
Effectiveness of statins vs.exercise on reducing postprandial hypertriglyceridemia in dyslipidemic population:A systematic review and network meta-analysis
2022-10-31 07:52LauraAlvarezJimenezAlfonsoMorenoCabaasMiguelRamirezJimenezFelixMoralesPalomoJuanOrtegaRicardoMoraRodriguez
Laura Alvarez-Jimenez,Alfonso Moreno-Cabañas,Miguel Ramirez-Jimenez,Felix Morales-Palomo,Juan F.Ortega,Ricardo Mora-Rodriguez
Exercise Physiology Lab at Toledo,Sports Science Department,University of Castilla-La Mancha,Toledo 45004,Spain
Abstract Background:Individuals at risk of suffering cardiovascular disease(CVD)present with larger increases in blood triglyceride(TG)concentration after a high-fat meal than do healthy individuals.These postprandial hypertriglyceride levels are an independent risk factor for CVD.Prescription of statins and a bout of prolonged exercise are both effective in lowering postprandial hypertriglyceride levels.We aimed to evaluate the comparative effectiveness of statins vs.a bout of aerobic exercise in reducing fasting and postprandial TG(PPTG)concentrations in individuals at high risk of developing CVD.Methods:Thirty-seven studies from a systematic literature search of the PubMed,EMBASE,and Cochrane databases were included in this review.The selected studies conducted trials involving statin therapy(n=20)or a bout of aerobic exercise(n=19)and measured their impact on PPTG levels as the outcome.Two studies analyzed both treatments and were included in duplicate.The meta-analysis was constructed using a random-effects model to calculate the mean difference(MD).The Student t test was used to compare the data sets for statins vs.exercise.Results:Overall,statin and exercise interventions showed similar reductions in PPTG levels,with an MD of-0.65 mmol/L for statins(95%confidence interval(95%CI):-0.54 to-0.77;p<0.001)and-0.46 mmol/L for exercise(95%CI:-0.21 to-0.71;p<0.01).However,statins lowered fasting TG levels more than exercise(MD=-1.54 mmol/L,95%CI:-2.25 to-0.83;p=0.009).Conclusion:Although aerobic exercise is effective in lowering blood TG levels,statins seem to be more efficient,especially in the fasted state.A combination of exercise and statins might reveal a valuable approach to the treatment and prevention of CVD.More studies are required to determine the underlying mechanisms and the possible additive effects of these interventions.
Keywords:Aerobic exercise;Cardiovascular disease;Hydroxymethylglutaryl-CoA reductase inhibitor;Meta-analysis;Metabolic syndrome
1.Introduction
Dyslipidemia(elevated plasma cholesterol,elevated triglyceride(TG)levels,and/or reduced high-density lipoprotein cholesterol levels)contribute to the development of atherosclerosis and cardiovascular disease(CVD).The risk for atherogenic plaque formation increases after ingestion of meals with high-fat content due to the rise in the remnant of TG-rich lipoproteins(i.e.,chylomicrons and very low-density lipoprotein-triglyceride(VLDL-TG)levels).1In healthy men,a high-fat meal reduces flow-mediated vasodilation in association with increases in serum TG levels,suggesting that hypertriglyceridemia could impair endothelial function.2Furthermore,postprandial TG(PPTG)levels 6-8 h after a high-fat meal are an independent predictor of the presence of coronary artery disease.3Upon ingestion of a high-fat meal,individuals with metabolic syndrome(MetS)and dyslipidemia produce more hepatic VLDL-TG and chylomicrons than healthy individuals.4,5Thus,interventions geared to reducing PPTG levels could be clinically effective in populations with adverse atherogenic postprandial profiles.
Statins(i.e.,inhibitors of hydroxymethylglutaryl coenzyme A reductase)are prescribed for the prevention of coronary heart disease in patients with dyslipidemia.Statins stabilize the atherosclerotic plaque,reverse endothelial dysfunction,and decrease thrombogenicity.6The mechanisms of action of statins include reducing liver cholesterol synthesis,which culminates in a reduction in blood low-density lipoprotein(LDL)cholesterol levels.The intracellular hepatic cholesterol levels are under feedback-regulated control,7and when they are lowered by statins,LDL receptors are externalized to the hepatocyte surface to retrieve cholesterol from LDL cholesterol and circulating TG-rich lipoproteins.Thus,statins,in addition to reducing blood LDL cholesterol levels,have the secondary but important role of lowering blood TG levels.8Statins lower PPTG levels more than other antihypertriglyceridemic agents,such as niacin,9but fibrates lower it to a similar10or lower extent.11Publications on the effects of statins on PPTG levels have been accumulating in the past 2 decades,and now there are enough studies to assess the strength of this secondary but clinically relevant effect of statins.12-14
Another useful intervention for reducing the area under the PPTG curve after a high-fat meal is a bout of aerobic exercise.15The mechanisms of this reduction have not been fully elucidated,but they may be mediated by the exercise-induced activation of endothelial lipoprotein lipase(LPL),16-18which clear circulating lipoproteins.Although most exercise studies report reductions in PPTG levels after a high-fat test meal,the variability in the results is large.Factors such as exercise mode(i.e.,resistance vs.endurance),exercise dose(i.e.,duration and intensity),19,20the induced caloric deficit,21and the timing between exercise and the high-fat meal22can affect the PPTG response to exercise.15Although,most exercise studies have been conducted in healthy individuals,a few reports suggest that individuals with MetS and CVD could also benefit from exercise that lowers PPTG levels.23-25An updated account of the effects of exercise on PPTG levels in this population at risk of developing CVD is currently lacking in the literature.
We recently studied the combined effects of a bout of exercise and statin medication on PPTG levels in individuals with MetS.13,14The exercise intervention did not lower PPTG levels;thus,it was not possible to study the combinatory effects of both therapies(i.e.,exercise plus statins).However,there are enough data in the literature to assess the impact of statins or exercise on PPTG levels.Therefore,the purpose of this meta-analysis was to compare the effects of statins with the effects of aerobic exercise on the fasting TG and PPTG-level responses in individuals with CVD risk,thus providing clinicians and exercise physiologists with the most current information,allowing them to decide on the most effective therapy for reducing the atherogenic hypertriglyceridemia that occurs after meals.
