
An incidental presentation of Herlyn-Werner-Wunderlich syndrome with secondary infertility: A case report
2022-10-11 07:16:42AbiolaOmobonikeAdekoyaAdeniyiKazeemAkisekuAyodejiAnikeOlatunjiMojisolaAdejokeOlusolaBello
Abiola Omobonike Adekoya ,Adeniyi Kazeem Akiseku ,Ayodeji Anike Olatunji ,Mojisola Adejoke Olusola-Bello
1Department of Radiology,Olabisi Onabanjo University Teaching Hospital,Sagamu,Nigeria
2Department of Obstetrics and Gynecology,Olabisi Onabanjo University Teaching Hospital,Sagamu,Nigeria
ABSTRACT Rationale: Herlyn-Werner-Wunderlich syndrome,also known as obstructed hemi-vagina with ipsilateral renal agenesis (OHVIRA)syndrome,is a rare congenital anomaly of the Müllerian and Wolffian ducts.It is often asymptomatic until puberty and is usually misdiagnosed as infertility.Patient concerns: A 39-year-old woman desirous of pregnancy was referred to our radiodiagnosis unit for imaging evaluation on account of secondary infertility.Diagnosis: Incidental discovery of uterine bicornis bicollis and blind-ending hemivagina was noted at hysterosalpingography.Interventions: This necessitated the search for other genitourinary tract anomalies,and ipsilateral renal agenesis was also discovered.Outcomes: A diagnosis of Herlyn-Werner-Wunderlich syndrome was made.Lessons: Magnetic resonance imaging (MRI) is considered the gold standard imaging modality for the assessment of uterine malformations.However,in resource-poor centers where MRI is unavailable,a heightened clinical suspicion with the combination of available imaging modalities is important and reliable in making an accurate diagnosis,hence,successful management.
KEYWORDS: Infertility;Obstructed hemivagina;Renal agenesis;Uterus didelphys;Herlyn-Werner-Wunderlich syndrome
1.Introduction
Herlyn-Werner-Wunderlich syndrome is also known as obstructed hemi-vagina with ipsilateral renal agenesis (OHVIRA) syndrome.It is an extremely rare congenital anomaly of the Müllerian and Wolffian ducts with a triad of uterus didelphys,blind hemivagina,and ipsilateral renal agenesis.Various renal anomalies exist in Müllerian duct anomalies with unilateral renal agenesis constituting 43% of cases[1].The majority of the patients are asymptomatic and discovered incidentally after menarche with non-specific symptoms such as pelvic pain,dysmenorrhea,and palpable pelvic mass from retained menstrual flow[2].Ectopic pregnancy,infertility,and miscarriages with other obstetric complications are less frequently encountered in the long term[3].Given the rarity and low clinical suspicion of this syndrome,we present this case as its diagnosis may be missed in infertility evaluation.
2.Case presentation
A 39-year-old para 1+1married woman desirous of conceiving was referred to our Radiodiagnosis Unit for imaging evaluation on account of secondary infertility of eight years duration.She attained menarche at 13 years and menstruates for three days in a regular 28-day cycle.Since menarche,she experiences cyclical vaginal discharge and mild dysmenorrhoea which improves with analgesia.She attained coitarche at 17 years and had no history of dyspareunia and post-coital bleeding.She had been pregnant twice.The first conception was term and deliveredviaemergency cesarean section secondary to prolonged labor without significant postpartum complications.The second conception three years after was a tubal ectopic pregnancy,necessitating salpingectomy.She had never been on any form of contraceptive method.
Physical and abdominal examination findings were unremarkable.No abnormality was detected in the external female genitalia,introitus,and vagina.Biochemical parameters were normal.Transvaginal ultrasound showed two well-defined,separate,almost symmetric divergent uterine cavities and two separate cervices.Both ovaries were seen as normal (Figure 1A).Abdominal ultrasonography showed an absence of the right kidney and a normal placed left kidney.No renal stones,pelvicalyceal or ureteric dilatation were seen.Hysterosalpingography outlined two endocervical canals opening into two divergent hemi-uteri.A transverse communication at the isthmus and thin linear defects at the right lower endocervical canal were observed,likely surgical scars from previous surgeries.The right vagina was moderately distended and elongated with a cone-shaped blind-end.Wilkinson’s cannula was lodged at the left cervix.The right fallopian tube was demonstrated on the right hemi-uterine horn;however,only the cornual end of the left was seen (Figure 1B).A computed tomography scan of the abdomen and pelvis confirmed the absence of the right kidney with contrast-filled bowel loops at the right renal bed.The left kidney was normal in position and orientation with good excretion (Figure 2A).The left ureter and urinary bladder were normal.Complete duplication of the uterine horns,cervix,and vagina was confirmed with no communication between the endometrial cavities (Figure 2B).
