
Fragility of statistically significant findings from randomized clinical trials of surgical treatment of humeral shaft fractures:A systematic review
2022-09-22 01:44StephenCraigMorrisAnirudhGowdAvineshAgarwallaWesleyPhipatanakulNiravAminJosephLiu
World Journal of Orthopedics 2022年9期
lNTRODUCTlON
Humeral shaft fractures represent approximately 3% of all long-bone fractures[1] with an incidence around 13 per 100000 people per year[2]. While the vast majority may be managed nonoperatively[1-5],surgical treatment is generally indicated for open fractures,polytrauma patients,ipsilateral humeral shaft and forearm fractures (floating elbow),segmental fractures,and cases of failed treatment in functional brace[3]. However,it is important to note that there are currently no defined gold standards for the treatment of humeral shaft fractures[6,7]. Surgical treatment options include external fixation,open reduction and plate osteosynthesis (ORPO),minimally invasive plate osteosynthesis (MIPO),and intramedullary nail (IMN). Implant options for both ORPO and MIPO include dynamic compression plate (DCP) and locking compression plate (LCP). Numerous recent systematic reviews,meta-analysis,and network meta-analysis (NMA) review papers have been published aiming to determine the efficacy of these treatment options in order to provide reliable evidence to guide clinical decision making[6,8-13]. Based on the lack of consensus from the existing literature regarding surgical treatment of humeral shaft fractures,this manuscript aims to further assess the quality of the literature that guides treatment decisions by employing a new metric,the fragility index (FI). The FI has been introduced to further evaluate the robustness (or fragility) of randomized control trial (RCT) results[14,15].
The evaluation of RCTssystematic review,meta-analysis,or NMA represents level I evidence; however,the fact remains that many RCTs in orthopaedics,despite demonstrating statistically significant effects,are limited by small sample sizes and few outcome events[16-19]. Clinical studies are classically evaluated for statistical significance in the form ofvalues,and 95% confidence intervals,which help determine how likely observed effects would occur based solely on chance[20-22]. The FI represents the required number of participants in the RCT whose outcome would have to change from nonevent to event in order to convert a statistically significant result to nonsignificant. The FI is calculated by sequentially calculating thevalue using the Fisher exact test while changing an outcome from nonevent to event between cycles until the calculatedvalue is not significant,or> 0.05. Basically,the FI quantifies how many patients would be required to switch outcomes in order to change the study conclusions. In the case where a study reports a statistically significant result,but the FI is calculated to be zero,this would indicate that the Fisher's exact test did not find avalue < 0.05,whereas the statistical method used in the paper did. In addition,the FI may be lower than the number of patients lost to follow-up,limiting the confidence one may have in the study conclusion[14]. The higher the FI the more confidence the reader can have that the result is robust. While there is no defined cut off for the FI value,if the FI is zero or less than the number of patients lost to follow up,then any statistically significant result should be considered fragile and interpreted with caution. By applying the FI metric to RCTs evaluating surgical outcomes in humeral shaft fractures we can determine how much confidence these studies should be given in guiding treatment decisions.
Puss was so sadly terrified at the sight of a lion so near him that he immediately got into the gutter, not without abundance of trouble and danger, because of his boots, which were of no use at all to him in walking upon the tiles. A little while after, when Puss saw that the ogre had resumed his natural form, he came down, and owned he had been very much frightened.
Mom and Dad were happily talking about the chain of events that had led them to this place. That surgery, her Mom whispered. was a real miracle. I wonder how much it would have cost?
Due to this added value,the FI has been gaining traction in the literature with studies published across numerous medical specialties[15,23,32-35,24-31],in addition to orthopaedic subspecialties[25,36-40]. This valuable,new tool,the FI,can serve to increase our understanding of the literature regarding treatment of humeral shaft fractures,aiding in clinical decision making. Our primary objective was to determine the robustness of statistically significant findings in RCTs of the surgical treatment of humeral shaft fractures by systematically applying the FI. We sought to accomplish this objective by testing our hypothesis that the median FI in these RCTs would be less than the number lost to follow up and therefore would indicate fragile results.
