants stated they must be respected for their knowledge of treatments,understand their feelings,and be given more interpersonal communication opportunities with clinicians.
“I know when to be careful,like avoiding infection after chemo is done and drinking more water with the yellow water (methotrexate).But all these were what the doctors asked my parents to do.They(the doctors)never talk to me directly.They only talk to my parents.I am eager to communicate and be understood.” (C5)
“I hope they can help me know more about my disease during the rounds,like why some meds were used only after eating,why I need blood tests and punctures,and why I have not won the fight(against leukemia) yet.Sometimes they might think I do not understand,but actually,I can understand.In our family,my parents and I have very little talk about my disease.I am ten years old.I am sometimes happy and sometimes sad.I have my thoughts.I like to share it with doctors and nurses if they ask me.” (C3)
3.2.2.2.Subtheme 2: Let each family member have a voice.The parent participants shared their need for more open communication regarding each family member’s thoughts and feelings.However,they did not know how to communicate with their child during the treatment effectively.
“The doctors and nurses are helpful.However,from a family perspective,we do not know how to tell children this information in a way that a child can understand.We want to know what he(their son) will think about the treatment.But we do not know how to start the talk.” (P4)
“I think our family is a whole…although my husband is the head and makes decisions on big things,he is sometimes absent.
I accompany my kid all the time.I know more about my kid’s preferences,her body’s reaction to drugs,her feelings…I hope that doctors will talk and listen to each family member.Moreover,each of us should have a voice in making decisions.Not only me but also the child;she is the one who knows herself best.” (P15)
3.2.3.Theme 3: Providing care beyond the treatment
The participants described their needs beyond merely treating the disease but with more emotional support and information provision that calls for expanded care at each stage.
3.2.3.1.Subtheme 1: I am bigger than my body.The children explained their need for emotional consolidation and information about their prognosis.
“I think being in the hospital is to treat my body’s diseases.But I am still thinking about many other things.I am thinking about what to do with my schoolwork.I do not want to be absent from school,and I want to be an astronaut.People around me only look at the number of my white blood cells and platelets.No one has had a good chat with me.”(C2) “I was thinking about what to do in the future.Am I going to be good or bad?If I am good,can I grow up as big as my friends?If not,will I die?This is so terrible.But what will happen then?What will my parents do then?I am thinking of this all the time.I mean,I am bigger than my body.” (C5)
3.2.3.2.Subtheme 2:There are things beyond treatment.The parents emphasized more attention to transition care,palliative care,and care for the siblings.
“We are a family.My wife and I are separated because of the child’s disease.We have many ‘hollows’ in family.I do not know how to talk to my two children and wife.It seems that our family’s center is around the sick girl.This is bad.I hope the clinicians will meet the needs of our family,like allowing the little sister comes to see him and the opportunity for the family to reunite during the holidays.”(P1)
“There are things beyond treatment.Most kids in the ward spend time watching iPad or phones.The long screening time is not good for their health.But what can we (parents) do? There are hardly any playing activities after the pandemic.I want my son to have more exercise,but I am worried about the potential bleeding.”(P11)
“After moving to the maintenance period,I would like to see preparation for his transition to normal.Hopefully,he will not have any memory of this difficult time.But the meds,the chemo,cancer… I know something will be bad for his body for a long time.We need more information,support,and guidance.” (P17)
“I heard the word‘palliative care’.Most of us parents do not want to hear this word.I think it is related to treatment failure or abandoning our child.What can we do? We do not want to do this.However,people tell us that this care comforts the child and alleviates the symptoms.I would like to know more.In our dark moments,we may need it.” (P22)
3.2.4.Theme 4: Getting support from the community
The participants perceived unsatisfying support from the community.They required community support in their mentality,physical needs,and resources.
3.2.4.1.Subtheme 1: I am not a monster.The children were unhappy about being treated differently.They experienced discrimination,stigma,and stereotype.
“Monsters are living in me,but I am not a monster.I do not want to find my previous buddies to stay away from me in the neighborhood.I do not want special care from my teachers.For I can study hard like my classmates … I think people take me as a monster,different from others.Because only monsters can scare others and do not have good friends.I do not like it.I need support from my surroundings,who treat me as an ordinal boy and care for my body which sometimes is not strong.” (C1)
3.2.4.2.Subtheme 2:We want to connect with the resources near us.There were limited out-of-hospital healthcare services specifically for pediatric cancer patients.There was a lack of coordinated cancer care between the community and hospitals in the health system.
“There is limited support.The one (a national children’s hospital)that treated our girl far from our hometown.When we got back home after a period of intensive treatment,except for one follow-up call from our attending,there was no continuous support.I mean,tell us how to observe the symptoms,cope with our fear of relapse and return to our daily life.” (P13)
“It was hard that we still fully relied on the pediatric oncology service of a children’s medical center.When our daughter was uncomfortable,like nausea and cramping,we could not take her elsewhere but to the same hospital.There would be more than a one-hour drive,and we must wait a long in the clinic.I would say there was a lack of coordinated cancer care between the community and hospitals in the health system.Physicians in my community health care seemed reluctant to take care of a child with cancer or have ‘recovered’ from cancer.Besides medical care,we must connect with the resources near us.Peers group,supporting funds,people in the community that could be turned to in an emergency,etc.” (P23)
4.Discussion
This study provided an in-depth understanding of unmet SCNs from the perspective of Chinese children with cancer and their parents.As conveyed through the quotes,although met with differing views,a combined perspective provided a better reflection of the unmet needs,which pointed to the potential of developing targeted child-parent-friendly interventions.
