
Drug-induced autoimmune hepatitis: A minireview
2022-07-08 03:06ChinKimgTanDanielleHoLaiMunWangRahulKumar
World Journal of Gastroenterology 2022年24期
Chin Kimg Tan, Danielle Ho,Lai Mun Wang, Rahul Kumar
Abstract Drug-induced autoimmune hepatitis (DIAIH) is a specific phenotype of druginduced liver injury that may lead to the devastating outcome of acute liver failure requiring liver transplantation. Drugs implicated in DIAIH include antimicrobials such as nitrofurantoin and minocycline, non-steroidal anti-inflammatory drugs, statins as well as anti-tumor necrosis agents. The clinical features of druginduced liver injury are indistinguishable from idiopathic autoimmune hepatitis(AIH) as both may have positive AIH-related autoantibodies, elevated immunoglobulin G, as well as similar histopathological findings. In patients who show no clinical improvement, or there is progressive liver injury despite cessation of the suspected drug, a liver biopsy should be considered, whereby the presence of advance fibrosis on histology favors the diagnosis of idiopathic AIH. Empirical treatment with corticosteroids may be required in patients with non-resolving liver injury. A typical clinical scenario supportive of DIAIH includes a history of drug exposure with spontaneous resolution of liver injury after drug withdrawal and the absence of relapse after rapid steroid taper. In this article we report two cases of DIAIH secondary to Sorafenib and Atorvastatin along with a review of currently available literature. Early identification and treatment often lead to a favorable outcome in DIAIH.
Key Words: Drug-induced liver injury; Drug-induced autoimmune hepatitis; Autoimmune hepatitis; Review
INTRODUCTION
Idiosyncratic drug-induced liver injury (DILI) is rare and affects 14-19 per 100000 persons yearly[1,2].Despite its relatively low incidence, it is a leading cause of acute liver failure in the United States[3],Europe[4,5], and Japan[6]. In patients with DILI, liver-related death and liver transplantation occur in 3.6%-10% of cases[7].
Drug-induced autoimmune hepatitis (DIAIH) is a specific phenotype of idiosyncratic DILI with features indistinguishable from idiopathic autoimmune hepatitis (AIH), as it shares serological markers and/or histological features with idiopathic AIH[8]. Various terms have been used synonymously with DIAIH, including immune-mediated DILI[9] and drug-induced AIH-like injury[10].
Due to its rare occurrence, it is difficult to estimate the frequency of DIAIH. In addition, studies use varying definitions of DIAIH and drug causality assessments, as well as having diverse patient populations with different follow-up periods (Tables 1 and 2). It is estimated that DIAIH accounts for 2%-18% of AIH cases[10-14], and 2.9%-8.8% of all DILI are due to DIAIH[15,16]. The increasing incidence of AIH has been in part attributed to prevalent use of anti-tumor necrosis factor agents[14].
DRUGS ASSOCIATED WITH DIAIH
Multiple drugs that have been associated with DIAIH are classified into those with definite association (e.g., Minocycline, Nitrofurantoin, Infliximab), probable association (e.g., Diclofenac, Atorvastatin,Rosuvastatin, Etanercept), and possible association, depending on the cases reported and associations as summarized in the most recent American Association Society of Liver Disease AIH Practice Guidance[10].
DIAIH is classically associated with minocycline, nitrofurantoin, methyldopa, dihydralazine, and tienilic acid[17]. DILI with autoimmune phenotype defined as DILI with presence of AIH antibodies(antibodies to nuclear antigen, smooth muscle, and soluble liver antigen) occur in 83%, 74%, 60%, and 43% of nitrofurantoin, minocycline, methyldopa, and hydralazine related DILI cases, respectively[15].Immuno-allergic phenotype characterized by any combination of rash, fever, facial edema, lymphadenopathy, and eosinophilia is common in DILI associated with these four drugs as well, ranging from 11%-27%[15]. Another important cause of DIAIH include statins, where DIAIH or DILI with immune features occurs in about 8.5%-27.2% of all statin related DILI[18,19].
In recent years, there has been a change in the predominant culprit drugs causing DIAIH to antitumor necrosis factor[14], statins, and non-steroidal anti-inflammatory drugs[16,20,21] with notable contribution from complementary alternative medicines in studies from Asia[22].
PATHOGENESIS OF DIAIH
Reactive metabolites generated from hepatic metabolism of drugs bind to cellular proteins such as components of CYP450, which is then recognized as neoantigens by heightened immunological response leading to AIH[11,23,24] as a result of misdirected immune response against self[25].
