
Histological difference in ligament flavum between degenerative lumbar canal stenosis and non-stenotic group:A prospective,comparative study
2022-09-22 01:43MantuJainMukundSableAmitPurushottamTirpudeRabiNarayanSahuSudeepKumarSamantaGurudipDas
World Journal of Orthopedics 2022年9期
lNTRODUCTlON
Lumbar canal stenosis (LCS) is a common spinal disorder that affects elderly patients,leading to lower back pain,leg pain,and neurogenic claudication,which rarely ends in paresis[1,2]. Because the ligamentum flavum (LF) covers most of the posterior and lateral part of the lumbar spinal canal,the hypertrophied facets and LF hypertrophy (LFH) are responsible for LCS despite the disc complex,contributing to spinal canal narrowing[2,3]. Thus,morphological and histological changes in developing lumbar spinal canal encroachment must be studied[4,5]. With aging of the global population,a paradigm shift toward symptomatic LCS that requires surgical treatment is observed[6].
LF contains the purest form of elastic tissue among ligaments. These elastic fibers decrease with age and are replaced by collagen fibers[2]. The causes of LFH are multifactorial,including the activity levels,age,and mechanical stress[7,8]. Based on transmission electron microscopy findings,Postacchini[9] concluded that the reduced elasticity might cause bulging of the LF into the spinal canal even in the standing position.
And yet standing10 beside the hospital bed watching the life ebb11 from my sleeping father was painful. I felt like a little girl at his bedside, unable to talk to him yet again. I became fixated with his fingers – fat and soft, lying gently curled beside him. Slowly they transformed from plump sausages to stone – white and immovable. It was his fingers that told me he had gone from this life, not the bleeping of monitors or the bustling12 of nursing staff.
Studies have exhibited a qualitative transformation in the dynamics of the LF components with degeneration[1,6,10-12]. The LFH exhibited loss of elastic fibers,increased content of collagen fibers,and chondrometaplasia,leading to calcification. A few studies have suggested this association of calcification[10],whereas two other studies have suggested a decrease in the elastin/collagen ratio[2,4]. Electron microscopy has revealed fragmentation and changes in the quality of elastic fibers.
The LF,which envelops the spinal canal,is a highly elastic structure that contains four times pure elastin than collagen[6]. If the LF surrounding the spinal canal becomes hypertrophic,it will compress the dural sac containing the cauda equina or the nerve root. Elsberg[13] first reported a case of LFH causing sciatica. Several clinical studies have reported that LFH is the primary pathology in LCS[1,2,4,6-10]. Although surgical excision is the only therapeutic management for patients with LFH in LCS,a deeper understanding of the pathophysiology can encourage future nonsurgical or prophylactic treatment modalities. Thus,the present study attempted to study the pathological changes in LF and compare the LCS and non-LCS study groups.
Therefore,the present study attempted to explain the LF structure histologically in a semiquantitative manner by using advanced imaging software.
MATERlALS AND METHODS
The present prospective study was conducted following the Helsinki Declaration principles and approved by the local institutional review board (T/IM/18-19/43 dated 04/01/2019). Valid written informed consent was obtained from all participants.
Who rides straight forward shall know both hunger and cold.Who rides to the right shall live, though his steed be dead.Who rides to the left shall die, though his steed shall live.
Study population
The present study was conducted in 74 adult patients undergoing lumbar spine surgery between January 2019 and March 2020 in the departments of orthopedics or neurosurgery in a tertiary care center. Patients with characteristic clinical and radiological findings of spinal stenosis were grouped as the LCS study group. Simultaneously,patients with lumbar disc herniation,infective etiology (tubercular or non-tubercular),trauma,and malignancy constituted the non-LCS study group. Patients with prior lumbar surgery were excluded from the study. Clinical details such as age,sex,duration of symptoms,and level of involvement were recorded.