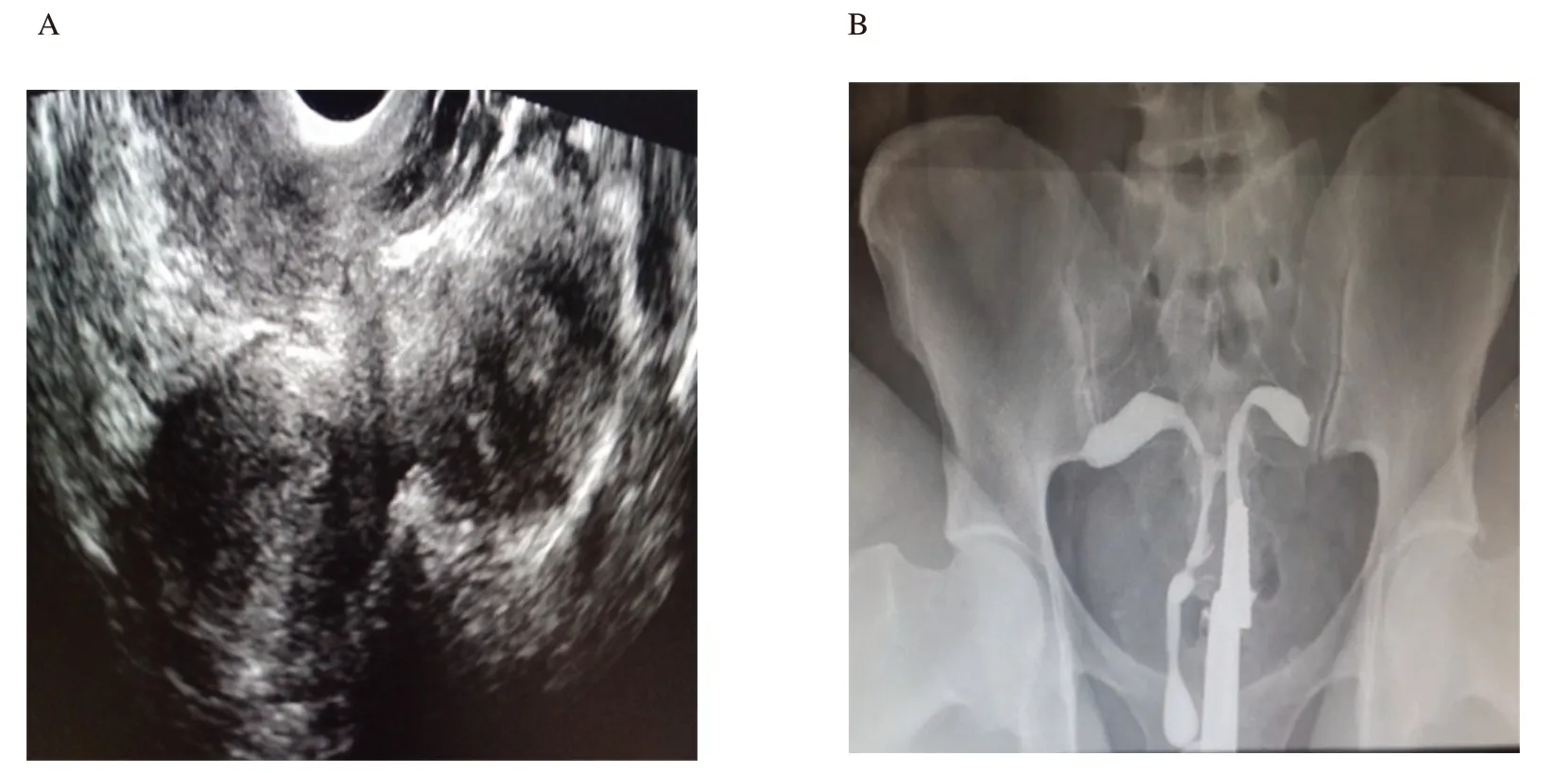
Figure 1.Transvaginal ultrasonography of a 39-year-old infertile woman shows two separate and divergent uterine cavities (A).Hysterosalpingography shows two endocervical canals opening into two divergent hemi-uteri and elongated cone-shaped blind-ending right hemivagina (B).