2.Methods
2.1.Data sources and search strategy
A literature search was conducted in July 2020 in the following databases:PubMed(National Institutes of Health,National Library of Medicine),EMBASE,and Cochrane.The search was restricted to studies in humans,studies written in English,and studies published before June 2020.Eligible studies included only randomized controlled trials approved by ethics committees.We selected studies using repeated-measures crossover randomized trials.Title,abstract,and keyword search fields were examined in 2 search actions:(1)“Statin”OR“HMG-CoA reductase”and(2)“Exercise”OR“physical activity”.These search actions were combined with the following terms to restrict the search to studies conducting a high-fat test meal:AND“postprandial lipemia”OR/AND“postprandial triglyceridemia”OR/AND“oral fat tolerance test”OR/AND“high-fat meal”.These search actions were further combined with the following terms to restrict the search to individuals with cardiovascular risk factors:AND“overweight”OR/AND“obesity”OR/AND“abdominal obesity”OR/AND“dyslipidemia”OR/AND“hypercholesterolemia”OR/AND“metabolic syndrome”OR/AND“hypertension”OR/AND“cardiovascular diseases”OR/AND“coronary heart disease”OR/AND“type 2 diabetes mellitus”OR/AND“T2DM”.
Two reviewers(LAJ and RMR)independently carried out the identification,screening,eligibility,and inclusion of studies,with disagreement being settled in joint meetings.
2.2.Study selection
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses(PRISMA)statement guidelines.26The inclusion criteria for the studies were as follows:(1)the study included the triglyceridemic response after a high-fat test meal as the dependent variable;(2)the study included treatment with statins or aerobic exercise as the independent variable;(3)the study had to report both fasting and PPTG measurements;(4)the study was a controlled trial;(5)the study included participants who had at least 1 MetS factor(i.e.,abdominal obesity,hypertension,fasting dyslipidemia,or hyperglycemia27),familial hypercholesterolemia,coronary artery disease,or type 2 diabetes mellitus;and(6)the study provided means and standard deviations(or standard errors,medians,or interquartile ranges)for both treatment and control trials,or these data could be derived from graphs.
2.3.Data extraction
We found a total of 37 studies that fulfilled the criteria.Of these studies,20 analyzed the effects of statin treatments,8,12-14,28-43and 19 studied the effects of exercise interventions.9,13,14,20,44-58Two studies analyzed both treatments and were included in duplicate.13,14Study quality was evaluated according to the Physiotherapy Evidence Database(PEDro)scale.59
2.4.Data analysis
The mean difference(MD)of each study was calculated to estimate an overall summary MD,with a 95% confidence interval(95%CI).Data were analyzed using a random-effects model due to the variability in experimental factors.Heterogeneity among studies was tested using the Q statistic and was quantified by I2.Interpretation was as follows:I2:0%-40%=low heterogeneity;30%-60%=moderate heterogeneity;50%-90%=substantial heterogeneity;75%-100%=considerable heterogeneity.60,61z tests were used to compare summary variables.All meta-analyses were performed using Comprehensive MetaAnalysis(CMA)Version 3.3.070 software(Biostat,Englewood,NJ,USA).We also ran paired and unpaired Student t tests to assess within-(fasting vs.PPTG levels)and between-(statins vs.exercise)differences between sets of studies.Last,we used an unpaired Student t test to assess whether the subjects’characteristics between sets of studies(statins vs.exercise)differed.62The correlation between fasting and postprandial variations in response to statins was evaluated using the Pearson correlation coefficient.For this statistical analysis,we used Excel(Microsoft Office 2010;Microsoft,Redmond,WA,USA).
3.Results
3.1.Literature search
The initial online search yielded 404 potential studies.After screening(reviewing the title and abstract),367 studies were dismissed according to the inclusion criteria(PRISMA flow chart)(Fig.1).Upon further analysis,20 studies using statins as an intervention and 19 using exercise as an intervention were included in the final meta-analysis.The included studies enrolled 595 individuals(436 males and 159 females;27% female).A total of 371 participants had a statin intervention and 224 had an exercise intervention.Most studies(34 of 37)used a repeated-measures crossover,randomized control trial design,which reduced most sources of experimental bias.As shown in Table 1,the studies achieved a mean PEDro score of 7.4 of 11.
3.2.Characteristics of the selected studies
A detailed description of each study is provided in Table 2(statins)and Table 3(a bout of exercise).Briefly,the mean age of the participants in the statin and exercise studies was 52±6 years and 45±6 years(mean±SD),respectively(p=0.03).Subjects in the exercise studies presented a higher body mass index(BMI)(BMI=31±3 kg/m2)in comparison to the statin participants(BMI=27±2 kg/m2;p<0.001).Each study used a different high-fat test meal because standardization has not been fully developed.63However,the content of fat as a percent of the total energy of the meal was similar in the studies(i.e.,statin vs.exercise;p=0.21).Studies using the aerobic exercise intervention used primarily a bout of low-intensity(60% maximal oxygen consumption(VO2max))prolonged(>45 min)continuous exercise.In the studies using the statin intervention,the dose of statin varied according to the pharmacological bioavailability of the various statins used(lovastatin,pravastatin,cerivastatin,simvastatin,atorvastatin,or pitavastatin).
3.3.Data analysis
3.3.1.Statin effect
Fig.2 shows the overall results of the statin treatment data set on fasting TG and PPTG levels.Statistically significant reductions were found for fasting TG(MD=-0.53 mmol/L,95%CI:-0.68 to-0.39;p<0.001)and PPTG concentrations(MD=-0.65 mmol/L,95%CI:-0.77 to-0.54;p<0.001).The Student t test showed that the effect of statins on lowering fasting TG levels was similar to their effect on lowering PPTG levels(p=0.503).