In this minireview, we highlight two recent cases of DIAIH induced by Sorafenib and Atorvastatin seen at our center. We also aim to review the current literature on DIAIH and discuss distinguishing features between DIAIH and AIH.

Table 1 Studies comparing drug-induced autoimmune hepatitis and drug-induced liver injury
CASE DISCUSSION
Patient A
A 61-year-old man and teetotaler presented with a 1-week history of jaundice and malaise. He was on Atorvastatin 40 mg daily for 4 years for hyperlipidemia. He had a normal liver function test (LFT) prior to admission. He was started on Sorafenib 6 wk prior to presentation with jaundice for recurrent sarcoma of the left thigh. Clinical examination was unremarkable apart from scleral icterus. The LFT showed severe hepatocellular (HC) injury [bilirubin 4.56 mg/dL, alkaline phosphatase (ALP) 190 U/L,alanine transaminase (ALT) 1004 U/L, aspartate transaminase (AST) 790 U/L, international normalized ratio (INR) of 1.53]. Viral hepatitis screen, AIH-specific antibodies, and abdominal imaging were unremarkable. Of note, serum immunoglobulin G (IgG) was elevated (18.6 g/L). The liver biopsy showed features supportive of DILI and AIH (Figure 1). The Simplified AIH score was 6. The Roussel Uclaf Causality Assessment Model (RUCAM) score was 9 for Sorafenib and 6 for Atorvastatin.Diagnosis of Sorafenib-induced AIH was made. His LFT improved spontaneously with normalization of LFT 8 wk after stopping Sorafenib (Figure 2A).
Patient B
A 65-year-old man who was on Atorvastatin 40 mg daily presented with an incidental finding of acute HC pattern of liver injury 18 mo after initiation of Atorvastatin (albumin 39 g/L, globulin 39 g/L,bilirubin 0.64 mg/dL, ALP 107 IU/L, ALT 696 U/L, AST 381 U/L). Viral hepatitis screening, AIHspecific antibodies, and abdominal imaging were unremarkable. His serum IgG was normal (14.28 g/L).Atorvastatin was stopped, and an improvement in LFT was noted within the 1 wk (albumin ALT 474 U/L, AST 195 U/L). The RUCAM score for Atorvastatin was 4. As such, he was given the diagnosis of possible Atorvastatin-induced DILI. However, despite this initial improvement in his LFT, there was subsequent deterioration 2 wk after stopping Atorvastatin (albumin 34 g/L, globulin 43 g/L, ALP 137U/L, ALT 1404 U/L, AST 676 U/L, INR 1.09). A liver biopsy was performed 3 wk after stopping Atorvastatin in view of worsening acute liver injury. This showed marked HC injury with histological features suggestive of AIH (Figure 3). Following the liver biopsy, there was again spontaneous improvement (ALT 699 U/L), but this did not persist. Two months after cessation of Atorvastatin, he had severe HC injury with jaundice (bilirubin 11.87 mg/dL, ALP 96 U/L, ALT 1095 U/L, AST 938 U/L,INR 1.33) and elevated IgG (28.35 g/L). Liver biopsy was repeated, and this again demonstrated features of AIH. He was then started on prednisolone with rapid improvement of LFT (Figure 2Β). The final diagnosis was Atorvastatin-induced AIH.
