
Calcium pyrophosphate dihydrate crystals in a 9-year-old with osteomyelitis of the knee:A case report
2022-09-22 01:44WilliamPavlisDavidConstantinescuRajanMurgaiSpencerBarnhillBrianBlack
World Journal of Orthopedics 2022年9期
lNTRODUCTlON
Calcium pyrophosphate dihydrate deposition disease (CPPD),formerly known as pseudogout,is a common inflammatory arthritis that may asymptomatically present as chondrocalcinosis or as episodes of acute calcium pyrophosphate (CPP) crystal arthritis. Increasing age is one of the strongest risk factors for the condition,with the condition rarely seen before the age of 40 and common in patients over 80[1]. In cases where the condition has been identified in patients under 40,risk factors such as genetic predisposition or metabolic disorders are almost always present[2]. In this report,we present the case of a 9-year-old male with no past medical history developing CPP crystals in the synovial fluid of the knee during an episode of osteomyelitis caused by cat scratch injury. The patient’s mother consented to the publication of this case report and accompanying images.
CASE PRESENTATlON
Chief complaints
A 9-year-old,African American male presented to the emergency room accompanied by his mother with right knee pain of 5 d duration.
History of present illness
The patient stated that the pain began after he was scratched by a cat 5 d prior to presentation. His mother noticed her son was not bearing weight on the right lower extremity 2 d after the incident. He described the pain as constant and worsening and aggravated by both passive movement of the knee and weight bearing of the extremity. The patient and his mother denied any history of fever or drainage from the wound but did report antecedent upper respiratory infection symptoms one week prior. He had not trialed NSAIDs or acetaminophen for the injury. The patient was in the 2grade and lived with both parents. The orthopedics service was consulted to rule septic arthritis of the right knee.
There is a story from many years ago of a primary school teacher. Her name was Mrs. Thompson. And as she stood in front ofher 5th grade class on the very first day of school, she told the children a lie. Like most teachers, she looked her students and said that she loved them all the same.
She lives in a castle which lies east of the sun and west of the moon,42 and there too is a princess43 with a nose which is three ells long,44 and she now is the one whom I must marry
History of past illness
In the literature,few reports of CPPD in younger patients have been published,with most being associated with significant relevant co-morbidities[5-9]. The youngest cases of CPPD disease identified from the literature were two 16 year old patients in Germany[9]. The condition’s occurrence in those younger than 55 has been linked to familial hereditary predisposition and metabolic conditions such as hyperparathyroidism,hemochromatosis,Wilson’s disease,hypophosphatasia,and hypomagnesemia[2]. In two prior cases,patients presented with CPPD disease at age 24 and 31 despite no relevant comorbidities or similar familial occurrence[6,7]. The patient in this case similarly demonstrated no metabolic or genetic abnormalities and lacked any similar family history. Acute attacks of CPPD are often found in the setting of acute joint trauma or illness,making this patients concomitant trauma and osteomyelitis a likely inciting factor[2]. However,the pathogenesis of this condition is still not fully understood,and this case highlights the need for more research on the role of join trauma and inflammation on the development of CPPD.
Personal and family history
That Christmas, as I sat looking at my brightly wrapped presents, the shining tree and my happy family, I remembered Lauren. I hoped that she was having just as wonderful a Christmas with her family. I felt like we had helped to keep a little girl s belief in Santa Claus alive.
Physical examination
Focused examination of the right lower extremity demonstrated warmth and swelling across the knee. Superficial scratches were noted across the anterolateral leg. One punctate wound on the lateral knee was noted without erythema or drainage. Thigh and leg compartments were soft and compressible. Significant pain was reproduced with both axial loading and passive range of motion of the knee from 0°-40°. Sensation and motor function were intact in all nerve distributions with palpable distal pulses and brisk capillary refill in all toes.
Laboratory examinations
Initial laboratory studies showed a white blood cell count of 8.9,C-reactive protein of 1.1,and erythrocyte sedimentation rate of 39. The patient had a calcium level of 9.7 and alkaline phosphatase of 209. Due to the clinical concern for septic arthritis,joint aspiration was performed. Aspiration yielded 10 mL of cloudy,viscous,yellow fluid. Follow-up cell counts of the synovial fluid yielded a glucose of 99,protein of 4.9,and a WBC of 7,345 with 59% polymorphic neutrophils. Positively birefringent,rhomboid shaped crystals were present and identified as calcium pyrophosphate dihydrate crystals. Bacterial and fungal cultures of the fluid were both negative for any growth. This synovial fluid analysis was suggestive of an inflammatory origin and a preliminary diagnosis of CPP arthritis was made.