MATERlALS AND METHODS
The cumulative FI values for each outcome within each study are listed in Table 3 and presented graphically (Figure 2). The FI was found to be 0 for all individual outcomes except for iatrogenic nerve palsy in 1 out of 14 studies (higher rate with DCP compared with IMN),malunion in 1 of 7 studies (higher rate in IMN compared with LCP),shoulder impingement in 4 of 10 studies (higher rate in IMN compared with MIPO or DCP),elbow stiffness in 1 of 4 studies (higher rate in DCP compared with IMN),and secondary surgeries in 1 of 11 studies (higher rate with IMN compared with DCP). When totaling all complications for each study,the FI was >0 in 2 out of the 15 studies,with higher complication rates in IMN compared with MIPO or DCP. Overall,the FI was greater than 0 in only 9.8% (9/91) and was greater than the number lost to follow up in 2% (2/91) of outcomes studied.
Now ten years later am sitting here going threw some of my old thing and at the bottom of my old jewelry6 box I found that letter that you wrote me a couple years ago it read:
Data was extracted from the included studies by individual review of each study by the primary author. Accuracy of data extraction was confirmed by independent review by the remaining authors separately,with any discrepancy resolved by group consensus. An electronic data form was developed and the following data were extracted for each included study:First author,journal,publication year,comparison groups,randomization parameters,initial sample size,total patients lost to follow up,final sample size,patients in study group 1,patients in study group 2,patients lost to follow up in group 1,patients lost to follow up in group 2,presence of power analysis,as well as the number of events for each outcome in each group and reported p-value for dichotomous outcomes (delayed union/nonunion,iatrogenic radial nerve palsy,infection,malunion,shoulder impingement,elbow stiffness,secondary surgeries). For our study lost to follow up included any patients initially enrolled in the study but not included in final analysis for any reason. The total number of events for all complications was defined as the sum of delayed union/nonunion,iatrogenic radial nerve palsy,infection,malunion,shoulder impingement,and elbow stiffness. The total number of events for all complications was calculated for each study group within each included study.
