
Sequential chemotherapy and icotinib as first-line treatment for advanced epidermal growth factor receptor-mutated non-small cell lung cancer
2022-06-27 08:30ShengJieSunJinDiHanWeiLiuZhiYongWuXiaoZhaoXiangYanShunChangJiaoJianFang
World Journal of Clinical Cases 2022年18期
lNTRODUCTlON
Sun SJ, Jiao SC, and Fang J carried out the studies, participated in collecting data, and drafted the manuscript; Han JD and Liu W performed the statistical analysis and participated in its design; Wu ZY, Zhao X,and Yan X participated in the acquisition, analysis, interpretation of data and drafted the manuscript; All authors have read and approved the final manuscript.
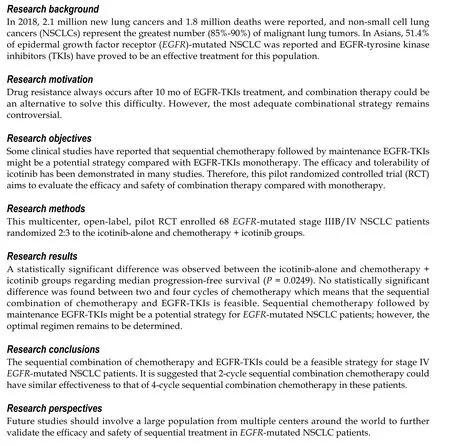
Despite the improvement in progression-free survival (PFS) by EGFR-TKIs, acquired resistance inevitably develops after about 10 mo of treatment[3,6]. Due to the complexity of the EGFR-TKI resistance mechanisms[6-8], a combined treatment approach could be used to prevent or delay resistance development[7]. One of the combination therapies of interest and most frequently explored is chemotherapy + TKI. In clinical trials, a combination of chemotherapy and EGFR-TKI (concomitant or intercalated) generally showed improved efficacy compared with EGFR-TKI alone as the first-line treatment for advanced NSCLC[9-13]. Nevertheless, the best combinational strategy remains controversial.
2.1 小鼠血清IL-33、TNF-α检测结果 模型组血清中IL-33水平与正常对照组比较明显降低(P<0.05)。模型组血清中TNF-α水平与正常对照组比较明显增高(P<0.01)。经益气固本胶囊治疗后,其血清中IL-33水平明显升高,低剂量组差异明显(P<0.05),高剂量组差异显著(P<0.01);其血清中TNF-α水平明显降低,低剂量组、高剂量组均与模型组比较,差异均有统计学意义(P<0.05)。见表1。
In preclinical studies, compared with concurrent administration of gefitinib alone, the sequential administration of pemetrexed or paclitaxel with gefitinib exerted stronger anti-tumor activity by enhancing cell cytotoxicity[14-18]. Sequential chemotherapy followed by maintenance EGFR-TKI therapy may be a potential strategy, as suggested by recent clinical trials[19-21]. Icotinib was suggested to have potential effects and tolerability when used sequentially with chemotherapy[22-24]. Therefore,the present pilot study aimed to evaluate the efficacy and safety of different sequential combinations of chemotherapy (varying cycle number and chemotherapeutic agents), followed by icotinib maintenance
icotinib alone as a first-line treatment for advanced
-mutated NSCLC. The results might help improve the treatment strategies for these patients.
MATERlALS AND METHODS
Study design and patients
This multicenter, open-label, pilot randomized controlled trial (RCT) was conducted in four centers in China between November 2012 and July 2015. The study was carried out according to the principles of the Declaration of Helsinki and the guidelines of the Good Clinical Practice of the International Council for Harmonization. The trial was approved by the ethics committees of General Hospital of People's Liberation Army. All patients signed an informed consent form before any study procedure.
The inclusion criteria were: (1) Age 18-72 years; (2) patients with treatment-naïve advanced lung cancer having
-sensitive mutation confirmed by pathological examinations; (3) stage IIIB or IV lung cancer; (4) Eastern Cooperative Oncology Group (ECOG) score of 0-2; (5) normal cardiac, liver, and renal functions, and routine blood test results; (6) expected survival > 3 mo; (7) negative urine pregnancy test within 7 d before screening for women of child-bearing age, and agreement to apply effective contraception measures to prevent pregnancy during and within 3 mo after the study for fertile men and women; and (8) signed informed consent forms. The exclusion criteria were: (1) Brain metastases; (2) active infection (according to the judgment of investigators); (3) major organ failure, such as decompensated cardiopulmonary failure; (4) newly developed myocardial infarction or cerebral infarction within 3 mo; (5) presence of a second malignant tumor (except for cured cervical cancer or skin cancer); (6) interstitial lung disease; or (7) pregnant or breastfeeding women.
在生产建设和百姓用电的过程中,结合实际需求和增长情况等,在电力系统发展中,需要明确电力电缆设备故障以及探测技术的问题,关系到电力传输的稳定性和安全性,在后续电缆故障分析的阶段,科学合理实施预设。此外先进的探测技术有重要的作用,在电缆故障判断的过程中,需要发挥良好的运行性能,保证电力系统的正常供电。
Trial registration: ClinicalTrials.gov, NCT01665417. Registered on August 12, 2012, https://clinicaltrials.gov/ct2/show/NCT01665417.
Randomization and blinding
This study involved three randomizations. The patients were first randomized 2:3 to icotinib-alone
chemotherapy + icotinib. The patients in the chemotherapy group were then randomized 1:1 to two
four cycles of chemotherapy and further randomized 1:1 to pemetrexed and cisplatin (PP)
docetaxel and cisplatin (DP) (Figure 1). All randomizations were carried out using a central randomization system designed by an independent biostatistician. The stratification factors after randomization included clinical stage (IIIB
IV), type of
mutation (exon 19 mutation
exon 21 mutation), ECOG score(0-1
2), and smoking status (non-smokers
mild smokers
regular smokers). This study was a pilot study, and the patients, treating physicians, and data assessors could not be blind to treatment allocation due to the nature of the treatments.
Treatment
Icotinib was provided by Betta Pharmaceutical Co., Ltd. (Zhejiang, China). Two or four cycles of PP(pemetrexed disodium 500 mg/m
iv d1, cisplatin 75 mg/m
iv d1, q3w) or DP (docetaxel 75 mg/m
iv d1, cisplatin 75 mg/m
iv d1, q3w) were administered to the patients assigned to the first-line chemotherapy + icotinib treatment. Icotinib hydrochloride (oral, 125 mg, tid) was used as maintenance therapy or second-line therapy until disease progression or the occurrence of severe toxicity for patients with clinical benefits or progressive disease after chemotherapy. Second-line chemotherapy after disease progression on icotinib was the crossover of the first-line chemotherapy. The chemotherapy regimen after DP/PP treatment had no restriction.
For the patients assigned to first-line icotinib treatment, 125 mg icotinib was administered orally three times per day until disease progression or the occurrence of severe toxicity. For second-line treatment,the patients received the PP (pemetrexed disodium 500 mg/m
iv d1, cisplatin 75 mg/m
iv d1, q3w) or DP (docetaxel 75 mg/m
iv d1, cisplatin 75 mg/m
iv d1, q3w) chemotherapy regimen, at the discretion of the treating physician.