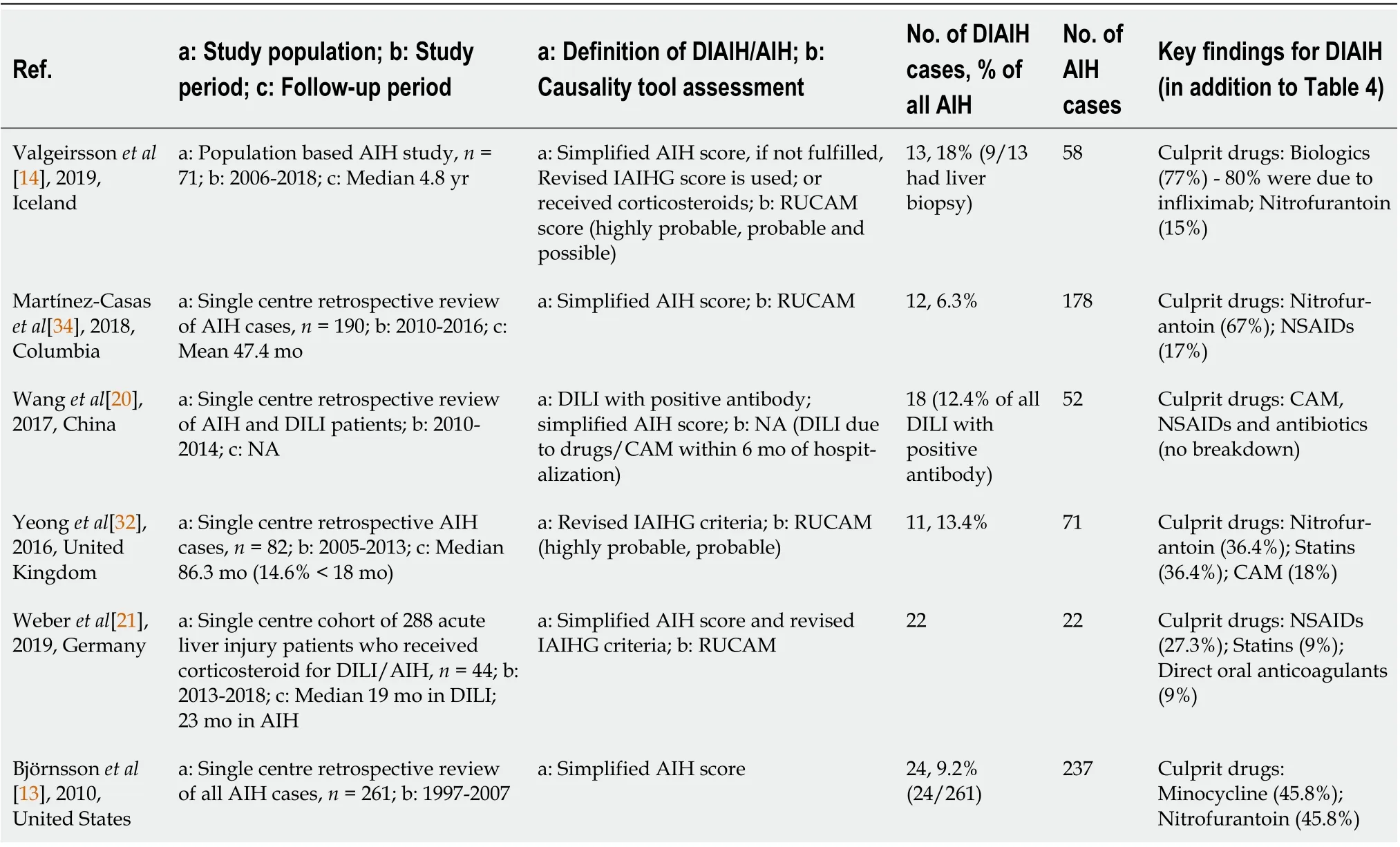
Table 2 Studies comparing drug-induced autoimmune hepatitis and autoimmune hepatitis
WHEN TO SUSPECT DIAIH IN PATIENTS WHO PRESENTS WITH DILI
The cases described above highlight two possible presentations of DIAIH. The first patient (patient A)had DILI and histological features compatible with AIH on liver biopsy. Although Sorafenib has not been reported to be associated with DIAIH, the temporal sequence of this case presentation and subsequent spontaneous resolution after cessation of Sorafenib is in keeping with DIAIH.
DIAIH shares many similar characteristics with DILI without features of AIH. More than half of DIAIH present with acute liver injury associated with jaundice in 70%-75% of cases[16], which is similar to DILI. On top of that, rash may be present in 4.5% of DIAIH and 7.9% of DILI[26].
The following pointers are useful in identification of DIAIH in patients who present with DILI. The main differences between these two conditions are also summarized in Table 3: (1) DIAIH and AIH should always be considered as differentials in a patient with a hepatocellular pattern of DILI. DIAIH is rarely associated with a cholestatic/mixed picture, and it is only seen in 8% of cases[16]; (2) A detailed medication history with a focus on recent drug exposures including complementary alternative medicines is essential[10]; (3) The latency period of drug exposure in DIAIH is usually prolonged compared to other types of DILI, some with a latency period exceeding 1 year,e.g., nitrofurantoin and minocycline[15]; (4) Seropositivity for AIH antibodies,e.g., antinuclear antibody (ANA), anti-smooth muscle antibody, anti-liver kidney antibody, and elevated serum IgG suggest possible DIAIH.However, not all patients with DIAIH have detectable autoantibodies or elevated IgG. Similarly, a proportion of patients with DILI may have detectable AIH antibodies[15,16]; (5) In the presence of detectable AIH antibodies and elevated IgG, AIH scoring (either pre-treatment score for Revised International AIH Group criteria[27] or simplified AIH score[28]) is useful to assess for possible orprobable AIH; (6) Liver-specific causality assessment tools may be used to ascertain the strength of association between drug exposure and clinical manifestation,e.g., RUCAM[29]; and (7) Liver biopsy is the cornerstone for the diagnosis of DIAIH and should be considered in the following scenarios: (a) Non resolving or worsening liver injury despite stopping possible culprit drugs; (b) Seropositivity of AIH antibodies, raised IgG, or possible AIH based on AIH scoring systems.