But sitting quietly in the back, with tears streaming down his face, an ordinary carpenter realized the Master Carpenter had used him in an extraordinary way.
For each study the FI was then calculated for all complications,secondary surgeries,as well as each complication individually. The FI was calculatedthe method described previously by Walsh[14] using a publicly available calculator found at http://clincalc.com/Stats/FragilityIndex.aspx. After inputting the total number of patients in the control group,experimental group,control group with primary endpoint,and experimental group with primary endpoint,this tool calculates thevalue using the Fisher exact test. If thevalue is significant (< 0.05),the tool incrementally converts 1 outcome from nonevent to event and recalculates thevalue until thevalue increases above 0.05 and the result becomes insignificant. The methodological quality of each RCT was also assessed by calculating the Jadad scale[42],also known as the Oxford Quality Scoring System,for each trial.
Then the serpent made a rush at the youth with wide open jaws13 to swallow him at one gulp14, but the young man leaped aside and drew his sword, and fought till he had cut off all the seven heads
RESULTS
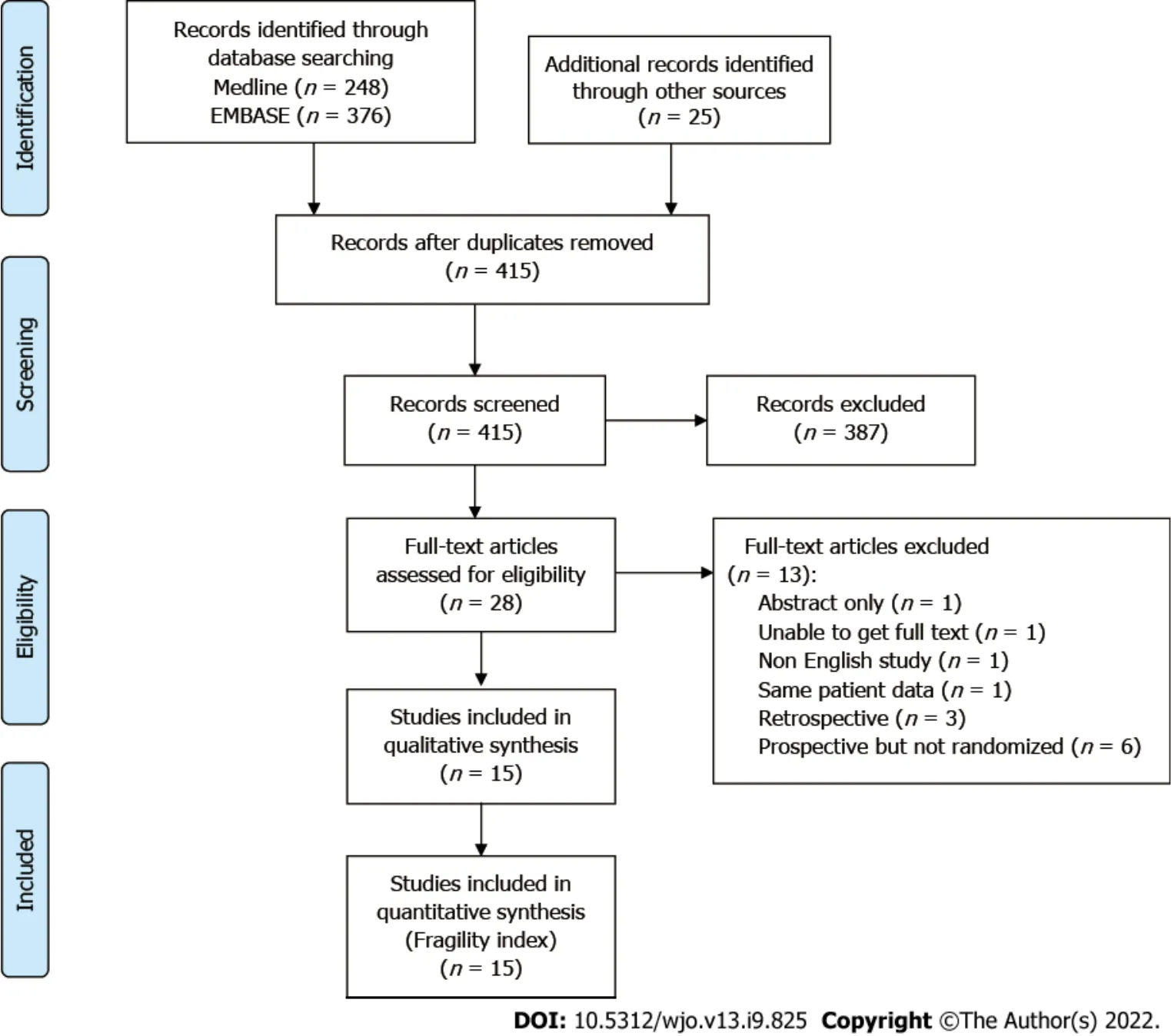
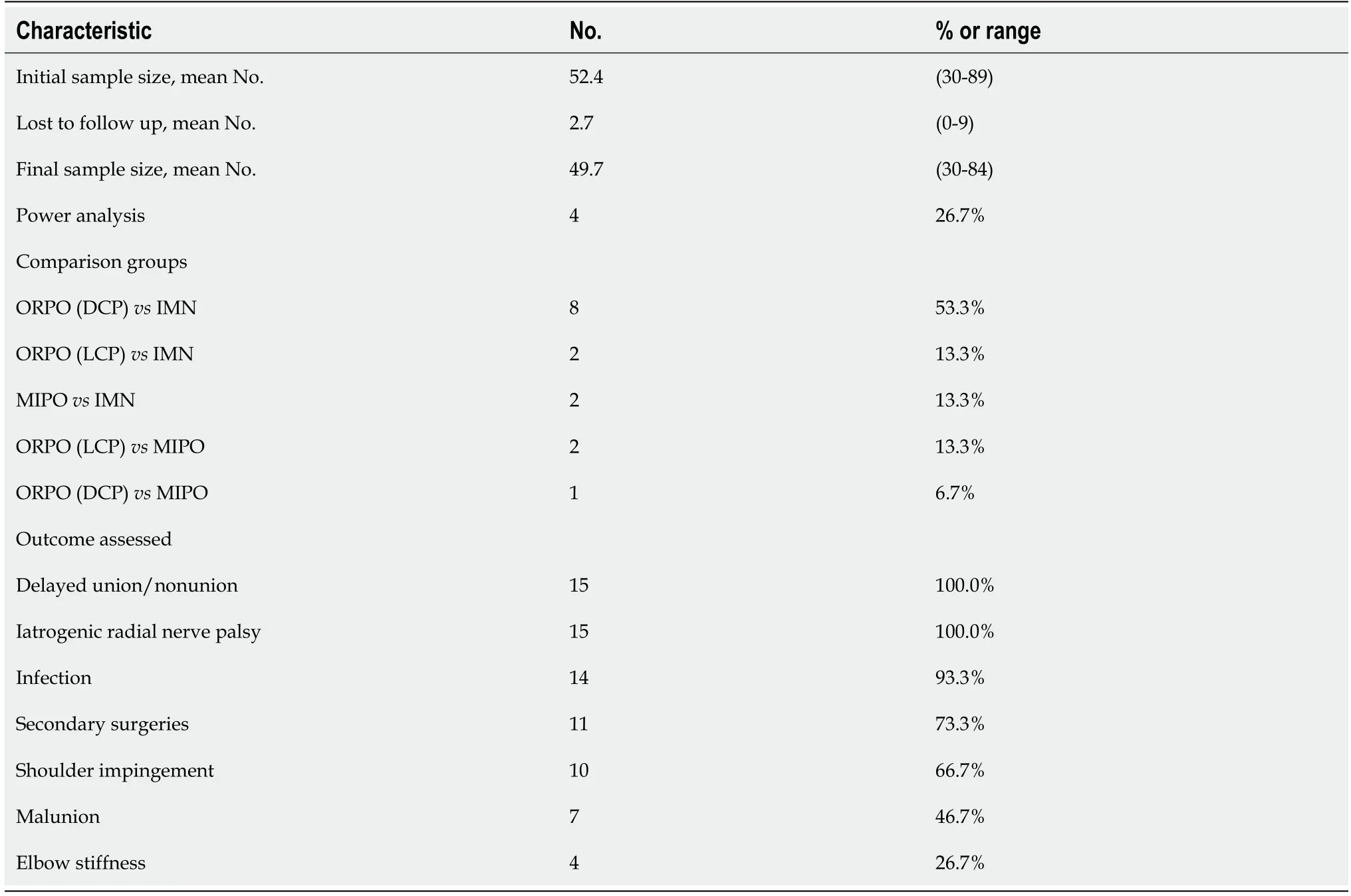
Our review of RCTs from recent review articles as well as systemic search strategy produced 415 records screened and 28 full text articles assessed (Figure 1). Of these,15 studies met inclusion criteria (Table 1)[43-57]. The primary outcome was only defined in two studies,shoulder function defined by University of California,Los Angeles (UCLA) scoring system in one study[43] and shoulder function defined by the American Shoulder and Elbow Surgeons (ASES) score in the other[56]. Table 2 contains summary characteristics for these trials. The mean initial sample size was 52.4 (range 30-89),mean lost to follow up of 2.7 (range 0-9),while the mean final sample size was 49.7 (range 30-84). The mean Jadad scale score was 2.5 (range 1-3). Power analysis was only reported in 4 studies (26.7%).