The study's primary endpoint was PFS, defined as the date of the start of treatment to the date of PD(per RECIST 1.1) or death, whichever occurred first. The secondary endpoint was overall survival (OS),defined as the time from the start of treatment to death. Other efficacy endpoints included overall response rate (ORR) and disease control rate (DCR). The ORR was defined as the proportion of patients achieving CR or PR, and the DCR was defined as the proportion of patients achieving CR, PR, or SD.
Assessment
For patients on first-line chemotherapy, the tumor response was assessed after every two cycles of chemotherapy. During icotinib maintenance therapy, treatment efficacy assessment was performed 4 wk after treatment initiation and then every 6 wk until disease progression. For patients on first-line icotinib therapy, tumor response was assessed 4 wk after treatment initiation and then every 6 wk until disease progression. The tumors were assessed by plain and enhanced pulmonary computed tomography (CT) scanning, abdominal ultrasound examination, CT scanning or magnetic resonance imaging (MRI), ultrasound examination of superficial lymph nodes, brain MRI (if necessary), and emission CT (if necessary). The response to treatment was classified as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) according to RECIST 1.1[25]. The safety evaluation was performed using physical examinations and laboratory examinations (hematological and blood biochemical examinations). All adverse events were recorded from the informed consent until 30 d after the last dose of the study drug. The severity of the adverse events was assessed and documented according to the National Cancer Institute-Common Toxicity Criteria 3.0. The investigators judged the relationship between the adverse events and treatment.

Outcomes
在拉斐尔前派短暂的第一乌托邦消亡之后,罗塞蒂的艺术对后世的影响反而要远超从前。如果说此前更多的是以团队成员的性质进行艺术活动的话,那么这段时期的罗塞蒂已经完全呈现出自己的个人风格了。
Statistical analysis
All analyses were performed using SAS 9.2 (SAS Institute, Inc., NC, United States). The efficacy analysis was performed in the full analysis set, defined as all randomized patients who received at least one dose of the study drug. The safety set included all randomized patients who received at least one dose of the study drug. Continuous data are presented as means ± SD and medians (ranges). Categorical data are presented as numbers (percentages). PFS and OS were analyzed using the Kaplan-Meier method and the log-rank test. The ORR and DCR were summarized as percentages and Clopper-Pearson 95%CIs.Two-sided
values of < 0.05 were considered statistically significant.
RESULTS
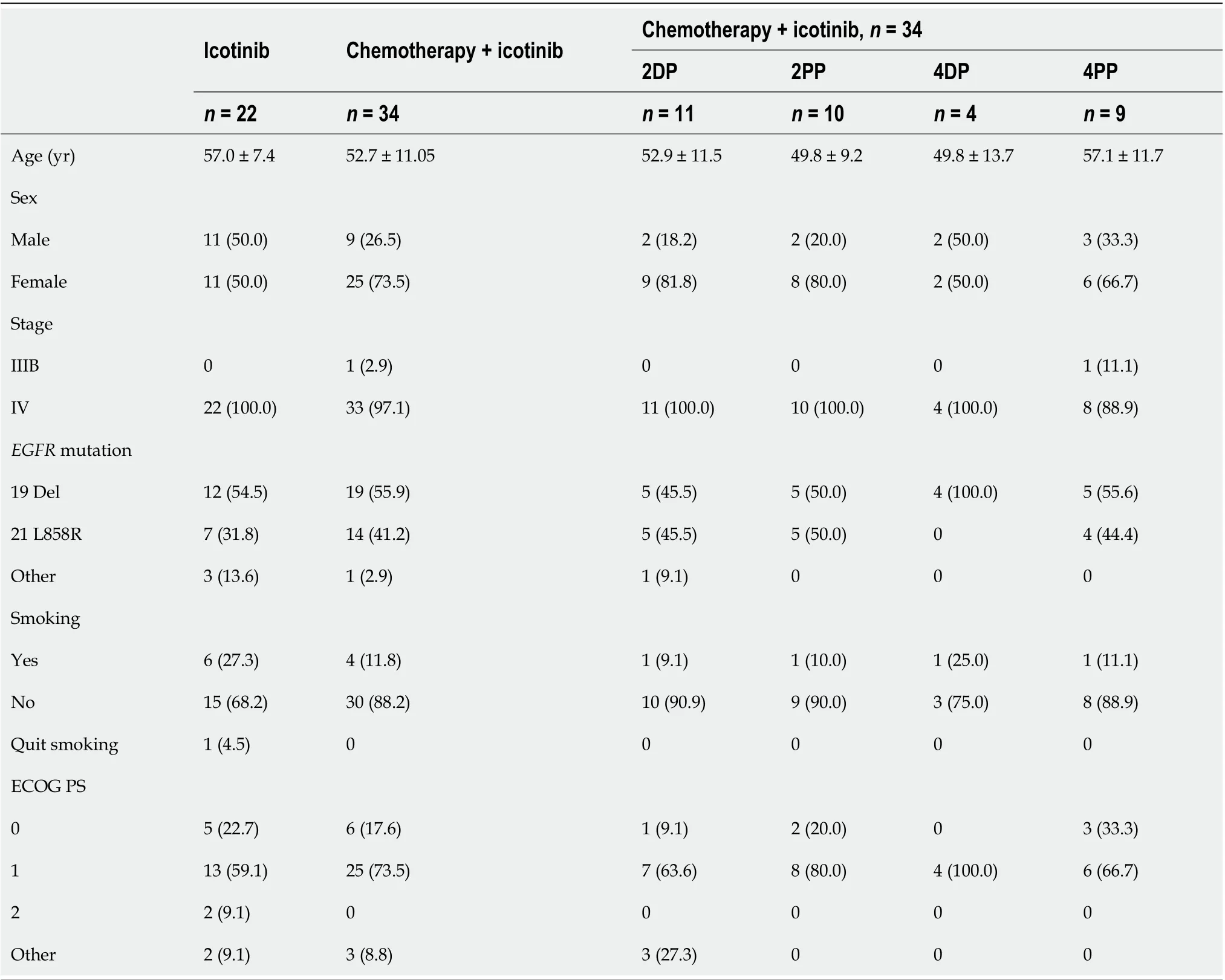
Characteristics of the participants
Between November 2012 and July 2015, 68 participants were recruited: 24 in the icotinib-alone group and 44 in the chemotherapy + icotinib group. The participants who received single-dose treatment (22 in the icotinib-alone group and 36 in the chemotherapy + icotinib group) were included in the analysis. All participants were randomized, and treatment was initiated. The characteristics of the participants are shown in Table 1. All patients except one had stage IV NSCLC.
A sequential combination of chemotherapy and EGFR-tyrosine kinase inhibitor is feasible for stage IV
-mutated NSCLC patients.