At the sight of these wonders even the scolding tongue ceased, and the woman approached, and took the stones in her hand, setting greedily aside those that were the largest and most costly15
LF samples were obtained from 82 patients who underwent decompressive laminectomy in piecemeal by using a Kerrison's rounger and sent for histopathological assay in neutral buffer formalin. Of these,eight samples were excluded due to sufficient tissue availability. Thus,the final analysis was conducted in 74 patients.
Histology
The harvested LF components were kept in a solution containing 10% neutral buffered formalin for 24 h. The tissues were processed overnight on an automatic tissue processor (Leica Biosystems Ltd.) and embedded in paraffin. Multiple 4-μm thick sections were cut. All sections were stained with haematoxylin and eosin (H & E),Verhoef-Van-Gieson stains (VVG),Masson trichrome stain (MTS),reticulin,and Von-krossa stains.
Of the total,we selected 74 patients. The number of patients in the LCS and non-LCS groups was 34 and 40,respectively. The mean ± standard deviation of age of presentation in the LCS and non-LCS groups was 49.2 ± 8.9 and 43.1 ± 14.3 years,respectively. The difference in fibrosis (= 0.002),elastic fiber degeneration (= 0.01),elastic fragmentation percentage (66.5% ± 16.3%29.5% ± 16.9%),elastic content percentage (26.9% ± 6.7%34.7% ± 8.4%),collagen content percentage (63.6% ± 10.4%54.9% ± 6.4%),reduction of elastic/collagen ratio (0.4 ± 0.10.6 ± 0.1),and ligamentocyte number (39.1 ± 19.153.5 ± 26.9) between the LCS and non-LCS groups was statistically significant. The difference in calcification (= 0.08) and Pearson’s correlation between duration and loss of elastin was statistically nonsignificant. Subgroup analysis exhibited a consistent difference in LF morphology in patients aged ≥ 40 years between the two groups. A similar finding was observed in patients aged < 40 and > 40 years in the non-LCS group.
Light microscopy
The histological evaluation was performed by two experts who were blinded to the nature of the groups. Light microscopy was used to examine LF sections for elastic degeneration,fibrosis,metaplasia (chondroid or osteoid),hemorrhage,and calcification. Elastic degeneration was graded depending upon the percentage of elastic fibers exhibiting degenerative changes and elastin fiber fragmentation (1+:0%-33%,2+:33%-66%,and 3+:> 67% of elastic fibers). Fibrosis was graded as per the criterion described previously[2].
Image acquisition and morphometric analysis
Digital images were obtained using a commercial imaging system (ZEN blue edition on ZEISS Scope A.1 microscope) at 200X magnification for H & E,VVG,and MTS stains in the tagged image file format. For each case,at least two areas from different LF regions were captured randomly. All images were imported in Image J software java windows-64 application (ImageJ bundled with 64-bit Java 1.8.0_172) for morphometric analysis.
The morphological analysis of the digital images of different stains was performed for elastin content (VVG),collagen content (MTS),and the number of ligamentocytes (H & E). The tool was used to estimate the percentage of collagen and elastic fibers,elastic to collagen fiber ratio,number of ligamentocytes,and elastic fiber width. Each parameter was estimated three times,and two independent observers recorded the average.
Statistical analysis
Continuous data are presented as mean ± standard deviation (SD). Differences in the mean between the groups were tested using the independent t test. The Chi-square test was used to compare the categorical variables between the two groups. Correlation between various morphological parameters and duration of symptoms was determined using the Pearson's correlation test for the stenotic group. Subgroup analysis was also performed for patients aged ≥ 40 years and for patients aged < 40 and ≥ 40 years in the non-LCS group. All differences associated with a chance probability of ≤ 0.05 were considered. Data were analyzed using the IBM Statistical Package for Social Sciences ver. 17 (SPSS Inc.,Chicago,IL,United States).