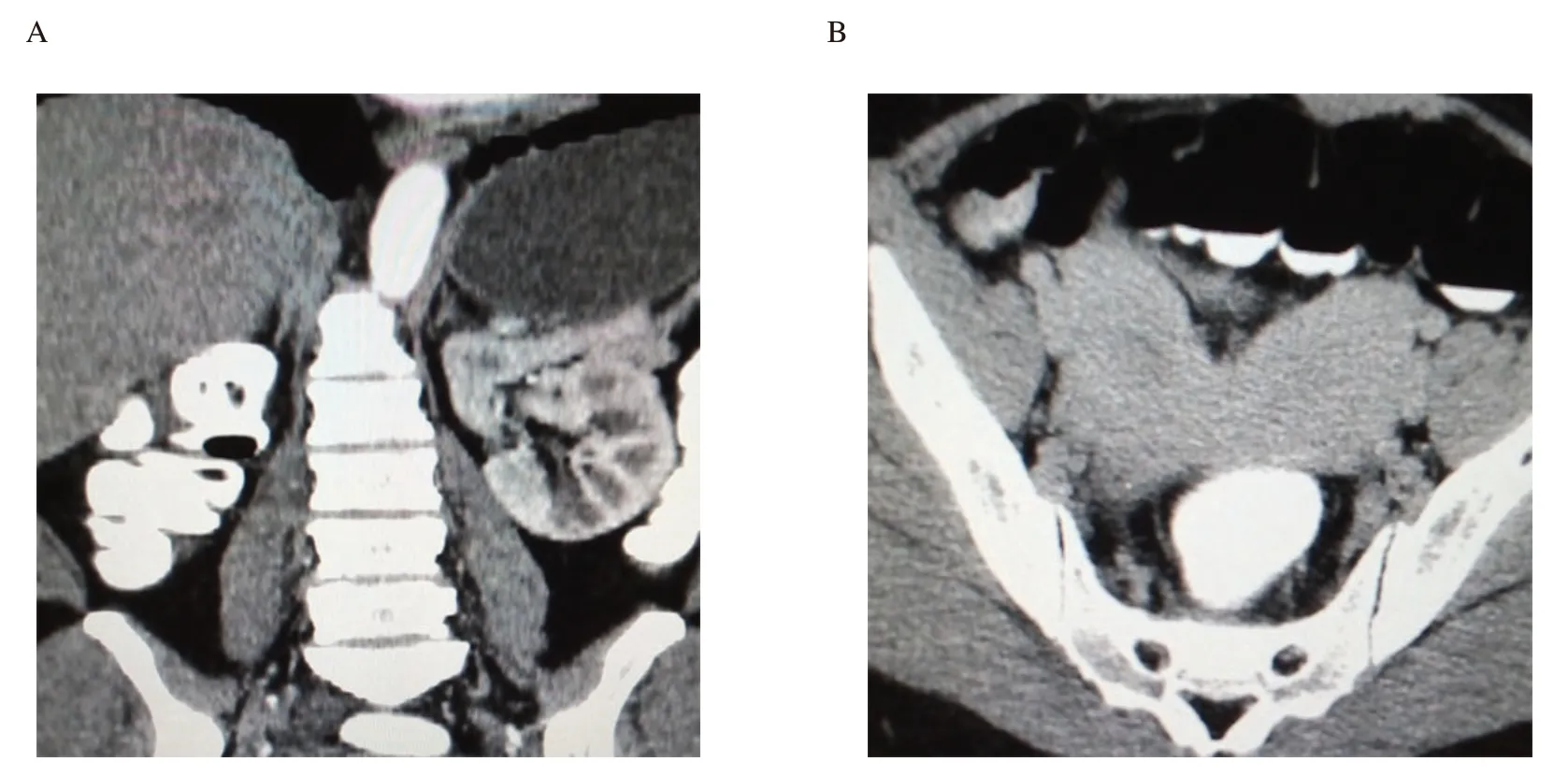
Figure 2.Computed tomography of the abdomen (sagittal view) shows an absent right kidney and a normally placed functioning left kidney (A).A computed tomography scan of the pelvis shows two hemi-uteri and two cervices (B).
A diagnosis of Herlyn-Werner-Wunderlich syndrome was made and communicated.She declined vaginal septum resection of the obstructed hemivagina as a treatment for cyclical dysmenorrhea and vaginal discharge.She was counselled on assisted reproduction,possible adoption,and potential obstetrics complications.
3.Discussion
The etiopathogenesis of Herlyn-Werner-Wunderlich syndrome is unclear;however,it is associated with anomalous development of paramesonephric (Müllerian) and mesonephric (Wolffian)ducts[3].The mesonephric ducts create the kidneys and induce Müllerian duct fusion.Therefore,a developmental anomaly of the caudal portion of the mesonephric ducts results in unilateral renal agenesis[3].Unilateral absence of the mesonephric duct causes lateral displacement and non-fusion of the Müllerian duct with the contralateral duct,resulting in a didelphic uterus[4].The contralateral Müllerian duct develops its hemivagina,whereas the displaced Müllerian duct with no contact with the urogenital sinus forms a blind sac,the imperforate or obstructed hemivagina[5].