In the present study, four cycles of chemotherapy were not better in terms of ORR, DCR, PFS, and OS compared with two cycles. Two cycles might be enough to eliminate tumor cells sensitive to chemotherapy and activate the immune system, while four cycles might lead to adverse events and decreases in blood immune cells[43]. In addition, fewer cycles could help reduce the physical, psychological, and economic burden of chemotherapy[43]. The rate of grade ≥ 3 TRAEs was 14.3% in the twocycle subgroup and 15.4% in the four-cycle subgroup. Hence, the present study suggests similar efficacy and safety for the two- and four-cycle regimens, which could be supported by a meta-analysis that suggested no added benefit of six cycles of first-line chemotherapy compared with three and four cycles[43]. However, this study was not powered to compare two-
four-cycle regimens, and additional studies are necessary to examine this point.
Response to treatment
Table 2 shows the responses to treatment. No participants achieved CR. In the icotinib-alone group, the ORR was 54.5% (95%CI: 32.2-75.6) and the DCR was 90.9% (95%CI: 70.8-98.9) compared with 44.1%(95%CI: 27.2-62.1) and 97.1% (95%CI: 84.7-99.9), respectively, in the chemotherapy + icotinib group.
When considering the number of chemotherapy cycles, the ORR was 47.6% (95%CI: 25.7-70.2) and the DCR was 100.0% (95%CI: 83.9-100.0) for two cycles, and the ORR was 38.5% (95%CI: 13.9-68.4) and the DCR was 92.3% (95%CI: 64.0-99.8) for four cycles. When considering the chemotherapy types, the ORR was 40.0% (95%CI: 16.3-67.7) and the DCR was 100.0% (95%CI: 78.2-100.0) for DP, and the ORR was 47.4% (95%CI: 24.4-71.1) and the DCR was 94.7% (95%CI: 74.0-99.9) for PP. When considering each chemotherapy regimen, the ORR was 33.3%-60.0%, and the DCR was 88.9%-100%.
3)三伏贴治疗方案:①三伏贴选穴:主穴1:选取大椎、定喘(双侧)、肺俞(双侧);主穴2:膻中、天突。两组穴位交替敷贴。
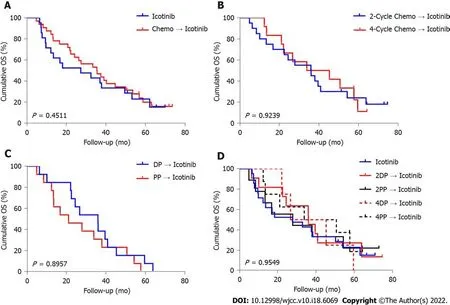
Survival
In the icotinib group, the median follow-up was 23.1 (range, 2.5-71.9) mo. The median follow-up in the chemotherapy + icotinib group was 36.0 (range, 5.1-75.7) mo. Figures 2 and 3 present the PFS and OS,respectively. The median PFS in the icotinib-alone and chemotherapy + icotinib groups was 8.0 mo(95%CI: 3.8-11.6)
13.4 mo (95%CI: 10.2-16.3), respectively (
= 0.0249). The median OS was 23.1(95%CI: 9.7-50.3)
36.0 mo (95%CI: 22.2-45.4), respectively (
= 0.4511). The median PFS of the participants who received two and four chemotherapy cycles was 12.1 mo
15.1 mo, and the median OS was 36.1 mo
33.9 mo, with no significant differences (PFS,
= 0.6605; OS,
= 0.9239). The PFS after two cycles of DP, two cycles of PP, four cycles of DP, and four cycles of PP was 11.9, 15.2, 15.2, and 15.1 mo, respectively; the median OS was 36.1, 28.0, 36.1, and 33.9 mo, respectively. No significant difference was observed among the different treatment regimens (PFS,
= 0.1815; OS,
= 0.9549).
Table 3 presents the treatment received after icotinib-based therapy. The treatment profile was similar in the two groups.
阿里很久没见到母亲了,阿里只知道母亲在睡觉。他不明白,母亲为什么老是睡觉。他想不明白,也问不出来。虽然每天早上他去东湖放录音,听母亲的声音,但那到底不是母亲。没有母亲温热的手掌,也没有母亲的笑声,更没有母亲每天跟他说这说那,给他好吃的东西。这个世界跟以前不一样了。母亲一直在睡觉,阿里竟也一直都不进她的房间。阿里不能吵她。
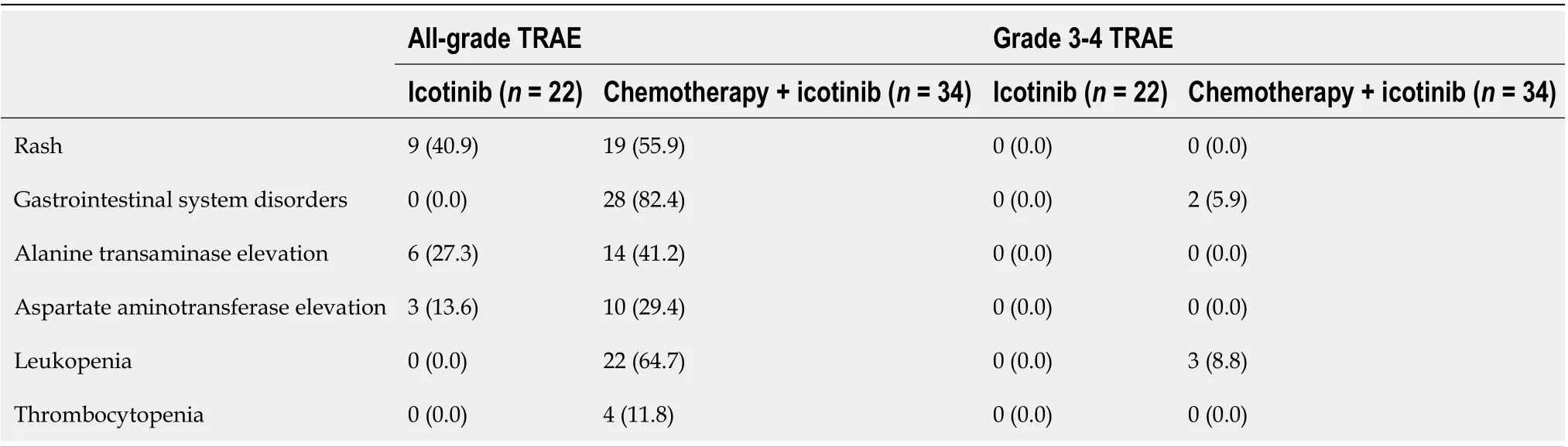
Treatment-related adverse events
The rates of all-grade treatment-related adverse events (TRAEs) were lower in the icotinib-alone group compared with the chemotherapy + icotinib group, and included rash (40.9%
55.9%), gastrointestinal system disorders (0.0%
82.4%), alanine transaminase elevation (27.3%
41.2%), aspartate aminotransferase elevation (13.6%
29.4%), leukopenia (0.0%
64.7%), and thrombocytopenia (0.0%
11.8%). Grade 3-4 TRAEs were not observed in the icotinib-alone group. However, grade 3-4 gastrointestinal system disorders (5.9%) and leukopenia (8.8%) were recorded in the chemotherapy +icotinib group (Table 4).