RESULTS
Clinical features
Of the 74 cases,34 cases constitute the LCS group and 40 cases constituted the non-LCS group (Figure 1). The mean ± SD age of presentation in the LCS and non-LCS groups was 49.2 ± 8.9 and 43.1 ± 14.3 years,respectively. The percentage of patients in the stenotic group aged > 40 years was 91%,whereas that in the non-stenotic group was 57.5%. This difference was statistically significant (= 0.001) (Fischer exact test). Although the non-stenotic group included permanent lumbar disc herniation,other pathologies were also observed (Table 1). Single-level involvement was observed in majority of cases. L4-5 involvement was observed in 43.5% patients,followed by L3-4 and L5-S1 involvement (23% patients each). The remaining patients exhibited involvement in L1-2 and L2-3 levels.
Histological differences between LCS and non-LCS groups
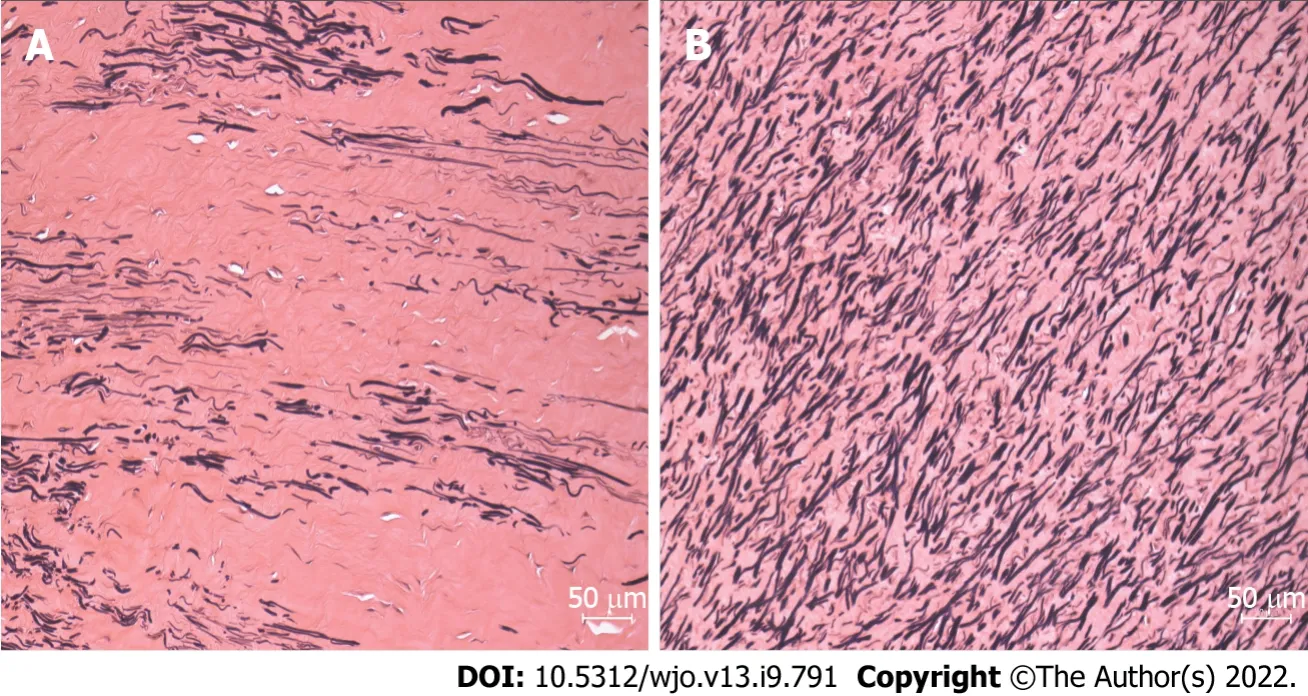
The histological differences in elastin fibers,collagen content,and ligamentocytes were compared between the two groups. The LCS group exhibited higher elastic degeneration and fibrosis than the non-LCS group (= 0.01 and 0.002,respectively) (Table 2; Figures 2-4). On the other hand,the extent of calcification,chondroid metaplasia,and hemorrhage was statistically nonsignificant between the groups.