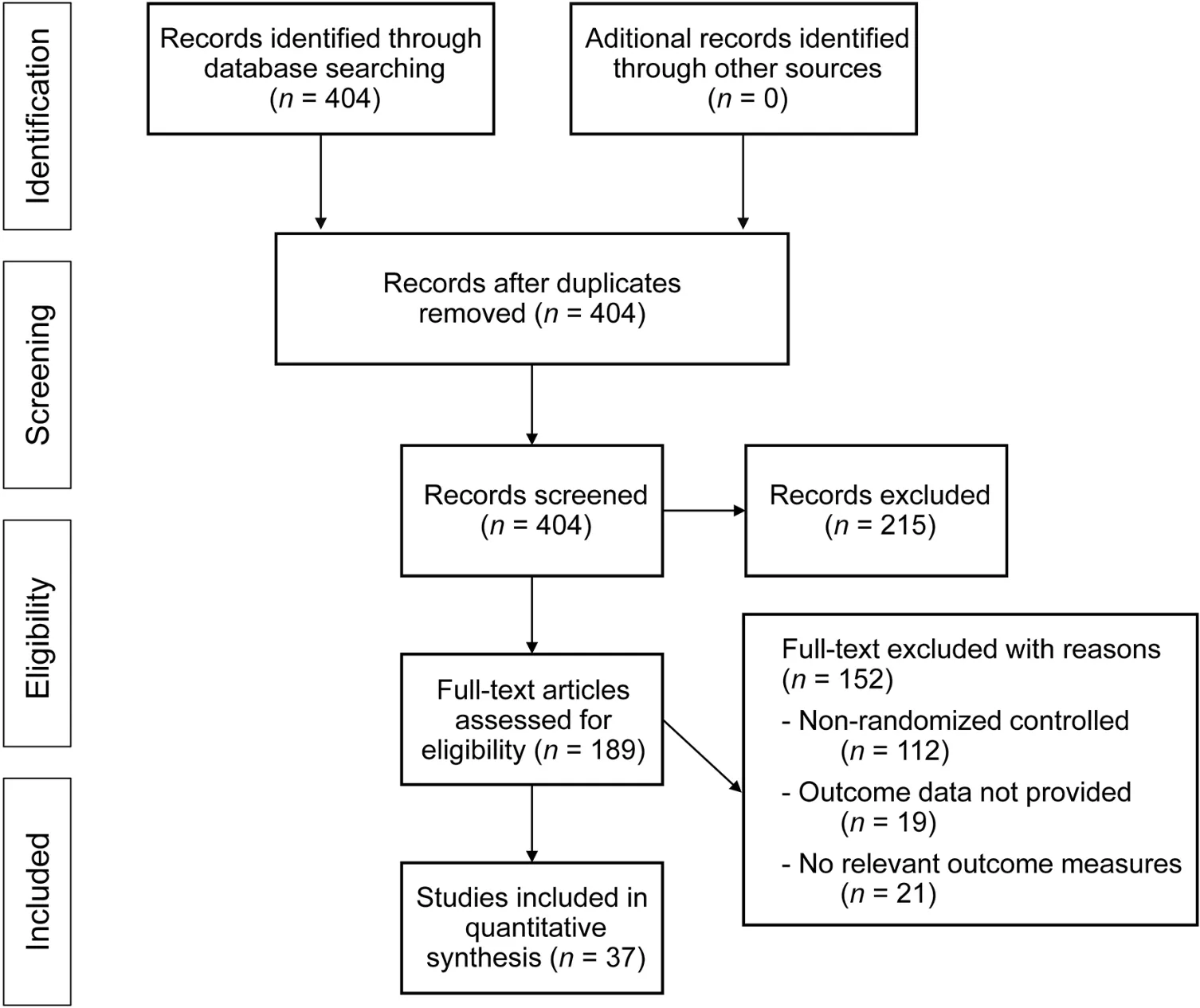
Fig.1.Meta-analysis PRISMA flow diagram.PRISMA=Preferred Reporting Items for Systematic reviews and Meta-Analyses.
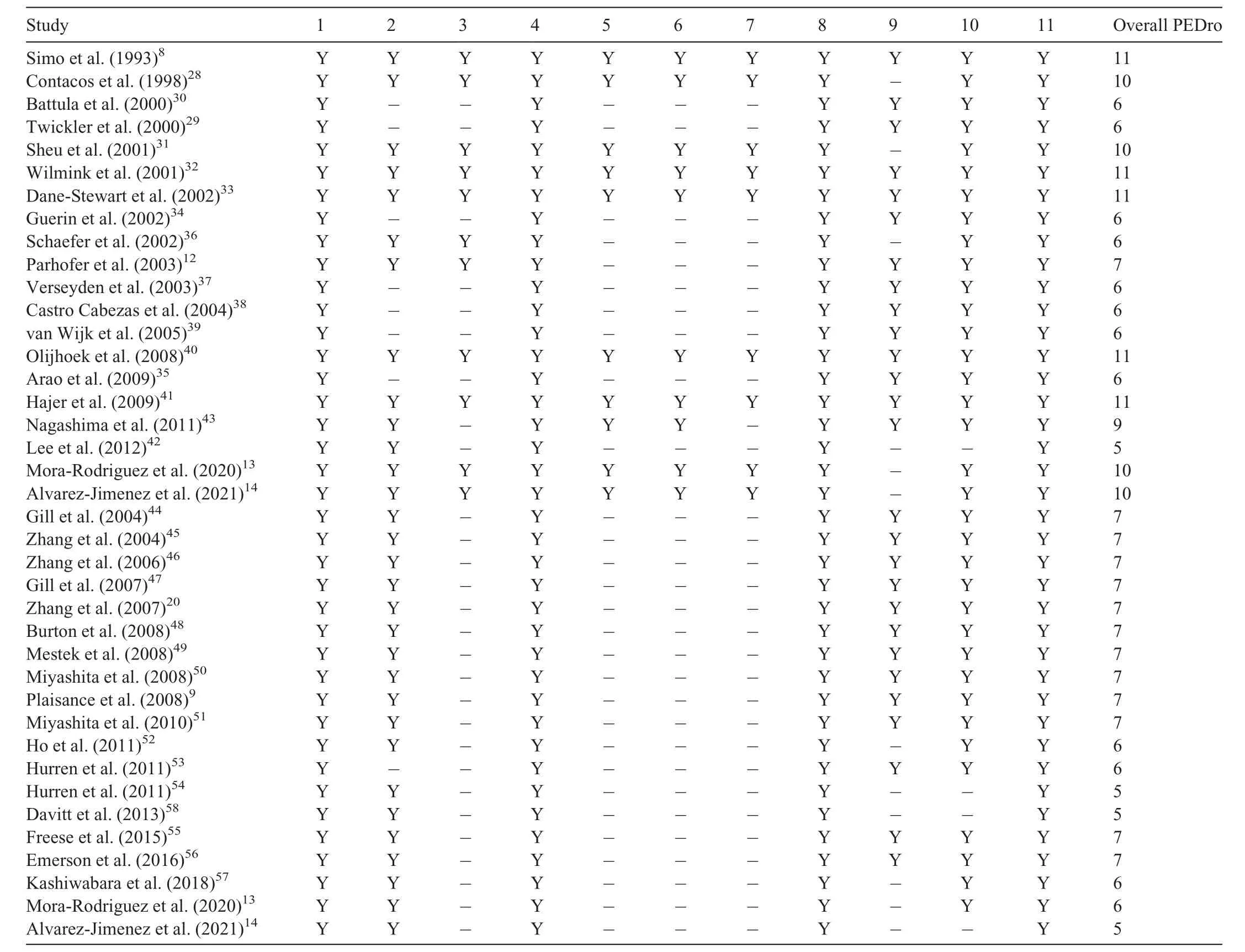
Table 1Quality metrics of included studies.