DlSCUSSlON
Sequential chemotherapy followed by maintenance TKI may be a potential strategy for advanced NSCLC with
mutation. However, the optimal regimen remains to be determined. In this study,icotinib was selected because of the potential effect and tolerability of sequential chemotherapy and icotinib[22-24]. The present study indicated that the sequential combination of chemotherapy followed by icotinib improved PFS by 5.4 mo compared with icotinib alone as the first-line therapy of NSCLC. In addition, no differences were observed between two and four cycles of chemotherapy and between PP and DP. Therefore, for patients with advanced NSCLC with
mutation, a sequential combination of chemotherapy and an EGFR-TKI is feasible. Considering the chemotherapy toxicity, the efficacy of a two-cycle chemotherapy regimen was comparable to that of a four-cycle chemotherapy regimen.
In the present study, no significant differences were observed in OS (36 mo
23.1 mo) and PFS (8.0 mo
13.4 mo), which was probably due to the small sample size or the fact of crossover of the treatment group upon disease progression. Considering the synergistic effect of EGFR-TKIs and chemotherapy in the elimination of tumor cells, as reported by some preclinical studies, gefitinib and erlotinib were combined with two chemotherapy regimens (cisplatin + gemcitabine; carboplatin +paclitaxel), thus launching four large phase III clinical studies, including INTACT 1 and 2 and TRIBUTE[26,27]. These studies showed no significant difference between chemotherapy and combined treatment groups (PFS and OS), which might be because the participants were not selected according to their
mutation status[28]. A retrospective analysis of the OPTIMAL study on
mutation (exon 19 deletion or exon 21 L858R mutation) showed that the OS of patients treated with chemotherapy alone was significantly lower than that of patients who received TKI and sequential chemotherapy [median OS: 11.2
29.7 mo, HR = 2.97 (1.74-5.07)]. Although it was a retrospective analysis, it also suggested that sequential treatment with TKI and chemotherapy for selected patients with
mutation could prolong patient OS[29]. However, a phase II clinical study in Japan, NEJ00, reported that in NSCLC patients with
mutation, the combined therapy of gefitinib, pemetrexed, and carboplatin was significantly superior to chemotherapy followed by targeted therapy[30]. Among the 80 enrolled patients, 41 received concurrent combination therapy, while 39 also had sequential therapy. The medianPFS was 18.3 mo
15.3 mo [HR = 0.71 (0.42-1.2),
= 0.02], and median OS was 41.9 mo
30.7 mo [HR= 0.51 (0.26-0.99),
= 0.042], respectively. The response rates in the two groups were similar (87.8% and 84.6%, respectively). Furthermore, phase II clinical studies conducted in China reported similar results for gefitinib combined with pemetrexed-based chemotherapy[31]. Based on the results of NEJ005, the phase III clinical study NEJ009 further confirmed that the efficacy of gefitinib combined with carboplatin and pemetrexed was superior to that of single-drug gefitinib treatment[32], which showed that the PFS was 20.9 mo (18.0-24.2)
11.2 mo (9.0-13.4) [HR = 0.43 (0.39-0.62),
< 0.001], and more importantly, OS was 52.2 mo
38.8 mo (HR = 0.69,
= 0.013). Subsequently, CTRI/2016/08/007149,conducted in India and almost completely similar to NEJ009, further confirmed that the efficacy of gefitinib combined with carboplatin and pemetrexed was significantly superior to that of gefitinib alone[33]. It also demonstrated that the PFS of gefitinib combined with pemetrexed-based chemotherapy was longer than 16 mo and longer than 20.9 mo in NEJ009, which was a much longer PFS than achieved by gefitinib alone. In particular, two phase III clinical trials, NEJ009 and CTRI/2016/08/007149, confirmed the benefits of OS in the combination treatment group. The studies mentioned above mainly focused on targeting, a synchronous combination of chemotherapy, or alternating sequential combination of targeting and chemotherapy. However, evidence on the use of sequential therapy based on chemotherapy followed by the target drug in
-mutant patients is lacking. Studies at the molecular level confirmed that sequential chemotherapy with the EGFR-TKI erlotinib after docetaxel could enhance the M-phase stagnation of tumor cell division and growth, resulting in cell apoptosis. They suggested a synergistic effect between molecular targeted therapy and appropriate sequential chemotherapy. These experimental results indicated that the use of chemotherapy first to induce tumor cell stagnation and apoptosis in the M phase, followed by EGFR-TKIs to enhance this effect[34], would result in sequential therapy having a superposition effect, which might be used as a feasible option.Similar to the present study, Han
[13] compared gefitinib + pemetrexed + carboplatin
gefitinib alone
pemetrexed + carboplatin and reported a higher ORR with the TKI + chemotherapycombination than for TKI alone or chemotherapy alone (82.5%
65.9%
32.5%), with similar trends in PFS and OS. Similar results were also reported by Wen
[35] and Yan
[36]. Another RCT focused on first-line chemotherapy and TKI sequential treatment in patients with advanced non-squamous NSCLC[37,38]. PFS and OS were similar in the pemetrexed + cisplatin + gefitinib and gefitinib monotherapy groups in the ITT population and
-mutated subgroup, but the sample size in the
-mutated subgroup was too small to draw a firm conclusion. The combination therapy may outperform the monotherapy ORR as chemotherapy and TKIs do not affect the cancer cells using the same mechanisms (
, hitting the cells in multiple ways), and intratumor heterogeneity may be present(
, using multiple drugs increases the likelihood of killing cells resistant to one of the drugs used). The immune system can also be activated[9,34,39,40]. Nevertheless, the PFS in the sequential treatment group in the present study was superior to that in the TKI-alone therapy group. The reason for the inconsistent results in these two studies might be that the number of patients with
mutation in either study was small, affecting the consistency of the study results. Of note, the recent results of the FLAURA trial showed that first-line osimertinib achieved better OS and PFS than the comparator EGFRTKIs[41], and sequential osimertinib with chemotherapy as a first-line option should be investigated.Due to the TRAE profile of osimertinib, the sequential use of chemotherapy and osimertinib could decrease the occurrence of TRAEs in the first-line treatment of NSCLC. Furthermore, the combination of EGFR-TKIs with vascular endothelial growth factor inhibitors could be a potential strategic option[42]and should also be examined.



从图8(a)、图8(b)可以看出,带内误差补偿前,成像场景中强目标距离向旁瓣很高,远端旁瓣数值也较高,会遮盖周围弱目标,成像效果很差。经过带内幅度和相位误差补偿后,旁瓣数值降低十分明显,远端旁瓣对周围目标的影响非常小,成像质量得到明显改善。综合以上处理结果可知,子带内幅度和相位误差得到了有效的补偿。
There are many therapeutic options in lung cancer, including chemotherapy, targeted therapy, and immunotherapy[2,44-48]. Icotinib is a promising targeted therapy for
-mutated NSCLC[18,22-24].The present study selected the combination of icotinib (or other EGFR-TKIs) and chemotherapy since it is the most studied combination in NSCLC, with apparent benefits in response and survival[9,18,24,34-36,49]. Still, the combination of EGFR-TKIs and immunotherapy could be a promising option for NSCLC[50-52], but some evidence suggests that immunotherapy is not effective in patients with
mutated NSCLC, probably because of the specific tumor microenvironment[52,53]. Indeed, early trials showed that immunotherapy monotherapy was inferior to EGFR-TKIs in
-mutated NSCLC[52,53]. Subsequent studies showed that the combination of immunotherapy with EGFR-TKIs in
mutated NSCLC resulted in high rates of serious AEs (33.3%-71.4% of grade 3-4 AEs)[54-56]. Therefore,additional studies are necessary before being able to use immunotherapy with EGFR-TKIs in patients with
-mutated NSCLC.