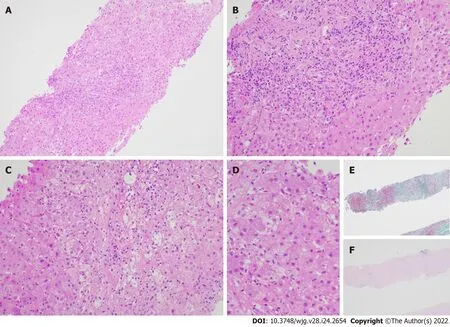
Figure 1 Liver biopsy specimen for patient A. A: Low power view [hematoxylin & eosin (H&E) 100 ×] displays conspicuous portal and lobular inflammation with lobular disarray. Mild steatosis is also noted; B: Higher magnification of the portal tract (H&E 200 ×), zone 1, shows moderate chronic inflammation,lymphoplasmacytic predominantly, and rare eosinophils, with interface damage; C: At similar magnification (H&E 200 ×), the lobule including the perivenular region,e.g., zones 2 and 3, exhibits lobulitis characterized by aggregates of plasma cells, swollen hepatocytes with rosetting, Councilman bodies, and hepatocyte drop-out;D: High power view (H&E 400 ×) demonstrates rosetting of hepatocytes with droplets of orange-brown bile pigment; E and F: Histochemical stains Masson trichrome(E, 40 ×) showing collapse with mild early young fibrosis and Victoria blue (F, 40 ×) revealing paucity of elastic fibers, thus in keeping with subacute injury. Overall,the appearances are supportive of subacute drug-induced liver injury in association with autoimmune hepatitis histological pattern.
Known culprit drugs of DIAIH such as nitrofurantoin may be overlooked as these agents are associated with longer latency period and have a lower ALT at presentation. A higher fibrosis stage or cirrhosis may be observed as a higher proportion of these patients are unknowingly continued on Nitrofurantoin prior to the diagnosis[30]. This underscores the importance of understanding the common culprits of DIAIH, where a significant proportion of DILI presents with DIAIH[15]. LiverTox®is an up-to-date online resource that provides information on hepatotoxicity caused by medications and supplements[31].
With the increasing use of targeted tumor therapies such as kinase inhibitor and immunotherapy,there are some case reports of DIAIH associated with these medications. To our knowledge, this is the first case report of Sorafenib-induced AIH. Imatinib, another type of kinase inhibitor, has also been reported to be associated with DIAIH[14,32].
Several studies have attempted to compare the differences between DIAIH and DILI (Table 1)[15,16,22], with key features of DIAIH including significantly longer duration of drug exposure and latency;higher ALT and AST; higher proportion of patients with positive ANA and SMA, and higher level of serum IgG, as summarized in Table 3.
Liver biopsy is key in differentiating DIAIH from DILI without features of AIH[10,33]. In patients with DIAIH, the histopathological features are similar to that of idiopathic AIH with significantly higher proportion of patients showing severe portal inflammation, prominent portal-plasma cells, rosettes, and severe focal necrosis as compared to other types of DILI[16].

Figure 2 Bilirubin and alanine transaminase trend for patients A and B. A: Patient A; B: Patient B.
Though there is no significant difference in the severity and outcomes of DIAIH compared to other types of DILI, it is crucial to identify DIAIH in patients who present with DILI, as DIAIH may require treatment with immunosuppressants if liver injury does not improve with cessation of possible culprit drugs[10,31,33]. A significantly higher proportion of patients (50% to 80%) with DIAIH are treated with corticosteroids/immunosuppressants as compared to non-DIAIH DILI, and DIAIH will need longer term follow up even when LFT normalizes as late relapses may occur in up to 50% of cases where immunosuppressants are stopped[22]. Majority of relapses occur within a year, but some may present late up to 3 years after the initial diagnosis, and risk factors for late disease recurrence are not clear.