3.3.2.Exercise effect
The effects of a bout of exercise on fasting and PPTG levels are shown in Fig.3.Exercise induced an MD of-0.46 mmol/L overall mean reduction(95%CI:-0.71 to-0.21)on PPTG levels(Fig.3B).However,the overall effects of exercise on fasting TG levels were less pronounced(MD=-0.22 mmol/L,95%CI:-0.33 to-0.12;p<0.01)but were still statistically significant(z=4.2;p<0.01).The Student t test revealed that the effect of exercise on reducing fasting TG levels was 0.24 mmol/L smaller than the effect on reducing PPTG levels(p=0.015).
3.3.3.Comparison between statin and exercise effect on blood TG levels
The Student t test indicated that the effect of statins on lowering fasting TG was larger than the exercise effect(MD=-1.54 mmol/L,95%CI:-2.25 to-0.83;p=0.009).However,the effect of statins compared to exercise on lowering PPTG levels was not significantly different(p=0.425).
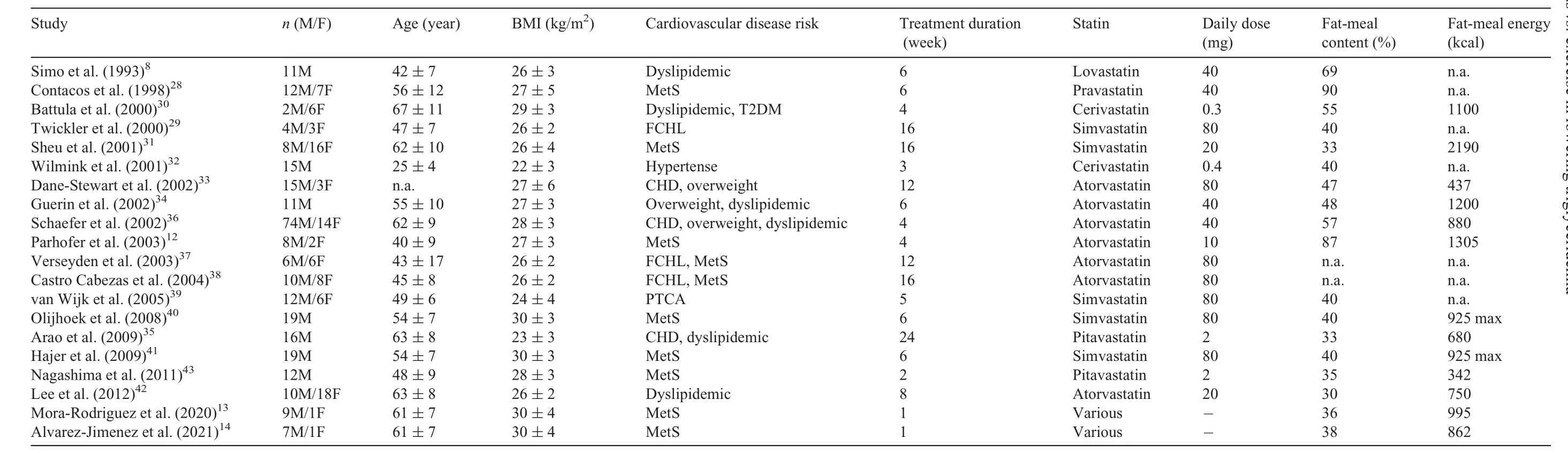
Table 2Characteristics of statins studies.