㊳ 插 图 出 自 L.D.Ettlinger,“The Pictorial Source of Ripa's'Historia'”,Journal of the Warburg and Courtauld Institutes,vol.13,no.3/4,1950,图版 63。
Roviello
[57] reported that EGFR-TKIs led to good outcomes in older adults with
-mutated NSCLC. We agree that EGFR-TKIs could be a valuable and less toxic treatment option for older adults who often have difficulties with chemotherapy. Unfortunately, in the present study, the sample size was too small to be able to examine the influence of age on the treatment outcomes. Furthermore, as per the inclusion criteria, no patients > 72 years old were enrolled. Nevertheless, examining treatment options specifically in older adults is indeed a future direction for research.
This study had some limitations. This study was an exploratory study with a small sample size, and the analysis of OS had limited power. In addition, it was restricted to Chinese patients. It was an investigator-initiated trial. Only icotinib was provided, and the patients had to pay for the chemotherapy. This could have influenced recruitment. Although the trial was open to stage IIIB-IV patients, only one stage IIIB participant was actually recruited, mostly limiting the conclusions to stage IV patients. Due to the limited generalizability, the efficacy of sequential chemotherapy followed by TKI in the Caucasian population requires further investigation. Whether the results could also be generalized to non-stage IV patients remains to be examined.
CONCLUSlON
For patients with stage IV NSCLC and
mutation, sequential chemotherapy followed by TKI maintenance therapy is feasible. No significant differences were found in terms of the influence of the different number of chemotherapy cycles or different chemotherapy drugs on the curative effect,suggesting that fewer chemotherapy cycles could result in the same therapeutic effect in these specific patients.
ARTlCLE HlGHLlGHTS
FOOTNOTES
Globally, lung cancer is the malignancy with the highest incidence and mortality. In 2018, 2.1 million new lung cancers and 1.8 million deaths were reported, with an annual age-standardized incidence rate of 22.5 per 100000 individuals and an age-standardized yearly mortality rate of 18.6 per 100000 individuals[1]. Non-small cell lung cancers (NSCLCs) represent the greatest number (85%-90%) of malignant lung tumors[2], and almost half of NSCLCs are adenocarcinomas. Adenocarcinomas display activating mutations in the epithelial growth factor receptor (
) gene, making such cancers candidates for EGFR tyrosine kinase inhibitor (EGFR-TKI) therapy[3-5]. In Asians, individuals harboring
mutations account for 51.4% of adenocarcinoma NSCLCs[3-5]. Currently, EGFR-TKIs are the guideline-recommended first-line treatment for advanced NSCLC with
mutations[5].
The study was reviewed and approved by General Hospital of People's Liberation Army.
深化水利建设与管理体制改革 为水利改革发展提供坚实保障……………………………………………………… 孙继昌(23.9)
ClinicalTrials.gov, NCT01665417. Registered on August 12, 2012,https://clinicaltrials.gov/ct2/show/NCT01665417.
All patients signed an informed consent form before any study procedure.
The authors declare no conflicts of interest.
The raw dataset analyzed in the current study are available from the corresponding author on reasonable request.
熵权法通过收集客观信息,以事实为基础进行计算,消除了信息之间的重叠性,有很强的说服力。但是未反映研究人员的经验,同时易受离散极值的影响,结果有时与实际情况不符,难以得到公认。
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Sheng-Jie Sun 0000-0001-7010-9472; Jin-Di Han 0000-0002-0790-9802; Wei Liu 0000-0002-1534-1823; Zhi-Yong Wu 0000-0002-8763-4449; Xiao Zhao 0000-0002-8661-1480; Xiang Yan 0000-0002-3683-474X; Shun-Chang Jiao 0000-0001-8017-5342; Jian Fang 0000-0003-3697-4563.
Zhang H
Webster JR
Zhang H
1 Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018 : GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018 ; 68 : 394 -424 [PMID: 30207593 DOI: 10 .3322 /caac.21492 ]
2 Novello S, Barlesi F, Califano R, Cufer T, Ekman S, Levra MG, Kerr K, Popat S, Reck M, Senan S, Simo GV,Vansteenkiste J, Peters S; ESMO Guidelines Committee. Metastatic non-small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up.
2016 ; 27 : v1 -v27 [PMID: 27664245 DOI:10 .1093 /annonc/mdw326 ]
3 Cabanero M, Sangha R, Sheffield BS, Sukhai M, Pakkal M, Kamel-Reid S, Karsan A, Ionescu D, Juergens RA, Butts C,Tsao MS. Management of
-mutated non-small-cell lung cancer: practical implications from a clinical and pathology perspective.
2017 ; 24 : 111 -119 [PMID: 28490925 DOI: 10 .3747 /co.24 .3524 ]
4 da Cunha Santos G, Shepherd FA, Tsao MS. EGFR mutations and lung cancer. Annu Rev Pathol 2011 ; 6 : 49 -69 [PMID:20887192 DOI: 10 .1146 /annurev-pathol-011110 -130206 ]
5 Singer J, Irmisch A, Ruscheweyh HJ, Singer F, Toussaint NC, Levesque MP, Stekhoven DJ, Beerenwinkel N.Bioinformatics for precision oncology.
2019 ; 20 : 778 -788 [PMID: 29272324 DOI: 10 .1093 /bib/bbx143 ]
6 Morgillo F, Della Corte CM, Fasano M, Ciardiello F. Mechanisms of resistance to EGFR-targeted drugs: lung cancer.
2016 ; 1 : e000060 [PMID: 27843613 DOI: 10 .1136 /esmoopen-2016 -000060 ]
7 Maione P, Sacco PC, Casaluce F, Sgambato A, Santabarbara G, Rossi A, Gridelli C. Overcoming Resistance to EGFR Inhibitors in NSCLC.
2016 ; 11 : 99 -105 [PMID: 27028971 DOI:10 .2174 /1574887111666160330120431 ]
8 Del Re M, Crucitta S, Gianfilippo G, Passaro A, Petrini I, Restante G, Michelucci A, Fogli S, de Marinis F, Porta C, Chella A, Danesi R. Understanding the Mechanisms of Resistance in
-Positive NSCLC: From Tissue to Liquid Biopsy to Guide Treatment Strategy.
2019 ; 20 [PMID: 31416192 DOI: 10 .3390 /ijms20163951 ]
9 Nan X, Xie C, Yu X, Liu J. EGFR TKI as first-line treatment for patients with advanced EGFR mutation-positive nonsmall-cell lung cancer.