Figure 3 Liver biopsy findings for patient B. A: Low power view [hematoxylin & eosin (H&E) 100 ×] shows portal and lobular inflammation with lobular disarray and mild steatosis; B: Higher magnification of the portal tract (H&E 200 ×) demonstrates moderate plasma cell-rich chronic inflammation with continuous interface damage; C: Lobulitis with aggregates of plasma cells and rosetting of hepatocytes is present in the lobule (H&E 200 ×); D and E: Masson trichrome (D, 40 ×)and Victoria blue (E, 40 ×) display mild early young fibrosis and paucity of elastic fibers, respectively. The absence of old mature type fibrosis suggested not a chronic injury. The autoimmune hepatitis histological pattern observed was therefore interpreted to be drug related, atorvastatin-induced.
DIFFERENTIATING DIAIH AND IDIOPATHIC AIH
The second case highlights the difficulty in differentiating DIAIH from idiopathic AIH. Βoth conditions have overlapping clinical presentations with HC pattern of liver injury and may have detectable ANA,SMA, and raised IgG in some cases[10,11]. A number of studies compared the difference between DIAIH and AIH (Table 2), with the key differences summarized in Table 4. Some useful features to distinguish between these two entities:
Clinical presentation
Majority (60%-83%) of DIAIH present with an acute presentation, whereas it is seen in less than 20%-35% of cases with idiopathic AIH[10,34]. Most studies of the two conditions do not demonstrate a significant difference in LFT levels[14,21,30,34], but ALT[13,30,34], AST[14,34], and bilirubin[14,34] tend to be higher in patients with DIAIH. Only one study[20] showed a significantly higher level of bilirubin,AST, and ALT in patients with DIAIH. There was no significant difference in the proportion of patients with detectable ANA (77-94%)[20,21] and elevated IgG (36%-59%)[14], although one study showed AIH had higher level of serum IgG compared to DIAIH; it was not, however, statistically significant[14].Immuno-allergic presentation with skin rash, fever, lymphadenopathy, and eosinophilia favor DIAIH,as it may occur in up to 30% of DIAIH[10,11].
AIH scoring and causality assessment
In a cohort of 44 patients with DIAIH and AIH, the simplified AIH score was not useful in differentiating the two entities[21]. Of note, patients with AIH had significantly higher pre-treatment AIH score compared to patients with DIAIH. The sensitivity and the specificity for pre-treatment AIH score (using a cut off of ≥ 12 – probable AIH) was shown to be 59% and 82%, respectively. As for RUCAM, using a cut off of ≥ 6 (probable), the specificity reaches 91%, albeit with a low sensitivity at 32%. When these are used in combination, there is still a potential for misdiagnosis in up to 11% of patients.
Histopathology
Βoth DIAIH and AIH share similar histological findings (portal and periportal infiltrates of lymphocytes, lobular hepatitis, plasma cells, and eosinophils) with no clear differentiating features,except presence of advance fibrosis or cirrhosis favoring idiopathic AIH[11,34]. However, a significantly higher proportion of patients with AIH showed typical features of AIH (54%) as compared to DIAIH(18.2%)[20], specifically in terms of portal inflammation with interface hepatitis and plasma cell infiltrates. The same study also found that DIAIH tended to have more eosinophilic infiltrates, which was not noted in other studies[21].
Treatment and response to treatment
The cornerstone in the management of DIAIH is to stop the culprit drug. Spontaneous improvement of LFT may then occur, as was observed in patient A. The most consistent and significant differentiating feature between DIAIH and AIH in published case series thus far lies in the response to treatment(Table 4). In cases where liver injury does not resolve despite cessation of the culprit drug or where the degree of DILI is severe, corticosteroids are usually started as per the initial management of AIH. Most studies on DIAIH exclusively include patients who were treated with immunosuppressants[14,20,21,30]. Βoth DIAIH and AIH showed excellent response to corticosteroids, with remission rate exceeding 90% in most cases[21,30-34].