Renal agenesis is the commonest associated non-genital anomaly,commonly ipsilateral with the obstructed hemivagina[3,5].A study reported 63.9% and 36.1% distribution on the right and left sides respectively[6].Patients with OHVIRA syndrome usually present after menarche with cyclical pelvic pain and dysmenorrhoea from retained blood in the obstructed hemivagina[2,5,6].However,it may present late and unrecognized with menstruation flowing from the patent unobstructed hemivagina,especially in the presence of uterine communication[1].The presence of normal menstrual flow and absent obstructive symptoms as noted in our patient increases misdiagnosis[5,6].
Although magnetic resonance imaging (MRI) gives a better evaluation of the uterus with additional information on the surrounding structures,its absence should not deter diagnosis[7].Saraveloset al[8] reported increased accuracy of Herlyn-Werner-Wunderlich syndrome diagnosis using a combination of hysterosalpingography and two-dimensional ultrasonography,where MRI,three-dimensional ultrasonography,and laparoscopy were unavailable.Reportedly,hysterosalpingography has 78%sensitivity,90% specificity,and 86% accuracy and two-dimensional ultrasonography has 56% accuracy with low false positive in Müllerian duct anomalies diagnosis[8].Hysterosalpingography demonstrates the uterine outline and fallopian tubes with added information on the presence and level of communication with the hemiuteri and hemicervices,further increasing its diagnostic accuracy.In this index case,the level of communication and the obstructed hemivagina were well visualized during the uterine distension at hysterosalpingography.
Limited studies regarding pregnancy rate among Herlyn-Werner-Wunderlich syndrome before treatment exist as most would have been treated at adolescence.In China,9.8% of the assessed women had term deliveries,suggesting possible pregnancy,although,with an increased possibility of early pregnancy loss[6].Another study suggested that women with uterine didelphys have approximately 80% chance of conception,but with 22% and 74% rates of premature delivery and abortion respectively[5].This is evident in this case,having both term delivery and ectopic pregnancy.
The management of Herlyn-Werner-Wunderlich syndrome is tailored to the patient’s complaint.Vaginal septum resection is indicated in symptomatic women presenting at menarche in preserving fertility[5-7].Surgical interventions such as incision and drainage of abscesses,metroplasty,and hemi-hysterectomy with or without salpingo-oophorectomy may be needed.This will relieve the presenting symptoms,regain their normal anatomical appearance and function as well as prevent long-term complications related to retrograde menstrual blood flow such as hematocolpos,pyocolpos,endometriosis,and pelvic adhesions[9].Two successful pregnancies in uterine didelphic womenviathe split embryo transfer inin-vitrofertilization/intracytoplasmic sperm injection cycles were recently reported[10].
In conclusion,Herlyn-Werner-Wunderlich syndrome may have a late presentation in adulthood,presenting with infertility.Therefore,the detection of reproductive tract congenital anomalies should compel the attending physician to look for associated renal anomalies.A combination of imaging modalities should be employed where MRI is unavailable.This may heighten definitive diagnosis and hence fertility preservation.
Ethics statement
This study was approved by the ethics committee of the local hospital.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of interest statement
The authors declare that they have no competing interests.
Funding
This study received no extramural funding.
Authors’contributions
Abiola Omobonike Adekoya,Adeniyi Kazeem Akiseku,OAyodeji Anike Olatunji,and Mojisola Adejoke Olusola-Bello made substantial contributions to the conception and design of the work.They were involved in data acquisition,analysis,and interpretation of the data.Abiola Omobonike Adekoya and Adeniyi Kazeem Akiseku drafted the work,and revised it substantively,contributing greatly to writing the manuscript.Abiola Omobonike Adekoya obtained the informed consent.Abiola Omobonike Adekoya,Adeniyi Kazeem Akiseku,Ayodeji Anike Olatunji,and Mojisola Adejoke Olusola-Bello revised critically and prepared the final version of the manuscript.Abiola Omobonike Adekoya supervised the whole project.All authors read and approved the final manuscript for publication.
 Asian Pacific Journal of Reproduction2022年5期
Asian Pacific Journal of Reproduction2022年5期
- Asian Pacific Journal of Reproduction的其它文章
- Impact of gamete health on fertilization and embryo development: An overview
- L-carnitine improves developmental competence of buffalo oocytes in vitro
- Evaluation of intratesticular chlorhexidine gluconate for chemical contraception in dogs
- Oxytocin improves testicular blood flow without enhancing the steroidogenic activity in Baladi goats
- Association of the microbial culture of follicular fluid,vaginal swab and catheter tip with β-hCG IVF positive and negative
- Anti-Müllerian hormone and antral follicle count predict ovarian response in women less than 45 years following GnRH antagonist multiple-dose protocol