My father will then get very angry, and as the king must answer for what his fool does he will sentence him, even although he has paid his debt, either to answer three questions or to lose his life
Imaging examinations
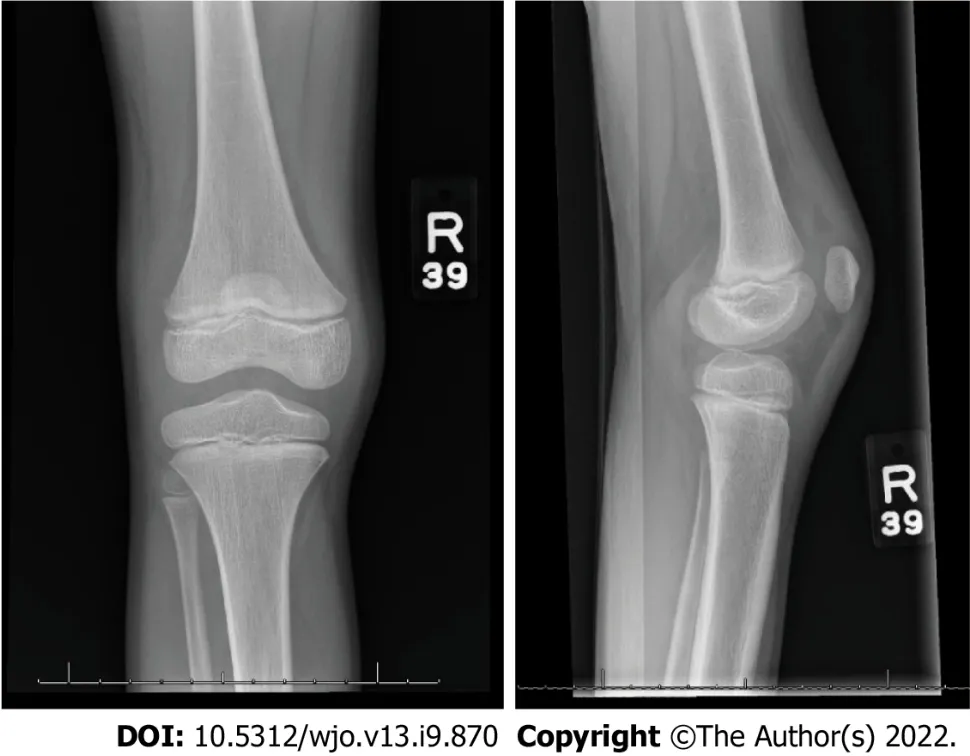
Radiographs of the right knee demonstrated a joint effusion within the suprapatellar recess and trace effusion within Hoffa’s fat pad (Figure 1). No chondrocalcinosis was observed. Follow-up ultrasound of the right knee was performed for comparison,which showed a simple fluid collection in the knee joint.
The patient was placed in an ace wrap for compressive dressing,started on oral ibuprofen,intravenous (IV) ceftriaxone and clindamycin,and admitted for additional work-up. Pediatric infectious disease was consulted and elected to continue ongoing antibiotic management and perform Bartonella titers,which were negative. On the third day of admission,MRI with IV contrast was performed and significant for a focal,intra-synovial area of enhancing,6 mm cortical defect at the lateral border of the lateral femoral condyle (Figure 2). Additionally,a small joint effusion and subcutaneous soft tissue edema overlying the proximal tibia,rim enhancement suggestive of synovitis,and a collection within the inflammatory changes of the vastus lateralis with rim enhancement suggesting small abscess formation were also found.
The patient had no relevant family history,including no history of metabolic disorders such as hereditary hemochromatosis or hyperparathyroidism.

FlNAL DlAGNOSlS
CPPD is a common form of arthritis with still relatively little known about its pathogenesis and prevalence. The condition is rarely identified in those under the age of 40. In this study,we present the rare case of a 9-year-old with CPP crystals in the synovial fluid of the knee during an episode of osteomyelitis. This rare finding presents further questions regarding the pathogenesis of the condition and its role in pediatric joint infection and arthritis. Future diagnostic studies among pediatric populations may identify additional cases of CPP crystals in children and shed new insights on the mechanisms of CPP deposition.
TREATMENT
Antibiotic management was changed to IV ampicillin-sulbactam due to concern for Pasteurella secondary to cat scratch. A diagnosis of CPPD was considered very unlikely due to the patient’s young age,lack of previous episodes or family history of CPPD,and absence of other medical issues considered risk factors for CPPD,such as hyperparathyroidism,hereditary hemochromatosis,chronic kidney disease,or loop diuretic use.
The cook said, You must be a witch, Many-furred Creature, for you always put something in the soup, so that it is much better and tastes nicer to the King than any that I cook
Debridement of the osteomyelitis and needle aspiration of the soft-tissue abscess were not performed due to the small size of the deformities and marked clinical improvement in the patient. Due to this,no cultures or drug sensitives of the abscess or bone were performed. By the fourth day of admission,the patient had remained afebrile,his CRP had decreased to less than 0.5,his right knee had become significantly less edematous,and he no longer endorsed pain or reduced range of motion. After final discussion with the infectious disease team,the decision was made to discharge the patient with a 4-wk supply of oral amoxicillin-clavulanate. The patient did not require physical therapy and was discharged without a walker. The patient was referred for follow-up in the infectious disease to ensure resolution of symptoms and monitor for side effects of antibiotic treatment. The mother was agreeable with the nonoperative management of her son and counseled to return to the emergency room if symptoms recurred.