2017 ; 8 : 75712 -75726 [PMID: 29088904 DOI: 10 .18632 /oncotarget.20095 ]
10 Decoster L, Giron P, Mignon S, De Grève J. The evolving first-line treatment of advanced non-small cell lung cancer harbouring epidermal growth factor receptor mutations.
2018 ; 7 : S134 -S137 [PMID: 29780706 DOI: 10 .21037 /tlcr.2018 .03 .08 ]
11 Sebastian M, Schmittel A, Reck M. First-line treatment of EGFR-mutated nonsmall cell lung cancer: critical review on study methodology.
2014 ; 23 : 92 -105 [PMID: 24591666 DOI: 10 .1183 /09059180 .00008413 ]
12 Zhang C, Leighl NB, Wu YL, Zhong WZ. Emerging therapies for non-small cell lung cancer. J Hematol Oncol 2019 ; 12 :45 [PMID: 31023335 DOI: 10 .1186 /s13045 -019 -0731 -8 ]
13 Han B, Jin B, Chu T, Niu Y, Dong Y, Xu J, Gu A, Zhong H, Wang H, Zhang X, Shi C, Zhang Y, Zhang W, Lou Y, Zhu L,Pei J. Combination of chemotherapy and gefitinib as first-line treatment for patients with advanced lung adenocarcinoma and sensitive EGFR mutations: A randomized controlled trial.
2017 ; 141 : 1249 -1256 [PMID: 28560853 DOI:10 .1002 /ijc.30806 ]
14 Wu M, Yuan Y, Pan YY, Zhang Y. Combined gefitinib and pemetrexed overcome the acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in non-small cell lung cancer.
2014 ; 10 : 931 -938 [PMID:24840891 DOI: 10 .3892 /mmr.2014 .2243 ]
15 Cheng H, An SJ, Dong S, Zhang YF, Zhang XC, Chen ZH, Jian-Su, Wu YL. Molecular mechanism of the scheduledependent synergistic interaction in EGFR-mutant non-small cell lung cancer cell lines treated with paclitaxel and gefitinib.
2011 ; 4 : 5 [PMID: 21255411 DOI: 10 .1186 /1756 -8722 -4 -5 ]
16 Li T, Ling YH, Goldman ID, Perez-Soler R. Schedule-dependent cytotoxic synergism of pemetrexed and erlotinib in human non-small cell lung cancer cells.
2007 ; 13 : 3413 -3422 [PMID: 17545550 DOI:10 .1158 /1078 -0432 .CCR-06 -2923 ]
17 Giovannetti E, Lemos C, Tekle C, Smid K, Nannizzi S, Rodriguez JA, Ricciardi S, Danesi R, Giaccone G, Peters GJ.Molecular mechanisms underlying the synergistic interaction of erlotinib, an epidermal growth factor receptor tyrosine kinase inhibitor, with the multitargeted antifolate pemetrexed in non-small-cell lung cancer cells.
2008 ; 73 :1290 -1300 [PMID: 18187583 DOI: 10 .1124 /mol.107 .042382 ]
18 Feng X, Zhang Y, Li T, Li Y. Sequentially administrated of pemetrexed with icotinib/erlotinib in lung adenocarcinoma cell lines
.
2017 ; 8 : 114292 -114299 [PMID: 29371987 DOI: 10 .18632 /oncotarget.23224 ]
19 Kubo E, Yamamoto N, Nokihara H, Fujiwara Y, Horinouchi H, Kanda S, Goto Y, Ohe Y. Randomized phase II study of sequential carboplatin plus paclitaxel and gefitinib in chemotherapy-naïve patients with advanced or metastatic non-smallcell lung cancer: Long-term follow-up results.
2017 ; 6 : 56 -62 [PMID: 28123729 DOI:10 .3892 /mco.2016 .1076 ]
20 Choi YJ, Lee DH, Choi CM, Lee JS, Lee SJ, Ahn JH, Kim SW. Randomized phase II study of paclitaxel/carboplatin intercalated with gefitinib compared to paclitaxel/carboplatin alone for chemotherapy-naïve non-small cell lung cancer in a clinically selected population excluding patients with non-smoking adenocarcinoma or mutated EGFR.
2015 ;15 : 763 [PMID: 26493267 DOI: 10 .1186 /s12885 -015 -1714 -y]
21 Patil VM, Noronha V, Joshi A, Choughule AB, Bhattacharjee A, Kumar R, Goud S, More S, Ramaswamy A, Karpe A,Pande N, Chandrasekharan A, Goel A, Talreja V, Mahajan A, Janu A, Purandare N, Prabhash K. Phase III study of gefitinib or pemetrexed with carboplatin in EGFR-mutated advanced lung adenocarcinoma.
2017 ; 2 : e000168 [PMID:28761735 DOI: 10 .1136 /esmoopen-2017 -000168 ]
22 Wang MC, Liang X, Liu ZY, Cui J, Liu Y, Jing L, Jiang LL, Ma JQ, Han LL, Guo QQ, Yang CC, Wang J, Wu T, Nan KJ,Yao Y. In vitro synergistic antitumor efficacy of sequentially combined chemotherapy/icotinib in nonsmall cell lung cancer cell lines.
2015 ; 33 : 239 -249 [PMID: 25370413 DOI: 10 .3892 /or.2014 .3583 ]
23 Zhang Y, Wang J, Yu Z, Ge H, Zhang LW, Feng LX. Outcomes of concurrent versus sequential icotinib therapy and chemotherapy in advanced non-small cell lung cancer with sensitive EGFR mutations.
2021 ; 14 : 890 -897[PMID: 33382908 DOI: 10 .1111 /cts.12951 ]
24 Zheng Y, Fang W, Deng J, Zhao P, Xu N, Zhou J. Sequential treatment of icotinib after first-line pemetrexed in advanced lung adenocarcinoma with unknown EGFR gene status.
2014 ; 6 : 958 -964 [PMID: 25093093 DOI:10 .3978 /j.issn.2072 -1439 .2014 .07 .18 ]
25 Nishino M, Jackman DM, Hatabu H, Yeap BY, Cioffredi LA, Yap JT, Jänne PA, Johnson BE, Van den Abbeele AD. New Response Evaluation Criteria in Solid Tumors (RECIST) guidelines for advanced non-small cell lung cancer: comparison with original RECIST and impact on assessment of tumor response to targeted therapy.
2010 ; 195 :W221 -W228 [PMID: 20729419 DOI: 10 .2214 /AJR.09 .3928 ]
26 Herbst RS, Prager D, Hermann R, Fehrenbacher L, Johnson BE, Sandler A, Kris MG, Tran HT, Klein P, Li X, Ramies D,Johnson DH, Miller VA; TRIBUTE Investigator Group. TRIBUTE: a phase III trial of erlotinib hydrochloride (OSI-774 )combined with carboplatin and paclitaxel chemotherapy in advanced non-small-cell lung cancer.