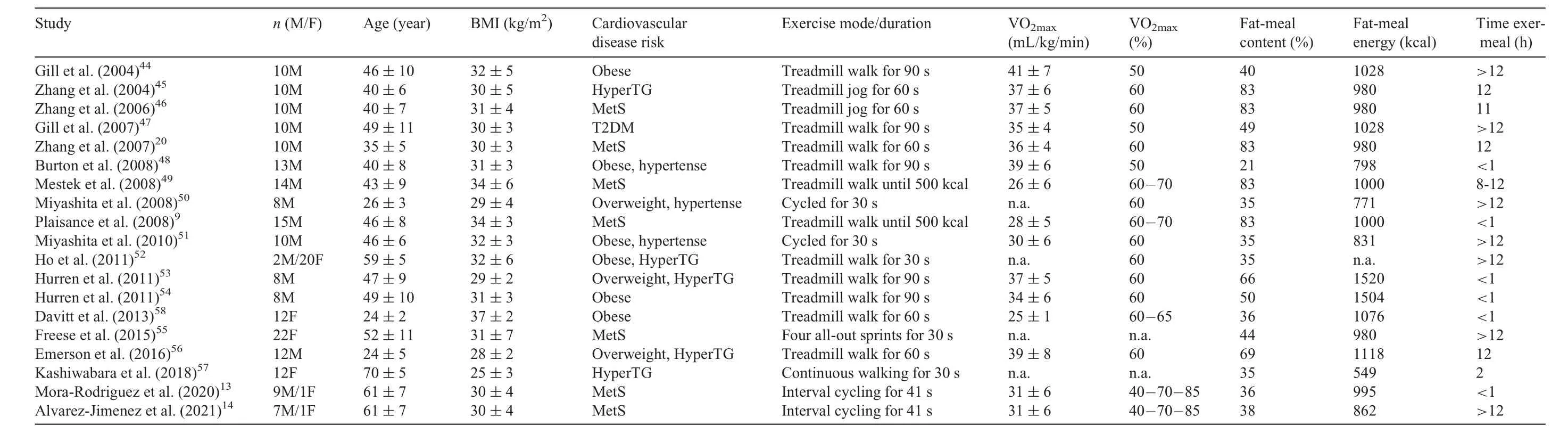
Table 3Characteristics of exercise trials.
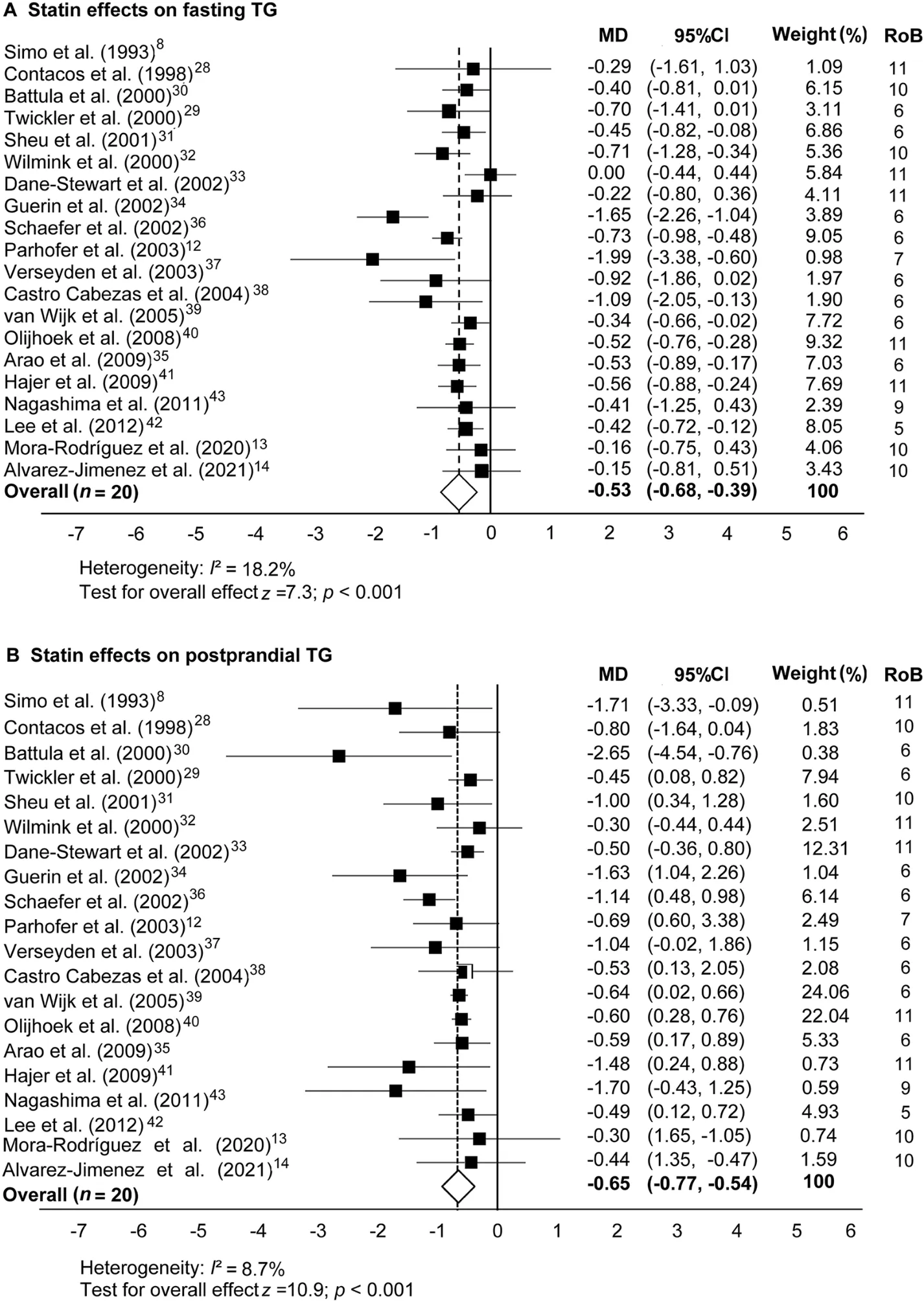
Fig.2.Statin effects on(A)fasting and(B)postprandial blood TG concentrations in comparison to a nonmedicated control trial.Data are MD and 95%CI.95%CI=95%confidence interval;MD=mean difference;RoB=risk of bias;TG=triglyceride.
4.Discussion
This meta-analysis gathered data from 37 randomized controlled trials and included data from 595 participants.It addressed the comparative effect of statin vs.exercise treatments on fasting blood TG levels and on elevations in blood TG levels following a high-fat test meal(i.e.,PPTG levels).PPTG levels have been shown to be a high-risk atherogenic situation predictive of coronary artery disease incidence;2,3therefore,reducing its level is clinically relevant to individuals with increased risk of CVD(e.g.,individuals with metabolic syndrome factors,obesity,type 2 diabetes,or coronary artery disease).Studies included in our meta-analysis attempted to reduce hypertriglyceridemia either by using statins(Fig.2)or by a bout of prolonged aerobic exercise(Fig.3).Both the statin and the exercise data sets revealed significant reductions in plasma TG concentrations in the overall mean in comparison to control trials(i.e.,either no medication or no exercise).The effects were observed in fasting TG as well as in PPTG levels.Thus,both therapies(statins and exercise)can reduce blood TG levels in individuals at risk of developing CVDs.