OUTCOME AND FOLLOW-UP
Pavlis W is responsible for the data curation and write original draft; Constantinescu D is responsible for methodology; Pavlis W,Constantinescu D,Murgai R and Barnhill S participate in the investigation; Pavlis W and Constantinescu D are responsible for the project administration; Black B is responsible for supervision; all authors participate in the manuscript conceptualization,review and editing.
DlSCUSSlON
The Magician s servants hurried after the fresh tracks, but when they came to the bridge, they stood, not knowing which road to take, as the footprints stopped suddenly, and there were three paths for them to choose from
The patient had no past medical history.
CPPD is frequently asymptomatic and believed to be severely underdiagnosed. One study found that CPP crystals were present in the synovial fluid of 30% of patients undergoing knee arthroplasty for osteoarthritis[10]. Diagnosis rates are dependent on methods of diagnosis. The identification of articular chondrocalcinosis on radiographs is a common means of diagnosis; however,studies of prevalence of the condition using this method vary widely based on the type and number of joints examined[1]. The most accurate form of diagnosis remains the identification of positively birefringent,rhomboid-shaped crystals in synovial fluid from the affected joint. In this study,no chondrocalcinosis was observed despite the identification of CPP crystals in synovial fluid.
This study is limited by the short follow-up period. Further follow-up will be required to evaluate the significance of this finding in the setting of this young patient’s acute injury. Additionally,this patient was not formally screened for several metabolic conditions associated with early-onset CPPD,such as hereditary hemochromatosis and hyperparathyroidism. Observation for repeat episodes of acute joint pain or the development of chondrocalcinosis will require further investigation for underlying causes of CPPD. However,this case report successfully presents findings of CPP crystals in a pediatric patient younger than any other previous reported in the literature. Further research could generate key findings on the pathogenesis of these crystals in the setting of trauma and infection in pediatric patients.
CONCLUSlON
A diagnosis of osteomyelitis was made with a rare,incidental finding of calcium pyrophosphate dihydrate crystals in synovial fluid analysis of the knee.
At 6-wk follow-up,the patient was asymptomatic,had completed his course of oral antibiotics,and had returned to prior function. The patient’s mother reported no ongoing noticeable disability or changes in her child. She reported overall satisfaction with the treatment of her child and the quality of care she received from the physician,nursing,and physical therapy staff during her son’s hospitalization.
In this case,we present the rare finding of CPP crystals in the synovial fluid of a healthy 9-year old child with osteomyelitis and a soft-tissue abscess following minor knee trauma. CPPD is a common inflammatory arthritis with a strong association with increasing age. A community prevalence study in the United Kingdom found the mean age of individuals with the condition to be 63.7,with prevalence increasing from 3.7% in those aged 55-59 to 17.5% in those aged 80-84[3]. Cases are very rarely identified in patients under the age of 40. In a study of a region encompassing one million people in Sweden,only 6 of 706 cases were identified in individuals under the age of 34,with the youngest patient being 20[4].
The patient’s mother provided informed consent for the publication of this case report and accompanying images.
All authors report no relevant conflict of interest for this article.
The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
United States
William Pavlis 0000-0003-3465-7871.
She knew this was the last evening she should ever see the prince, for whom she had forsaken119 her kindred and her home; she had given up her beautiful voice, and suffered unheard-of pain daily for him, while he knew nothing of it
Wu YXJ
And the Princess sang a song over him, and this was her song: Child, my child, how sound you sleep! Though your mother s care is deep, You can lie with heart at rest In the narrow brass-bound chest; In the starless night and drear You can sleep, and never hear Billows breaking, and the cry Of the night-wind wandering by; In soft purple mantle5 sleeping With your little face on mine, Hearing not your mother weeping And the breaking of the brine
A
Wu YXJ
 World Journal of Orthopedics2022年9期
World Journal of Orthopedics2022年9期
- World Journal of Orthopedics的其它文章
- Consensus Delphi study on guidelines for the assessment of anterior cruciate ligament injuries in children
- Histological difference in ligament flavum between degenerative lumbar canal stenosis and non-stenotic group:A prospective,comparative study
- Short arm cast is as effective as long arm cast in maintaining distal radius fracture reduction:Results of the SLA-VER noninferiority trial
- Revision anterior cruciate ligament reconstruction:Return to sports at a minimum 5-year follow-up
- Fragility of statistically significant findings from randomized clinical trials of surgical treatment of humeral shaft fractures:A systematic review
- Return to work following shoulder arthroplasty:A systematic review