2005 ; 23 :5892 -5899 [PMID: 16043829 DOI: 10 .1200 /jco.2005 .02 .840 ]
27 Johnson DH. Targeted therapies in combination with chemotherapy in non-small cell lung cancer. Clin Cancer Res 2006 ;12 : 4451 s-4457 s [PMID: 16857827 DOI: 10 .1158 /1078 -0432 .CCR-06 -0095 ]
28 Davies AM, Ho C, Lara PN Jr, Mack P, Gumerlock PH, Gandara DR. Pharmacodynamic separation of epidermal growth factor receptor tyrosine kinase inhibitors and chemotherapy in non-small-cell lung cancer.
2006 ; 7 : 385 -388 [PMID: 16800963 DOI: 10 .3816 /CLC.2006 .n.021 ]
29 Zhou C, Wu YL, Liu X, Wang CL, Chen GY, Feng JF, Zhang SC, Wang J, Zhou SW, Ren SX, Lu S, Zhang L, Hu CP,Luo Y, Chen L, Ye M, Huang JN, Zhi XY, Zhang YP, Xiu QY. Overall survival (OS) results from OPTIMAL(CTONG0802 ), a phase III trial of erlotinib (E) vs carboplatin plus gemcitabine (GC) as first-line treatment for Chinese patients with EGFR mutation-positive advanced non-small cell lung cancer (NSCLC).
2012 ; 30 : 7520 [DOI:10 .1200 /jco.2012 .30 .15 _suppl.7520 ]
30 Sugawara S, Oizumi S, Minato K, Harada T, Inoue A, Fujita Y, Maemondo M, Yoshizawa H, Ito K, Gemma A, Nishitsuji M, Harada M, Isobe H, Kinoshita I, Morita S, Kobayashi K, Hagiwara K, Kurihara M, Nukiwa T. Randomized phase II study of concurrent versus sequential alternating gefitinib and chemotherapy in previously untreated non-small cell lung cancer with sensitive EGFR mutations: NEJ005 /TCOG0902 . Ann Oncol 2015 ; 26 : 888 -894 [PMID: 25669832 DOI:10 .1093 /annonc/mdv063 ]
31 Yang JC, Cheng Y, Murakami H, Yang PC, He J, Nakagawa K, Kang JH, Kim JH, Hozak RR, Nguyen TS, Zhang WL,Enatsu S, Puri T, Orlando M. A Randomized Phase 2 Study of Gefitinib With or Without Pemetrexed as First-line Treatment in Nonsquamous NSCLC With EGFR Mutation: Final Overall Survival and Biomarker Analysis.
2020 ; 15 : 91 -100 [PMID: 31605797 DOI: 10 .1016 /j.jtho.2019 .09 .008 ]
32 Nakamura A, Inoue A, Morita S, Hosomi Y, Kato T, Fukuhara T, Gemma A, Takahashi K, Fujita Y, Harada T, Minato K,Takamura K, Kobayashi K, Nukiwa T. Phase III study comparing gefitinib monotherapy (G) to combination therapy with gefitinib, carboplatin, and pemetrexed (GCP) for untreated patients (pts) with advanced non-small cell lung cancer(NSCLC) with EGFR mutations (NEJ009 ). J Clin Oncol 2018 ; 36 : 9005 [DOI: 10 .1200 /jco.2018 .36 .15 _suppl.9005 ]
33 Noronha V, Patil VM, Joshi A, Menon N, Chougule A, Mahajan A, Janu A, Purandare N, Kumar R, More S, Goud S,Kadam N, Daware N, Bhattacharjee A, Shah S, Yadav A, Trivedi V, Behel V, Dutt A, Banavali SD, Prabhash K. Gefitinib Versus Gefitinib Plus Pemetrexed and Carboplatin Chemotherapy in EGFR-Mutated Lung Cancer.
2020 ; 38 :124 -136 [PMID: 31411950 DOI: 10 .1200 /JCO.19 .01154 ]
34 Zhang L, Qi Y, Xing K, Qian S, Zhang P, Wu X. A novel strategy of EGFRTKI combined chemotherapy in the treatment of human lung cancer with EGFRsensitive mutation.
2018 ; 40 : 1046 -1054 [PMID: 29917169 DOI:10 .3892 /or.2018 .6499 ]
35 Wen M, Xia J, Sun Y, Wang X, Fu X, Zhang Y, Zhang Z, Zhou Y, Li X. Combination of EGFR-TKIs with chemotherapy versus chemotherapy or EGFR-TKIs alone in advanced NSCLC patients with EGFR mutation.
2018 ; 12 : 183 -190 [PMID: 30555222 DOI: 10 .2147 /BTT.S169305 ]
36 Yan X, Wang H, Li P, Zhang G, Zhang M, Yang J, Zhang X, Zheng X, Ma Z. Efficacy of first-line treatment with epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) alone or in combination with chemotherapy for advanced non-small cell lung cancer (NSCLC) with low-abundance mutation.
2019 ; 128 : 6 -12 [PMID:30642455 DOI: 10 .1016 /j.lungcan.2018 .12 .007 ]
37 Yang JC, Kang JH, Mok T, Ahn MJ, Srimuninnimit V, Lin CC, Kim DW, Tsai CM, Barraclough H, Altug S, Orlando M,Park K. First-line pemetrexed plus cisplatin followed by gefitinib maintenance therapy versus gefitinib monotherapy in East Asian patients with locally advanced or metastatic non-squamous non-small cell lung cancer: a randomised, phase 3 trial.
2014 ; 50 : 2219 -2230 [PMID: 24953333 DOI: 10 .1016 /j.ejca.2014 .05 .011 ]
38 Yang JC, Srimuninnimit V, Ahn MJ, Lin CC, Kim SW, Tsai CM, Mok T, Orlando M, Puri T, Wang X, Park K. First-Line Pemetrexed plus Cisplatin followed by Gefitinib Maintenance Therapy versus Gefitinib Monotherapy in East Asian Never-Smoker Patients with Locally Advanced or Metastatic Nonsquamous Non-Small Cell Lung Cancer: Final Overall Survival Results from a Randomized Phase 3 Study. J Thorac Oncol 2016 ; 11 : 370 -379 [PMID: 26725183 DOI:10 .1016 /j.jtho.2015 .11 .008 ]
39 Patil PD, Shepherd F, Johnson DH. A Career in Lung Cancer: Pushing Beyond Chemotherapy.
2019 ; 39 : 583 -589 [PMID: 31099660 DOI: 10 .1200 /EDBK_239397 ]
40 Lim ZF, Ma PC. Emerging insights of tumor heterogeneity and drug resistance mechanisms in lung cancer targeted therapy.
2019 ; 12 : 134 [PMID: 31815659 DOI: 10 .1186 /s13045 -019 -0818 -2 ]
41 Cheng Y, He Y, Li W, Zhang HL, Zhou Q, Wang B, Liu C, Walding A, Saggese M, Huang X, Fan M, Wang J,Ramalingam SS. Osimertinib Versus Comparator EGFR TKI as First-Line Treatment for EGFR-Mutated Advanced NSCLC: FLAURA China, A Randomized Study.
2021 ; 16 : 165 -176 [PMID: 33544337 DOI:10 .1007 /s11523 -021 -00794 -6 ]
42 Horinouchi H. To combine or not to combine: anti-vascular endothelial growth factor therapies in EGFR mutation positive non-small cell lung cancer.