The most common comparison was between ORPO with DCP and IMN,found in 8 studies (53.3%). ORPO with LCPIMN,MIPOIMN,and ORPO with DCPIMN were the comparison groups of 2 studies each (13.3% each),and 1 study (6.7%) compared ORPO with DCP and MIPO. All 15 studies evaluated both the outcomes of delayed union/nonunion and iatrogenic radial nerve palsy. The majority of studies also reported incidence for infection (14 studies,93.3%),secondary surgeries (11 studies,73.3%),and shoulder impingement (10 studies,66.7%). Malunion was a reported outcome in 7 studies (46.7%),while only 4 studies (26.7%) reported the outcome of elbow stiffness.
The systematic review was completed,and results reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines statement[41]. We began by evaluating all review articles about humeral shaft fractures published from 2000 to 2019[6,8-12] and extracting from those studies all included RCTs for analysis. We then performed a systematic review of the literature to identify randomized controlled trials dealing with surgical treatment of humeral shaft fractures that had been published since the most recent review articles. The Medline and EMBASE databases were searched for the dates of January 1,2016 to April 1,2019 using the following Medical Subject Headings terms:“humeral fractures”. The Reference Citation Analysis (RCA) was also used to ensure high quality studies were included in the analysis. These dates were selected to identify new RCTs that would not have been included in prior systematic review articles. Titles and abstracts were screened,and full text manuscripts reviewed. Inclusion criteria included the following:patients randomized to 2 parallel arms,articles published in English,patient allocated to treatment and control arms in 1:1 ratio,reported statistical significance for dichotomous variables. Exclusion criteria included:published abstract only; studies without available full text,(non-English manuscripts; studies reporting patient data published previously; retrospective studies; and prospective studies that were not randomized.