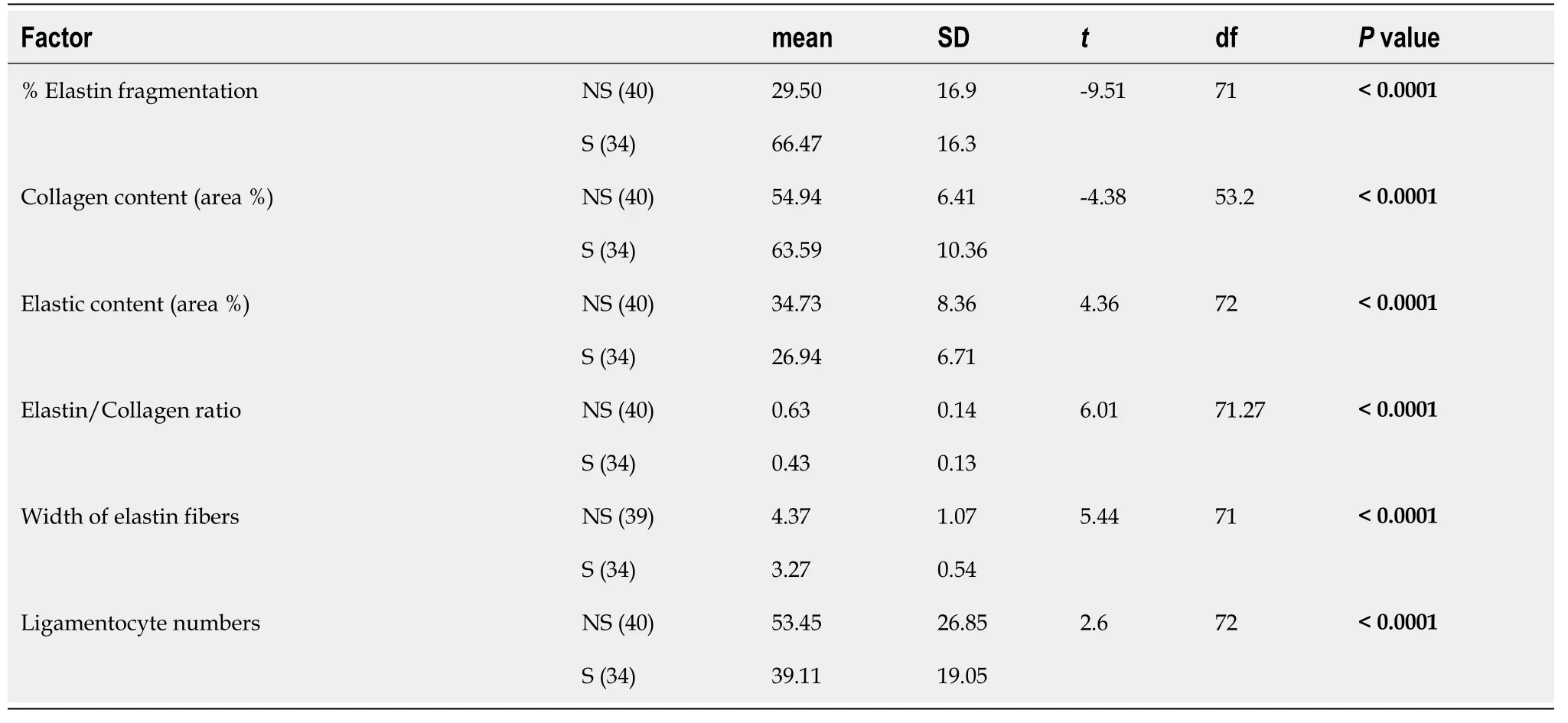
LF exhibited a significant reduction in the elastin content in the LCS group (< 0.0001,independent t test) and an increase in the collagen content (< 0.0001,independent t test) compared with those in the non-LCS group. The elastin/collagen ratio,width of elastic fibers,and ligamentocyte number were also significantly lower in the LCS group than in the non-LCS group (Table 3).