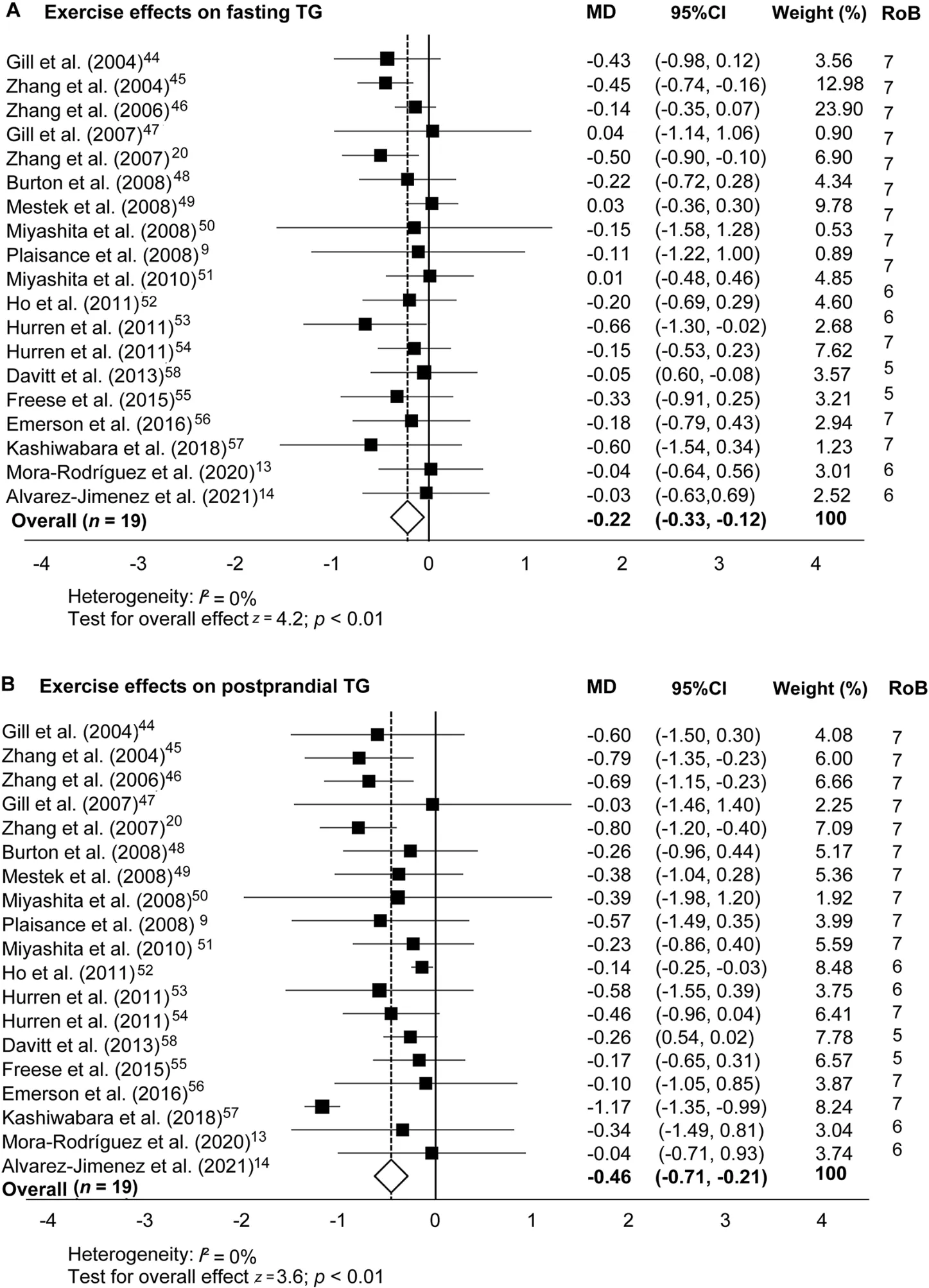
Fig.3.Exercise effects on(A)fasting and(B)postprandial blood TG concentrations in comparison to a nonexercise control trial.Data are MD and 95%CI.95%CI=95%confidence interval;MD=mean difference;RoB=risk of bias;TG=triglyceride.
4.1.Statin effects on PPTG
When statins were used,the mean reductions in fasting and PPTG concentrations were similar(i.e.,0.53 mmol/L vs.0.65 mmol/L;p=0.503)and averaged a 26% to 27% reduction compared to the control trials.The risk reduction for developing CVDs when lowering PPTG levels by this magnitude has not been previously investigated.However,a similar reduction in fasting blood cholesterol reduces mortality and morbidity risks by 22%.64Other authors have reported a strong positive association between the effects of statins on lowering fasting TG levels and their effects on lowering PPTG levels(r=0.487;p=0.05).65,66When we tested that correlation in our meta-analysis using the 20 studies that involved the statin intervention,the correlation did not reach statistical significance(r=0.335;p=0.148).The risk for atherogenic plaque formation is higher after ingestion of a high-fat meal than after an overnight fast;thus,the reported 27% reduction in PPTG levels with statins is suggestive of a new use for statins in reducing risk of mortality due to CVD by lowering PPTG levels.
4.2.Mechanisms of action of statins
The main action of statins is to decrease liver cholesterol synthesis.This reduction induces the liver to upregulate LDL-receptor activity7to seek cholesterol in the blood circulation.These receptors not only reduce circulating LDL cholesterol concentrations but also enhance the clearance of circulating TG-rich lipoproteins(i.e.,VLDL cholesterol and chylomicrons).67Some of the less well-known actions of statins include the postprandial metabolism of apolipoproteins.Statins reduce the incorporation of apolipoprotein-CIII in chylomicrons,liberating the inhibitory actions of apolipoprotein-CIII on LPL.By liberating LPL actions,statins may indirectly increase lipolysis.68,69Statins also stimulate chylomicronremnant catabolism,as reflected by a decrease in apolipoprotein-B48,68,70an apolipoprotein that forms in the intestine during the digestion of a fatty meal.These actions of statins,summarized in Fig.4,are likely to be the cause of the effectiveness of statin pharmacological treatments for lowering fasting TG and PPTG levels.