The FI represents a valuable tool that can aid in the interpretation of results from RCTs. Along withvalue and confidence intervals,the FI provides a quantitative metric regarding the robustness of the reportedly significant results. In applying the FI to RCTs comparing surgical treatment options for humeral shaft fractures,this study has shown that there is a significant lack of robust data to recommend one treatment option over another on the basis of delayed union/nonunion,iatrogenic radial nerve palsy,infection,malunion,shoulder impingement,elbow stiffness,or secondary surgeries. The results published in the literature for treatment of humeral shaft fractures should be interpreted cautiously. This study,while limited in the analysis of functional outcome,suggests no clear benefit of one surgical technique over another with respect to dichotomous outcomes. Plate and nail techniques should both be considered as options for surgical treatment of humeral shaft fractures.



DlSCUSSlON
The difference between treatment options may possibly be captured only by continuous variables,and not by dichotomous variables. There is precedence for this in the orthopaedic literature,as Bhandari[58] recommended that when orthopaedic surgeons anticipate small sample sizes they can optimize their study’s statistical power by choosing a continuous outcome variable. In reviewing 76 orthopaedic RCTs,these authors found significantly greater study power in RCTs reporting continuous variables compared with studies reporting dichotomous variables (= 0.042),despite similar mean sample size in each group (> 0.05). The difference in treatment options for humeral shaft fractures,however,has been reported and analyzed by continuous variables previously. As summarized in this review in Table 4,the majority of included RCTs reported on continuous variable outcomes. The FI is not designed to evaluate continuous variables,and therefore all these continuous outcomes fell outside the scope of our review. As such,application of the FI does not add to the commentary favoring any one treatment over the others on the basis of these continuous variables.
In analyzing all outcomes individually for humeral shaft fractures,the median FI was 0,and remained so when calculating median FI for all outcomes combined. This result is not surprising given the median FI ≤ 3 reported in the orthopaedic literature previously[36-40]. A recent study used FI to explore the literature on the treatment of clavicular fractures and found the median FI to be 2,with 46.7% of trials reporting the number of patients lost to follow-up exceeded the FI[40]. Sample sizes in an operative population are inherently lower. In addition,the cost,time,and resources required to complete RCTs with sufficiently large sample sizes often pose a significant challenge in orthopaedics,where the incidence of desired exposures and events can be low[18,58]. Simply increasing sample size alone,however,is not sufficient to guarantee increased FI values,as even very large sample size studies can still have fragile results if the between-group difference is very small[14].
Identify the fragility index,which identifies the number of patients have a change in outcome from a significant to non-significant. This is important as higher level studies guide management in orthopedics.
Our systemic review looked at randomized control trials (RCTs) of the surgical treatment of humeral shaft fractures and discovered that the median FI for all outcomes was 0. In the studies with data leading to FI > 0,the FI exceeded the number lost to follow up in only two instances (2%):(1) Lower incidence of iatrogenic radial nerve palsy with IMN compared with ORPO[45]; and (2) Lower rate of overall total complication with ORPO compared with IMN[56]. Therefore,all evaluated outcomes (nonunion,radial nerve palsy,infections,malunion,malrotation,shoulder impingement,elbow stiffness,secondary surgeries,and overall complications) were extremely fragile and did not demonstrate superiority of one intervention (ORPO,MIPO,IMN) over another.

Our study has potential weaknesses,with some inherent to the requirements of the FI. In order to calculate an FI,a study must compare 2 treatment arms,randomize patients to those arms in 1:1 ratio,and report dichotomous outcomes. These inclusion criteria limit both the number of studies that can be included for analysis,as well as the number of outcomes or results that can be analyzed from the included studies. Another requirement of the FI is that a study must be a prospective,randomized trial. Due to this requirement,we excluded 3 retrospective studies and another 9 prospective studies that were not randomized. While this represents a loss in the number of included studies,and associated decrease in number of included patient outcomes,we do not feel this represents a significant loss as it means that the included studies represent the highest level of data availability.
Another potential weakness relates to the FI itself,which is not without inherent weakness or controversy. RCTs with small samples and in which the event of interest is rare,are common in orthopaedics and tend to be inherently fragile. The FI revolves around the statistical threshold of using< 0.05 as a strict criterion of correct inference. While this cutoff is necessary for making statistical determinations,the actual judging of the quality of inference is a complex activity with more nuance than is afforded in having avalue slightly greater of less than 0.05[59]. The misinterpretation of statistical tests extends beyond just the FI[60].