Correlation of clinicopathological features between the LCS and non-LCS groups
The Pearson’s correlation test indicated a moderate correlation between decrease in the number of ligamentocytes and age in both groups (non-LCS-R:-0.52,< 0.001 and LCS-R:-0.578,< 0.001). All other morphological changes were statistically nonsignificant. The duration of symptoms in the LCS group was not significantly correlated with morphological changes in both groups.
The ligamentocyte number was moderately correlated with the elastin content in the LCS group (R:-0.450,= 0.008),(Figure 5). On the other hand,the collagen content was moderately correlated with the elastic content in the non-LCS group (R:-504,:0.001). The LCS group exhibited an inverse correlation between the elastin and collagen contents. However,this difference was statistically nonsignificant.




Subgroup analysis
Subgroup analysis exhibited a statistically nonsignificant difference between the patients aged < 40 years and those aged > 40 years in the LCS group. Additionally,the difference between the LCS and non-LCS groups in the percentage of patients aged > 40 years was statistically significant (Table 4).



DlSCUSSlON
And what was inside after all? Why, nothing but a serpent s skin, which her husband, who was, unknown to her, a magician, put on when he was at work; and at the sight of it the girl was turning away in disgust, when the earth shook violently under her feet, the palace vanished as if it had never been, and the bride found herself in the middle of a field, not knowing where she was or whither to go
Etiology
Sairyo[1] had proposed that LFH occurs due to degenerative changes with aging process,and also due to increased mechanical stress occurring in instability. Wang[14] have experimentally demonstrated increased motion in lumbar spine induced LFH. Chuang[15] have found that agerelated LFH occurred due to activation of the Akt and MAPK (apoptotic) pathways. The authors also postulated that hypertrophy is initiated in all subjects after the second decade of life. Zaki[16] also found that older individuals had some loss and rupture of elastic fibres with abnormal collagen,increase in vascularity and ossification particularly in the lumbar region as compared to the thoracic and cervical spine. Postacchini[9] observed that although older individuals with disc herniation exhibited some elastic fiber loss,the stenotic group of similar age exhibited more collagen and chondroid metaplasia and were strikingly different. However,the authors noted that there was no difference was observed in stenotic changes related to age and listhesis (degenerative),implying that instability does not accelerate hypertrophic changes[9]. The present study also exhibited no LCS-induced morphological changes in the non-LCS group of similar age. Similarly,no difference was observed in the non-LCS group with age < 40 years,whereas a statistically significant difference was observed from age > 40 years.
Levels and age
Sairyo[1] exhibited that LF thickness increased with age; however,the changes with age exhibited spinal level dependence. The increment at L4/5 and L3/4 levels was more extensive than that at L2/3 and L5/S1 levels. Similar changes in magnetic resonance imaging (MRI) were also reported by Kolte[7]. Okuda[10] exhibited that thickening was correlated to calcification,which was prime in LCS. A positive correlation was also observed by authors between calcification and clinical scoring (Japanese orthopedic association scores). The present study did not measure the thickness,either grossly,histologically,or radiologically. The present understanding of LCS has evolved from a pure 'static compression' (dependent on width) to a more “dynamic compression” that arises from the imbalance in LF components rather than actual width. Altun[2] hypothesized that the loss of elasticity is the contributing factor for LF infolding,leading to spinal canal narrowing[2].
Schräder[12] also studied 41 Ligaments in 21 patients and reported single-level stenosis in five patients,bi-segmental stenosis in 24 patients,and stenosis on three levels in 12 patients. Additionally,Hulmani[4] exhibited more double-level stenosis in their series. However,the present study exhibited more single-level involvement (= 32) than double-level (= 7) or multilevel (= 1) involvement. This may be due to the higher age group cohort in the study by Hulmani[4] compared to that in the present study (7249) due to the preferential selection. The present study exhibited that L4-5 was the most common involvement,followed by L3-4. Sairyo[1] proposed that high mechanical stress might be responsible for the preferential increase in thickness at the L4-5 level.