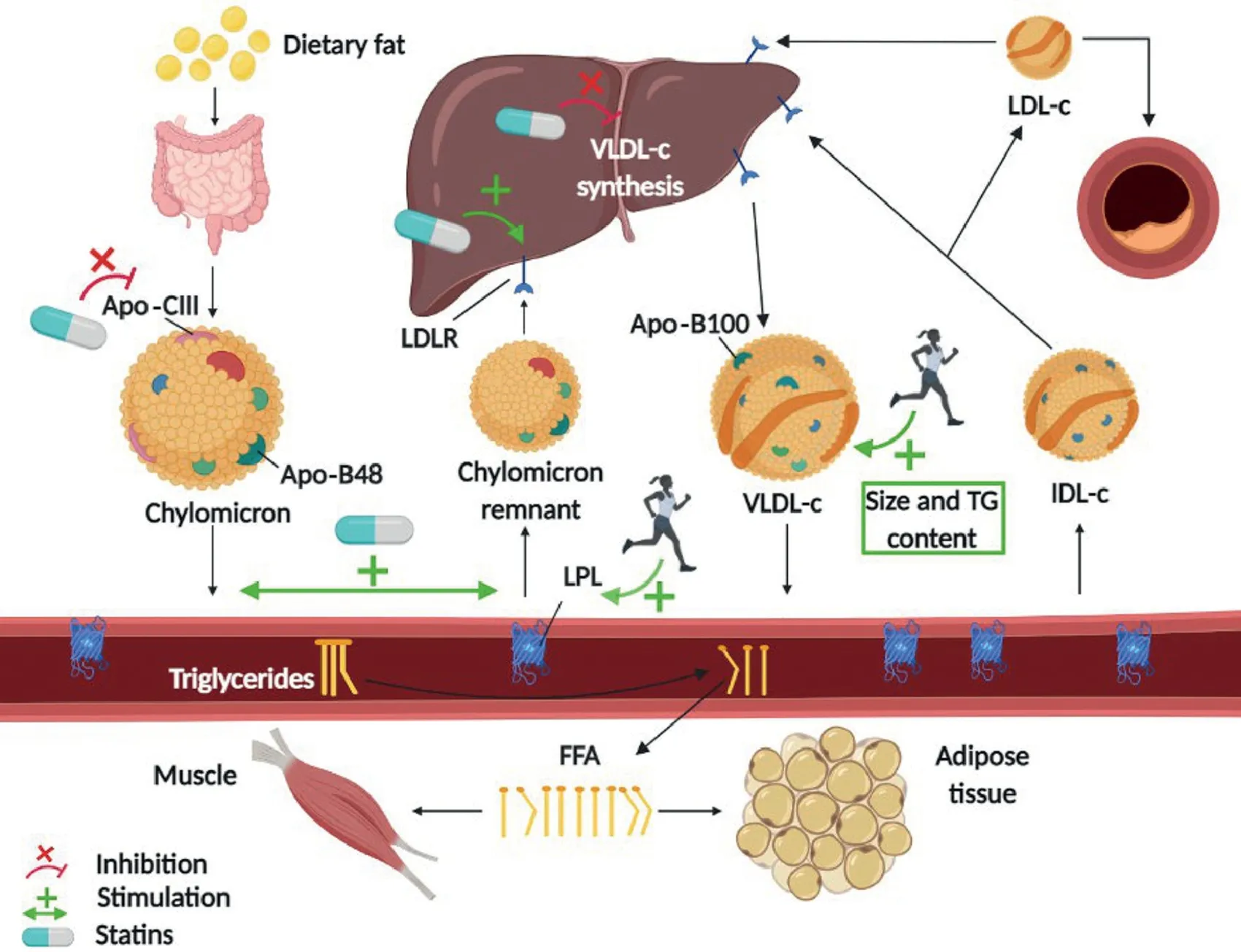
Fig.4.Possible mechanisms of action of statins and aerobic exercise in lowering postprandial triglyceridemia.Green arrows indicate stimulation;red lines indicate inhibition.The statin mechanisms encompass gut-derived apolipoproteins alteration,upregulation of hepatic LDLR and LPL in peripheral tissues,decrease in liver cholesterol synthesis,and increase in circulating triglyceride-rich lipoproteins clearance.The exercise mechanisms involve the activation of skeletal muscle LPL and the increase in triglyceride content of liver-derived VLDL-c particles.Apo=apolipoprotein;FFA=free fatty acid;IDL-c=intermediate-density lipoprotein cholesterol;LDL=low-density lipoprotein;LDL-c=low-density lipoprotein cholesterol;LDLR=low-density lipoprotein receptor;LPL=lipoprotein lipase;TG=triglyceride;VLDL-c=very low-density lipoprotein cholesterol.
4.3.Exercise effects on PPTG
In healthy individuals,a bout of prolonged aerobic exercise(involving high rates of oxygen delivery and consumption)lowers fasting blood TG levels and raises high-density lipoprotein-c concentrations.71The TG-lowering effect of exercise appears to be more powerful after ingestion of a fatty meal(high atherogenic risk)than after an overnight fast(Fig.3).A bout of exercise reduces PPTG levels not only in healthy individuals but also in individuals with dyslipidemia,52MetS,20and other CVD risk factors.58The 19 studies involving exercise interventions included in our meta-analysis suggest that a bout of aerobic exercise decreases PPTG levels by 18% in individuals at risk of suffering CVDs compared to individuals in a nonexercise control situation.Thus,our data suggest that exercise is also an effective therapy acting for lowering PPTG levels.