2020 ; 8 : 554 [PMID: 32411777 DOI: 10 .21037 /atm.2020 .01 .66 ]
43 Rossi A, Chiodini P, Sun JM, O'Brien ME, von Plessen C, Barata F, Park K, Popat S, Bergman B, Parente B, Gallo C,Gridelli C, Perrone F, Di Maio M. Six versus fewer planned cycles of first-line platinum-based chemotherapy for nonsmall-cell lung cancer: a systematic review and meta-analysis of individual patient data.
2014 ; 15 : 1254 -1262 [PMID: 25232001 DOI: 10 .1016 /S1470 -2045 (14 )70402 -4 ]
44 Tartarone A, Roviello G, Lerose R, Roudi R, Aieta M, Zoppoli P. Anti-PD-1 versus anti-PD-L1 therapy in patients with pretreated advanced non-small-cell lung cancer: a meta-analysis.
2019 ; 15 : 2423 -2433 [PMID: 31237152 DOI: 10 .2217 /fon-2018 -0868 ]
45 Mohsenzadegan M, Peng RW, Roudi R. Dendritic cell/cytokine-induced killer cell-based immunotherapy in lung cancer:What we know and future landscape.
2020 ; 235 : 74 -86 [PMID: 31222740 DOI: 10 .1002 /jcp.28977 ]
46 Petrelli F, Ferrara R, Signorelli D, Ghidini A, Proto C, Roudi R, Sabet MN, Facelli S, Garassino MC, Luciani A, Roviello G. Immune checkpoint inhibitors and chemotherapy in first-line NSCLC: a meta-analysis.
2021 ; 13 : 621 -631 [PMID: 33775103 DOI: 10 .2217 /imt-2020 -0224 ]
47 Petrelli F, Ghidini A, Luciani A. Topotecan or other agents as second-line therapy for relapsed small-cell lung cancer: A meta-analysis of randomized studies.
2021 ; 15 : 218 [PMID: 34476102 DOI: 10 .3892 /mco.2021 .2383 ]
48 NCCN Clincal Practice Guidelines in Oncology (NCCN Guidelines). Non-Small Cell Lung Cancer. Version 2 .2020 . Fort Washington: National Comprehensive Cancer Network, 2019
49 Rebuzzi SE, Alfieri R, La Monica S, Minari R, Petronini PG, Tiseo M. Combination of EGFR-TKIs and chemotherapy in advanced EGFR mutated NSCLC: Review of the literature and future perspectives.
2020 ; 146 :102820 [PMID: 31785991 DOI: 10 .1016 /j.critrevonc.2019 .102820 ]
50 Jin R, Zhao J, Xia L, Li Q, Li W, Peng L, Xia Y. Application of immune checkpoint inhibitors in EGFR-mutant non-smallcell lung cancer: from bed to bench.
2020 ; 12 : 1758835920930333 [PMID: 32565926 DOI:10 .1177 /1758835920930333 ]
51 Ito T, Nagashima H, Akiyama M, Utsumi Y, Sato H, Chiba S, Sugai M, Ube K, Mori Y, Watanabe K, Fukuhara T,Maemondo M. Treatment with immune checkpoint inhibitors after EGFR-TKIs in EGFR-mutated lung cancer.
2022 ; 13 : 386 -393 [PMID: 34904383 DOI: 10 .1111 /1759 -7714 .14267 ]
52 Wiest N, Majeed U, Seegobin K, Zhao Y, Lou Y, Manochakian R. Role of Immune Checkpoint Inhibitor Therapy in Advanced
-Mutant Non-Small Cell Lung Cancer.
2021 ; 11 : 751209 [PMID: 34868953 DOI:10 .3389 /fonc.2021 .751209 ]
53 Qiao M, Jiang T, Liu X, Mao S, Zhou F, Li X, Zhao C, Chen X, Su C, Ren S, Zhou C. Immune Checkpoint Inhibitors in EGFR-Mutated NSCLC: Dusk or Dawn?
2021 ; 16 : 1267 -1288 [PMID: 33915248 DOI:10 .1016 /j.jtho.2021 .04 .003 ]
54 Creelan BC, Yeh TC, Kim SW, Nogami N, Kim DW, Chow LQM, Kanda S, Taylor R, Tang W, Tang M, Angell HK,Roudier MP, Marotti M, Gibbons DL. A Phase 1 study of gefitinib combined with durvalumab in EGFR TKI-naive patients with EGFR mutation-positive locally advanced/metastatic non-small-cell lung cancer.
2021 ; 124 : 383 -390[PMID: 33012782 DOI: 10 .1038 /s41416 -020 -01099 -7 ]
55 Yang JC, Gadgeel SM, Sequist LV, Wu CL, Papadimitrakopoulou VA, Su WC, Fiore J, Saraf S, Raftopoulos H, Patnaik A. Pembrolizumab in Combination With Erlotinib or Gefitinib as First-Line Therapy for Advanced NSCLC With Sensitizing EGFR Mutation.
2019 ; 14 : 553 -559 [PMID: 30529597 DOI: 10 .1016 /j.jtho.2018 .11 .028 ]
56 Ma BBY, Rudin CM, Cervantes A, Dowlati A. Preliminary Safety and Clinical Activity of Erlotinib Plus Atezolizumab From a Phase Ib Study in Advanced NSCLC.
2016 ; 27 : ix139 -ix156 [DOI: 10 .1093 /annonc/mdw594 .005 ]
57 Roviello G, Zanotti L, Cappelletti MR, Gobbi A, Dester M, Paganini G, Pacifico C, Generali D, Roudi R. Are EGFR tyrosine kinase inhibitors effective in elderly patients with EGFR-mutated non-small cell lung cancer?
2018 ;18 : 15 -20 [PMID: 28391544 DOI: 10 .1007 /s10238 -017 -0460 -7 ]
猜你喜欢
中国动物保健(2022年2期)2022-05-05
中国现代医生(2022年6期)2022-04-23
中国典型病例大全(2022年9期)2022-04-19
健康体检与管理(2022年2期)2022-04-15
中国药学药品知识仓库(2022年2期)2022-03-23
智富时代(2018年5期)2018-07-18
智富时代(2018年5期)2018-07-18
计算机应用(2016年10期)2017-05-12
中学生数理化·七年级数学人教版(2016年6期)2016-05-14
海峡科学(2013年3期)2013-10-21
 World Journal of Clinical Cases2022年18期
World Journal of Clinical Cases2022年18期
- World Journal of Clinical Cases的其它文章
- Diabetes mellitus susceptibility with varied diseased phenotypes and its comparison with phenome interactome networks
- Impact of preoperative carbohydrate loading on gastric volume in patients with type 2 diabetes
- Disseminated strongyloidiasis in a patient with rheumatoid arthritis: A case report
- CYP27A1 mutation in a case of cerebrotendinous xanthomatosis: A case report
- Postoperative multiple metastasis of clear cell sarcoma-like tumor of the gastrointestinal tract in adolescent: A case report
- Efficacy and safety of adalimumab in comparison to infliximab for Crohn's disease: A systematic review and meta-analysis