Histology
Altun[2],Hulmani[4],and Reyes-Sánchez[18] exhibited contrasting findings regarding calcification. No statistical difference was observed in calcification between the LCS group and the lumbar disc herniation (LDH) group in these studies.
Okuda[10] and Elsberg[13] observed that nearly all ligaments were calcified in LCS. Calcium deposition within the ligament significantly aggravated the symptoms,and this process increased with age. The increase in the formation of calcium crystals is a significant factor for LF thickening. Okuda[10] observed that the mean age of patients with calcification and those without calcification was 74 ± 2.0 and 68 ± 1.4 years,respectively. Therefore,patients with calcification were significantly older than those in the LCS group. No reactive granulomatous tissue formation was noticed in the calcification focus. Other researchers have reiterated a smooth transition between calcific zones and surroundings[10,17]. Okuda[10] reported focal and dispersion-type calcification in their patients with LCS and correlated calcification with a low clinical score.
Schräder[12] exhibited calcification of all the ligaments,and the patients also exhibited relevant fibrosis with decrease in the elastic/collagenous fiber ratio. Additionally,Sairyo[1] reported that the LCS group exhibited increased LF thickness and fibrosis with reduced elastic fibers. These transformations were more predominant along the dorsal side than those along the middle of the dural side. Sato tel. also found that dorsal side is affected 30 more than the dural side[19] Peng[20] revealed that the dorsal fibers of the LF were subjected to higher stress than the dural fibers that have a fluid-filled tube,which keeps it smooth. Hamdan[11] exhibited that the LCS changes were more in the central portion than in the attachments. Yabe[21] reported a severe reduction in elastic fibres on the dorsal hypertrophied LF. We did not differentiate among the sides as the stenotic effect was due to in-toto changes in LF. Moreover,the LF was removed piecemeal in most of our cases. Hence,such differences were not observed in the present study.
Fuertes[22] were first to comment on the anatomical and fiber arrangements on different layers. The authors realized that aging and repetitive stress altered the elastic fiber organization,causing disarray,derangement,and even complete transformation with no elastic fibers. In the present study,morphologic changes such as diameter irregularity,orientation turbulence,and extent of fragmentation were observed in elastic fibers. A similar finding was observed though electron microscopy in the study by Hulmani[4]. The image software was used to perform the morphometric study based on light microscopy. The present study did not exhibit significant ganglionic cystic changes or chondroid metaplasia despite substantial fibrosis. The present study noted a statistically significant reduction in the elastin percentage,increase in collagen,and reduction in the elastin/collagen ratio. This finding is in contrast to that of other studies. Additionally,a significant change was observed in the elastic fibers (4.37 ± 1.073.27 ± 0.54;< 0.001),fragmentation,and decrease in the number of ligamentocytes. Altun[2] reported that elastic fiber reduction or collagen increase was not significant,except for calcification. Okuda[10] first described elastic fiber degeneration,and it was accompanied by a proliferation of collagen fibers among elastic fibers. Additionally,Hulmani[4] reported findings such as ganglion-like cystic lesion,mucinous degeneration,and vascularization that were confirmed through electron microscopy. Reyes-Sánchez[18] exhibited more cystic degeneration,fibrillar appearance,and hypercellularity in the degenerative listhetic group than in the degenerative stenotic group. These results could be caused by instability rather than a degenerative disease in the spine. Schräder[12] noted that the parallel arrangement of LF elastic fibers was lost in degenerative LCS. This finding is concurrent with that of the present study and the study by Altun[2].
Significant fibrosis was observed in the LCS group in the present study[2,4]. This finding is in contrast to that of Hulmani[4] or Altun[2],and Cheung[23] exhibited a positive correlation between fibrosis and LFH in the LCS group. On the other hand,the developmental stenotic group exhibited paradoxically less fibrosis[23]. Okuda[10] also exhibited graded fibrosis in their LCS patients. However,the correlation with the clinical symptoms of patients was not significant. Additionally,the authors exhibited a large number of chondroid cells in patients with spondylolisthesis[10]. These findings are similar to those of Fukuyama[8],who postulated that unstable lumbar spine accelerates LF degeneration and chondrometaplasia.