4.4.Mechanisms of action of exercise
The most frequently proposed mechanism for exercisereducing PPTG levels is the activation of skeletal muscle LPL,which induces the clearance of PPTGs(Fig.4).Activation of muscle LPL peaks 4-18 h after exercise;17,72thus,most studies separate exercise from the high-fat test meal by 8-12 h.However,7 exercise studies included in our meta-analysis waited fewer than 3 h between the high-fat test meal and exercise and found reduced PPTG concentrations.This finding suggests that other mechanisms beyond exercise activation of muscle LPL may be at play73and could involve exercise effects on hepatic metabolism.Some studies have found that exercise increases the TG content of liver-formed VLDL cholesterol particles,74,75which may increase its susceptibility to hydrolysis by LPL76(Fig.4).On the other hand,studies using stable isotopes suggest that a bout of aerobic77,78or resistance79exercise reduces fasting hepatic VLDL-TG secretion which,in turn,could increase chylomicron clearance.73,80
4.5.Comparison of statin vs.exercise interventions
The PPTG reductions in the statin trials(27%)and the exercise trials(18%)were not significantly different statistically.This suggests that for reducing the atherogenic risk in the postprandial state,both statin and exercise interventions could be recommended in a population at risk of developing CVDs.However,we detected that statins and exercise have different effects on fasting TG levels.Statins lowered fasting levels of TGs,and that reduction was maintained during PPTG levels.Reductions in fasting TG levels caused by statins probably contributed to the reduction in PPTG levels.This confirms that statins have a predominant effect in reducing liver VLDL-TG secretion because most of the elevation in blood TGs after ingestion of a fat-rich meal test comes from endogenous liver production.58In contrast,exercise did little to reduce fasting TG levels,although it significantly reduced TG levels when the high-fat test meal was ingested(i.e.,PPTG area under the curve).In fact,the Student t test revealed that exercise-caused reductions in fasting TG levels were significantly lower than the reductions in fasting TG levels obtained with statin treatments(10% vs.26% reduction,respectively;p=0.004).This finding suggests that the effect of exercise on LPL activation is visible only when a large supply of lipoproteins transits the vasculature after a high-fat meal.The intensity of exercise performed in most of the studies included in our meta-analysis(i.e.,around 60% VO2max)was not conducive to episodes of undue fatigue,nor did it represent a risk,even for patients with treated coronary or peripheral artery diseases.However,some side effects,especially at the muscular level,have been reported with statin treatments,which can occasionally result in rhabdomyolysis.81Nevertheless,none of the articles included in our meta-analysis mentioned side effects.
4.6.Limitations
Our meta-analysis is not free of limitations.First,the highfat test meals were not standardized among the studies.In 2011,Kolovou and coworkers63proposed to standardize the high-fat test meal to 75 g of fat,25 g of carbohydrates,and 10 g of protein.However,most of the studies in our meta-analysis that occurred after 2011(Table 1)did not follow this recommendation.The absolute amount of fat ingested in the high-fat test meal could affect the statin or exercise actions through a saturation effect or by insufficient interaction.However,the same high-fat test meal was used in the experimental and control trials of each study,which gives internal consistency to the studies.Second,the set of studies using exercise treatments also suffered from a lack of standardization in the exercise dose.Exercise duration ranged from 30 to 90 min;and,not unexpectedly,caloric expenditure varied up to 3-fold.Furthermore,the time that elapsed between ingestion of the high-fat test meal and the exercise intervention varied among studies.Third,it should be noted that the BMIs of the participants in the exercise studies were higher than the BMIs of participants in the statin studies(i.e.,31 kg/m2vs.27 kg/m2,respectively).Higher BMIs have been correlated with nonalcoholic fatty liver disease,which affects TG metabolism in fasting TG and PPTG levels.82Thus,it is possible that the improvements in both fasting TG and PPTG levels may be biased by the initial condition of the subjects.83Finally,the type of statins and the doses administered were different among the included studies,which could explain the differences in the strength and variability of the responses observed in the studies.84The use of frameworks like Consolidated Standards of Reporting Trials(CONSORT)85should be used to standardize the way researchers report the results of their studies.
5.Conclusion
In the studies we reviewed,both exercise and statin medication reduced PPTG levels,a result that was likely to be due to increased chylomicron and VLDL clearance and/or decreased VLDL cholesterol hepatic synthesis.The magnitude of the effect was similar,although the heterogeneity of the responses was larger when statins were used to lower PPTG levels.Expecting exercise to reduce blood TGs to the levels required to manage patients with severe hyperlipidemia may be unrealistic.However,using exercise as a coadjutant therapy seems a sensible hypothesis.It is unknown whether a combination of statins and exercise would generate additive effects on PPTG levels by increasing chylomicron and VLDL-TG catabolism or by reducing its secretion.14Additional studies are needed to assess whether the beneficial effects of exercise and statin treatments can be combined to reduce PPTG and,if so,improve the clinical treatment and prevention of CVDs.
Acknowledgment
This work was partially funded by a grant from the Spanish Ministry of Economy and Competitiveness(DEP-2017-83244-R)and the European Economic Community.
Authors’contributions
RMR developed the outline of the review,reviewed the literature,and wrote the manuscript;LAJ and JFO also reviewed the literature,contributed to figure preparation and data extraction,and provided suggestions for the original draft and revisions of the manuscript;AMC,MRJ,and FMP read the manuscript and provided suggestions for the original draft and revisions.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
 Journal of Sport and Health Science2022年5期
Journal of Sport and Health Science2022年5期
- Journal of Sport and Health Science的其它文章
- Risk management strategies for the 2022 Olympic Winter Games:The Beijing scheme
- Risk of bias and reporting practices in studies comparing VO2max responses to sprint interval vs.continuous training:A systematic review and meta-analysis
- Association of accelerometer-derived step volume and intensity with hospitalizations and mortality in older adults:A prospective cohort study
- Number of parous events affects the association between physical exercise and glycemic control among women with gestational diabetes mellitus:A prospective cohort study
- Can physical activity eliminate the mortality risk associated with poor sleep?A 15-year follow-up of 341,248 MJ Cohort participants
- Cardiorespiratory fitness,white blood cell count,and mortality in men and women