Here, indeed, it would be better to be a man than such a poor dumb fish as I am now, said he to himself; if I could only remember the words that the troll says when he changes my shape, then perhaps I could help myself to become a man again
CONCLUSlON
The relationship between enrolled initial sample size and FI for all complications (Figure 3) was calculated using the Spearman correlation coefficient and was found to not be significant with avalue of 0.830. The majority of included RCTs reported continuous variable outcomes such as operative time,radiation exposure time,operative blood loss,length of hospital stay,time to union,and functional outcome scores such as the UCLA scoring system,Mayo elbow performance index,and the ASES score. The outcomes with reported differences between groups are summarized in Table 4.
ARTlCLE HlGHLlGHTS
Research background
Humeral shaft fractures are a common injury which could be managed non-operatively or operatively.There is a lack of clear evidence to support open reduction internal fixation vs intramedullary nail fixation.
He looked annoyed. I rambled5 on about how I liked working “rehab” unit because I got to watch people reach their maximum potential. It was a place of possibilities. He said nothing.
Research motivation
While the FI was found to be > 0 in 9 outcomes total,the fact that the number lost to follow up exceeded the FI in 89/91 (98%) instances further confirms that those outcomes are quite fragile,and the significance of those conclusions should be called into question. When the number lost to follow up exceeds the FI this indicates that inclusion of the patients lost to follow up alone could have resulted in a nonsignificantvalue. Kesemenli[45] reported significantly higher rate of iatrogenic radial nerve palsy among the DCP group compared with the IMN group. Of note,this study reported no patients lost to follow up. While this suggests a robust outcome,the fact remains that the other 14/15 studies showed no difference among treatment groups regarding iatrogenic radial nerve palsy. Regarding all complications combined,two studies[55,56] resulted in FI > 0,but the FI exceeded the number lost to follow up in only one[56].
Research objectives
Applying the fragility index to humeral shaft fractures will aid in clinical decision making on treatment of humeral shaft fractures.
Colorful plastic sleds were shoved in the back of the Bronco and stashed9 in the little available trunk space of warm cars idling in the sub-zero Christmas chill. The moon was out and the trees were covered with frost, glittering like a snow globe in a happy child s hand.
Research methods
A systematic review of randomized controlled trials (RCTs) evaluating the surgical treatment of humeral shaft fractures was conducted. The fragility index (FI) was calculated for total complications,each complication individually,and secondary surgeries using the Fisher exact test,as previously published.
Research results
Fifteen RCTs were included in the analysis comparing open reduction plate osteosynthesis with dynamic compression plate or locking compression plate,intramedullary nail,and minimally invasive plate osteosynthesis. The median FI was 0 for all parameters analyzed. Regarding individual outcomes,the FI was 0 for 81/91 (89%) of outcomes. The FI exceeded the number lost to follow up in only 2/91(2%) outcomes.
Research conclusions
The FI shows that data from RCTs regarding operative treatment of humeral shaft fractures are fragile and does not demonstrate superiority of any particular surgical technique.
Research perspectives
Further research is needed to delineate whether open reduction internal fixation or intramedullary nail fixation is superior in the management of humeral shaft fractures.
But unfortunately, in spite of all her care, he grew so vain and frivolous10 that he quitted his peaceful country life in disgust, and rushed eagerly after all the foolish gaieties of the neighbouring town, where his handsome face and charming manners speedily made him popular
Morris SC is responsible for the data collection; Morris SC and Gowd AK analyze the data; Phipatanakul WP,Liu JN and Amin NH are responsible for the study conception; all authors participate in the manuscript preparation.
All authors report no relevant conflict of interest for this article.
The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
United States
Stephen Craig Morris 0000-0001-9462-7821; Anirudh K Gowd 0000-0001-7151-6459; Avinesh Agarwalla 0000-0001-5056-6780; Wesley P Phipatanakul 0000-0002-5110-1931; Nirav H Amin 0000-0002-1862-4669; Joseph N Liu 0000-0002-3801-8885.
Wu YXJ
A
Wu YXJ
 World Journal of Orthopedics2022年9期
World Journal of Orthopedics2022年9期
- World Journal of Orthopedics的其它文章
- Consensus Delphi study on guidelines for the assessment of anterior cruciate ligament injuries in children
- Histological difference in ligament flavum between degenerative lumbar canal stenosis and non-stenotic group:A prospective,comparative study
- Short arm cast is as effective as long arm cast in maintaining distal radius fracture reduction:Results of the SLA-VER noninferiority trial
- Revision anterior cruciate ligament reconstruction:Return to sports at a minimum 5-year follow-up
- Return to work following shoulder arthroplasty:A systematic review
- Evolution of evidence in spinal surgery – past,present and future Scientometric analysis of randomized controlled trials in spinal surgery