She knew it would so soon fade; so she took only a single greenleaf, carried it home, and laid it in her Bible, where it remainedever green, fresh, and unfading. Between the pages of the Bible itstill lay when, a few weeks afterwards, that Bible was laid underthe young girl s head in her coffin13. A holy calm rested on her face,as if the earthly remains14 bore the impress of the truth that she nowstood in the presence of God.
LFH etiology is multifactorial. The morphological transformation that includes reduction in the elastin/collagen ratio,degeneration,fragmentation of the residual elastic fibers,fibrosis,cicatrization,and calcification leads to a loss in elasticity that can infold into the spinal canal,causing narrowing. Future studies can evaluate the correlation between symptom duration and progression of specific changes.
The LCS and non-LCS groups differ in clinical parameters,mainly symptom duration. Histopathologically,the two groups exhibited significant differences in elastin degeneration,fragmentation,elastic/collagen ratio,fibrosis,and number of ligamentocytes. However,calcification was not significant between the groups.
Limitation
The present study exhibited that morphometric findings can be studied satisfactorily even in the absence of an electron microscope,which can be reproduced even in less sophisticated setups. However,it could not differentiate between the dorsal and dural aspects as we removed the LF piecemeal and not as a whole. The central and peripheral parts could not be segregated,which could allow more in-depth understanding,particularly of chondroid metaplasia. Clinical scoring,occupational activity,and MRI measurement were also ignored to keep the study simple. Additionally,gene expression was not studied in the present study.
CONCLUSlON
Several inflammatory cytokines have been studied which are responsible for the growth and reproduction and some of these plays’ crucial role in inflammatory response and progressive LF fibrosis[24]. However,we have not studied any such markers.
ARTlCLE HlGHLlGHTS
Research background
Ligament flavum (LF) hypertropy is the main etiopathogenesis of lumbar canal stenosis (LCS). The purely elastic LF undergoes a morphological adaptation including a reduction in the elastic fibers and a consequent increase in the collagen content,fibrosis,cicatrization,and calcification. However,the morphometric analysis can delineate the LF in patients with LCS from those without LCS,which would help in better understanding LCS pathogenesis.
Research motivation
Institutional research grant (AIIMS Bhubaneswar).
Research objectives
To compare the histopathological changes in LF between the degenerative LCS and non-stenotic (non-LCS) group.
For a long time I work with the fish ponds and met many customers, I knew some customers with fish keeping experience, some were poor or without any fish knowledge. If the customer is quietly looking at the same pond s fish for a little longer, bent1 or hand against the pond edge to have a detailed2 look, the meaning is they are with some fish keeping experience. If the customer looked at the fish and loudly talks, pointing at this one and that one randomly3, the meaning is they are without fish keeping experience or poor. I have seen the young man hadn’t looked at any fish for a little long while of the time. So I thought he was a poor one.
Research methods
The present prospective study was conducted in 82 patients who were divided into two groups,namely LCS and non-LCS. Demographic details of the patients such as duration of symptoms,level of involvement,and number of segments were recorded. The LF obtained from both groups was histopathologically examined for the fibrosis score,elastic fiber degeneration,calcification,and chondroid metaplasia. Morphometrical details included a change in elastin and collagen percentages,elastin/collagen ratio,elastic fiber fragmentation,and ligamentocyte numbers. All parameters were compared between the two groups by using the independent t test,Chi-square test,and Pearson’s correlation test.
Research results
I said secretly, because the Fairy had warned the Queen that the King was a magician; and as from time immemorial there had been a standing5 feud6 between the Fairies and the Wizards, he might not have approved of his wife s visit
Research conclusions
The quality change in elastin fibers and an increase in the collagen content and fibrosis cause loss of elasticity in LF,contributing to LCS pathogenesis. However,calcification did not play a significant role in LCS pathogenesis.