The revealed themes cover and overlap the domains of the Supportive Care Framework for Cancer Care,which highlights the multi-faceted impact of the disease and treatment on pediatric cancer patients,and their unique needs to be provided with support to improve patient outcomes.Particularly,Chinese children and their parents explained their anxiety about the uncertainty of the varied unmet needs at different stages of their cancer journey.This finding is consistent with previous studies about the multiple impacts of disease and treatment across the pediatric cancer continuum [21,22].Similar to their oversea counterparts [23,24],informational and emotional support appeared to be the most acknowledged categories of unmet needs.Participants also described their experiences with unmet needs in various contexts,e.g.,the intervention of disease and treatment,the child’s growth and development,family dynamics,and perceived service.To better understand each patient’s meaning of the illness,well-designed tailored care should be offered at different stages of the disease trajectory to achieve optimal patient-centered care.
The findings of this study suggest the importance of inviting and integrating the family member’s voice during the child’s treatment.Family-centered care has been welcomed by Chinese pediatric care practice [25].However,impacted by the Chinese culture,parents were less likely to disclose or talk about unfavorable information[26],which may prevent a frank and open talk about the family’s challenges during the challenging period.Besides,this study found that limited communication skills hindered parent-child conversations.Most of the time,children felt “ignored” as they were less talked to when being hospitalized.Listening to the thoughts and feelings of children as the patients are increasingly emphasized.However,literature suggested that most children would not share their symptoms unless they were directly asked [27].There are validated developmentally sensitive child-reported outcome measurements that can help elicit the child’s voice.Meanwhile,artrelated technologies like ‘draw and tell’ can be used to assist the child in effectively describing their needs comfortably[28].
A cancer diagnosis is like throwing a pebble in the water.Study participants stated their needs beyond merely treating the disease but relevant to the physical and psychosocial demands of children and their families around each stage of the treatment.This finding collaborates with previous studies suggesting comprehensive and in-depth supportive care for children with cancer and their families[12].Currently,there are very few reports on the pediatric cancer population needing palliative [29] or care transition [30] in the mainland of China.Due to the past one-child policy,there is a lack of Chinese information about caring for an ill child’s sibling,whose lives are also impacted by cancer [31].These hidden needs should be assessed and explored to better serve this special population.
This study found unsatisfying support from the participants’community.The traditional Chinese culture favors the concept of‘face’,which signifies a person/family’s reputation and self-esteem[32].Influenced by this culture,the cancer stigma may prohibit the deliverance and acceptance of supportive care to Chinese children with cancer.Pediatric cancer healthcare is generally provided by China’s national children’s hospital.Without coordinated care between the community and hospital,this special population’s wellbeing is impacted by disconnected service.This finding calls for a capacity building of pediatric-cancer-related knowledge and skill in the primary care service and close collaboration in the healthcare system in the mainland of China.
This study,however,has limitations.First,although we invited both children and parents,the included participants were not all dyads,as some parents’ children were under the age of eight.Second,there was a limitation in terms of the opinion of the patient’s physician in determining the child’s mental or verbal capacity to participate.Meanwhile,the children might have a limited understanding of their unmet needs due to cognitive capabilities.Third,we did not enroll long-term pediatric cancer survivors,which may impact a complete understanding of this population’s unmet needs.Fourth,the heterogeneous study sample might prevent the generalization of the study to a particular pediatric cancer population.Finally,we did not apply a longitudinal design that prevented us from exploring the unmet SCNs throughout the disease trajectory.
Future researchers may employ a more objective standard for including research to maximize children’s participation.Meanwhile,the enrollment of participants in extended survivorship will allow a more comprehensive understanding of this population’s unmet supportive care needs.In addition,a longitudinal follow-up of a particular cancer type will provide information for developing specific interventions at different disease stages.
Our findings provide fresh insights into supportive care needs in pediatric oncology.The lived experiences shared by the children and parents call for well-designed tailored care which can address the multiple impacts of disease and treatment across the pediatric cancer continuum,understanding each patient’s personal experiences of the unmet needs,encouraging each family member’s voice and a coordinated service in the healthcare system.
5.Conclusion
This study explored the lived experiences of Chinese children with cancer and their parents with unmet SCNs.Understanding their unique needs will help lay the foundation for developing and testing the effectiveness of the strategies to address the specific unmet needs experienced by this population.
CRediT authorship contribution statement
Lei Cheng:Conceptualization,Methodology,Data curation,Writing -review &editing.Ling Yu:Data Curation,Writing -review &editing.Haiying Huang:Data curation,Writing -original draft,Writing -review &editing.Mingxia Duan:Data Curation,Writing -review&editing.
Funding
This study was supported by the China National Natural Science Foundation of China Youth Science Foundation (71904030),China Medical Board Open Competition Grant (#21-427),Taikang Yicai Public Welfare Foundation (ZXJJ-YCGW-2021009),and Fudan Nursing Founding (FNF 202124).
Data availability statement
Authors declare the absence of shared data in the present study.
Declaration of competing interest
The authors stated that there was no conflict of interest in this manuscript.
Acknowledgments
The authors would like to thank all the children and parents who participated in this study.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.09.001.
 International Journal of Nursing Sciences2022年4期
International Journal of Nursing Sciences2022年4期
- International Journal of Nursing Sciences的其它文章
- Effects of equine-assisted interventions on older adults’ health: A systematic review
- Multicenter application of a nursing workload measurement scale in adult hospitalization units
- Exploring social movement concepts and actions in a knowledge uptake and sustainability context: A concept analysis
- Palliative care needs and symptom burden in younger and older patients with end-stage renal disease undergoing maintenance hemodialysis: A cross-sectional study
- Development and validation of a nomogram for predicting the risk of pressure injury in adult patients undergoing abdominal surgery
- Factors influencing the optimal selection of central venous access devices: A qualitative study of health care team members’perspectives