It should be borne in mind that there is discrepancy in literature regarding the mean time to achieve immunosuppression induced remission in DIAIH and AIH. While one study demonstrated similar 3 mo mean time to remission[21] in both conditions, another showed a significant difference, where DIAIH took a significantly shorter time than AIH to achieve remission[34] (2 movs16.8 mo). This may be attributed to the heterogeneity of the study population. Resolution of DIAIH usually occurs after 1 mo(rarely up to 3 mo) of immunosuppression. Unlike in AIH, DIAIH rarely requires long term immunosuppression and has very low relapse rates after cessation of immunosuppressants over a long follow-up of up to 4 years[10,11,13-15,20,21,34] (Table 2). In cases where DIAIH relapses, the time to relapse is significantly longer compared to AIH[30], which implies that patients with DIAIH will require a longer period of follow-up after resolution of liver injury as compared to the usual DILI. Interestingly,despite similar time to remission in the two groups, Weberet al[21] showed that an early rapid response to corticosteroid treatment differentiates DIAIH from AIH with good sensitivity and specificity at 77%,respectively. The early rapid response was defined by 9% drop of ALT per day in the first week of corticosteroid therapy.
The use of steroids appears to be a promising means of differentiating DIAIH or AIH in the early course of disease with better sensitivity than RUCAM and AIH score[21]. This also has the potential benefit of avoiding long term immunosuppressive therapy in DIAIH. Also, in 30%-35% of DIAIH cases that were initially seropositive for ANA and SMA, the antibodies became undetectable at 6 mo following the initial DILI, which was independent of treatment with corticosteroids[15].
Major hepatology society guidelines recommend a similar approach in terms of corticosteroids initiation in non-resolving DIAIH and AIH[10,11]. However, there is no consensus regarding treatment duration and methods to confirm remission before discontinuation of immunosuppressants. Thus, the decision and timing to stop treatment should be assessed on case-by-case basis[10]. In fact, one study has shown success in tapering off immunosuppression within 3-17 mo without evidence of relapse[20].
Risk alleles and monocyte-derived hepatocyte like cells
Risk alleles for idiopathic AIH such as HLA DRΒ1 DRΒ1*03:01 or DRΒ1*04:01 are uncommon in DIAIH and, if this is detected, may favor a diagnosis of AIH[10]. The MetaHeps®test, which uses monocytederived hepatocyte-like cells, has been used to differentiate DIAIH from AIH with high sensitivity and specificity[21]. However, this test is not readily available, thereby limiting its utility in clinical practice.The lymphocyte toxicity assay described by Neumanet al[35] can sometimes be helpful in differentiating drug hypersensitivity syndromes from idiopathic AIH as well.
Outcomes
The long-term outcome of DIAIH is excellent with a survival rate between 90%-100% without liver transplantation[10]. This is in contrast with idiopathic AIH, where there is a high risk of relapse upon treatment withdrawal and risk of progression to cirrhosis, resulting in the need for liver transplantation[10,11,34]. It is also noteworthy that DIAIH can lead to chronic DILI with abnormal LFT lasting more than 6 mo in 17%-22% of cases[15,36].
CONCLUSION
In summary, it is important to differentiate between DIAIH and AIH in patients who present with DILI,as the management and outcome differ. Early recognition of DIAIH is key as the mainstay of management is cessation of culprit drug and in some cases, initiation of corticosteroids with the aim to avoid long-term immunosuppression.
ACKNOWLEDGEMENTS
We acknowledge all our colleagues in the Department of Gastroenterology and Hepatology and Pathology at Changi General Hospital who help manage the 2 patients described in the manuscript. We would also like to thank the 2 patients described here who readily consented to be described in this manuscript.
FOOTNOTES
Author contributions:Kumar R and Tan CK conceptualized the study; Tan CK, Ho D, and Kumar R wrote the initial manuscript; Wand LM provided critical input and histo-pathological slides for the manuscript; all authors were involved in the critical revision.
Conflict-of-interest statement:All authors have no relevant conflict of interest to report.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC ΒYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Singapore
ORCID number:Chin Kimg Tan 0000-0002-3918-4340; Danielle Ho 0000-0003-0652-406x; Lai Mun Wang 0000-0001-7113-4215; Rahul Kumar 0000-0002-5092-4821.
S-Editor:Yan JP
L-Editor:Filipodia
P-Editor:Yan JP
 World Journal of Gastroenterology2022年24期
World Journal of Gastroenterology2022年24期
- World Journal of Gastroenterology的其它文章
- Patient-derived organoids for therapy personalization in inflammatory bowel diseases
- Rebuilding trust in proton pump inhibitor therapy
- Pancreatic involvement in celiac disease
- Downregulation of TNFR2 decreases survival gene expression, promotes apoptosis and affects the cell cycle of gastric cancer cells
- Novel multiplex stool-based assay for the detection of early-stage colon cancer in a Chinese population
- Utility of a deep learning model and a clinical model for predicting bleeding after endoscopic submucosal dissection in patients with early gastric cancer