By now, Mrs. Thompson realized the problem and she was ashamed of herself. She felt even worse when her students brought her Christmas presents, wrapped in beautiful paper and tied with pretty ribbons, except for Teddy s. His present was clumsily() wrapped in the heavy, brown paper that he got from a grocery bag.
Research perspectives
Tne study compare the histopathological changes in LF between the degenerative LCS and non-stenotic (non-LCS) group.
THERE was a miller1 who left no more estate to the three sons2 he had than his mill,3 his ass,4 and his cat.5 The partition was soon made. Neither scrivener6 nor attorney7 was sent for. They would soon have eaten up all the poor patrimony.8 The eldest had the mill, the second the ass, and the youngest nothing but the cat.9 The poor young fellow was quite comfortless at having so poor a lot.
That was a marvellous flute! Its sound was as thrilling as thewhistle of a steam engine; in fact it was much stronger, for itsounded and was heard in the yard, in the garden, in the wood, andmany miles round in the country; at the same time a storm rose androared; Everything in the right place
Jain M,Sable B,Tirpude AP,and Sahu RN conceived the idea; Jain M got the ethical clearance and grant for the study; Jain M,Sahu RN,and Das G collected the sample; Sable M and Tirpude AP performed the histological analysis; The data were compiled by Jain M and Samanta SK; Sable M and Jain M performed the statistical analysis; Jain M,Samanta SK,and Das G wrote the manuscript,whereas the other authors provided critical inputs; All authors have read and agree to the content of the manuscript.
The research is motivated due to high footfall of these patient on Orthopedic outpatient department. An interdepartmental meeting was made to analyze these patients and funds were provided by the institute.
The study was reviewed and approved by the Institutional ethics committee of AIIMS Bhubaneswar (T/IM/18-19/43 dated 04/01/2019).
It doesn t matter when. I m sure the Addisons are nice people, but I m not going to waste an evening socializing with people who don t have any eligible3 daughters.
All patients gave informed consent.
There is no conflict of interest.
The children danced round the grave, and the eldest8 of the boys among them, a practical youngster of seven years, made the proposition that there should be an exhibition of Puggie s burial-place for all who lived in the lane; the price of admission was to be a trouser button, for every boy would be sure to have one, and each might also give one for a little girl
Mom put the money back in the envelope. We didn’t talk, just sat and stared at the floor. We had gone from feeling like millionaires12 to feeling poor. We kids had such a happy life that we felt sorry for anyone who didn’t have our Mom and our late Dad for parents and a house full of brothers and sisters and other kids visiting constantly13. We thought it was fun to share silverware and see whether we got the spoon or the fork that night. We had two knives that we passed around to whoever14 needed them. I knew we didn’t have a lot of things that other people had, but I’d never thought we were poor.
Participants gave informed consent for data sharing.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
India
Mantu Jain 0000-0003-3848-4277; Mukund Sable 0000-0002-5364-1464; Amit Purushottam Tirpude 0000-0003-0223-2270; Rabi Narayan Sahu 0000-0003-1429-2123; Sudeep Kumar Samanta 0000-0003-3543-4485; Gurudip Das 0000-0001-7887-5526.
Liu JH
A
Liu JH
 World Journal of Orthopedics2022年9期
World Journal of Orthopedics2022年9期
- World Journal of Orthopedics的其它文章
- Consensus Delphi study on guidelines for the assessment of anterior cruciate ligament injuries in children
- Short arm cast is as effective as long arm cast in maintaining distal radius fracture reduction:Results of the SLA-VER noninferiority trial
- Revision anterior cruciate ligament reconstruction:Return to sports at a minimum 5-year follow-up
- Fragility of statistically significant findings from randomized clinical trials of surgical treatment of humeral shaft fractures:A systematic review
- Return to work following shoulder arthroplasty:A systematic review
- Evolution of evidence in spinal surgery – past,present and future Scientometric analysis of randomized controlled trials in spinal surgery