
lntramedullary bone pedestal formation contributing to femoral shaft fracture nonunion: A case report and review of the literature
2022-05-30 05:51CharlesPasqueAlexanderPappasChadColeJr
World Journal of Orthopedics 2022年5期
lNTRODUCTlON
Diaphyseal femur fractures treated with reamed intramedullary nail fixation have a low incidence of nonunion[1-5]. Nonunions have been found to occur secondary to infection and a variety of aseptic etiologies. Aseptic nonunions have been associated with fracture instability, distraction, malalignment,large bony defects, and open fractures. These procedure and fracture associated factors prevent adequate blood supply to the fracture site and impede the healing response. Patient factors have also been linked to nonunions in some series. These may be factors that lead to poor blood supply such as vascular disease, diabetes, and smoking. Others have a more direct effect on the healing process by impeding the immune response and preventing the proper balance of osteoblast/osteoclast activity.These include the use of non-steroidal anti-inflammatory drugs (NSAIDs), use of steroids, advancing age, malignancy, and diabetes mellitus[6-11].
When an aseptic fracture nonunion occurs after intramedullary nail fixation, there are multiple methods of revision that have been studied and proven to be effective. Such methods include, nail dynamization, exchange nailing, and augmentative plating[4,5]. Causes of non-union after revision have been found to be similar to that of non-union after initial fixation, though the rare incidence of repeat non-union has led to sparse data on the topic. We present a unique case of mid-shaft femur fracture nonunion after nail dynamization due to intramedullary bone pedestal formation.
Then he jumped high into the air, and landed safe on the other side, and after turning round to be sure that there was no chance of anyone pursuing him, trotted14 happily home to his grandmother
CASE PRESENTATlON
Chief complaints
A 37-year-old white male presented to our clinic with 5 mo of left thigh pain with activity.
I didn t pay attention to my friend as I cautiously knelt down beside the lady who was now furiously attempting to set her cart upright once more. I could feel the inquiring, skeptical31 eyes of the passersby32. I knew they were thinking I was crazy for helping33 her or, worse, that I had clumsily knocked over her cart and therefore was assisting her out of duty.
History of present illness
The patient’s symptoms began when he was involved in a motocross accident in which he came down hard from a jump. He remarkably was able to hop to his car and drive himself to a nearby hospital where he was found to have an obvious deformity of the left thigh. Subsequent evaluation was consistent with an isolated, closed, left mid-shaft femur fracture.
Fracture dynamization by distal locking screw removal is often attempted initially for delayed unions. This method provides the advantages of short procedure time with minimal soft-tissue dissection. Wu showed a 58% union rate with dynamization between 4 and 12 mo, but a high rate (21%)of femoral shortening of more than 2 cm[12]. In one meta-analysis, Vaughn[13] found a 66%(84/131) union rate with dynamization after nonunion though this rate increased to 82% (45/55) when treating delayed union. This provides evidence for the importance of close follow-up after intramedullary nailing as dynamization is most effective in the earlier windows of fracture healing. A review of the literature did not yield any reports of cases of post-dynamization union failure secondary to intramedullary bone pedestal formation.
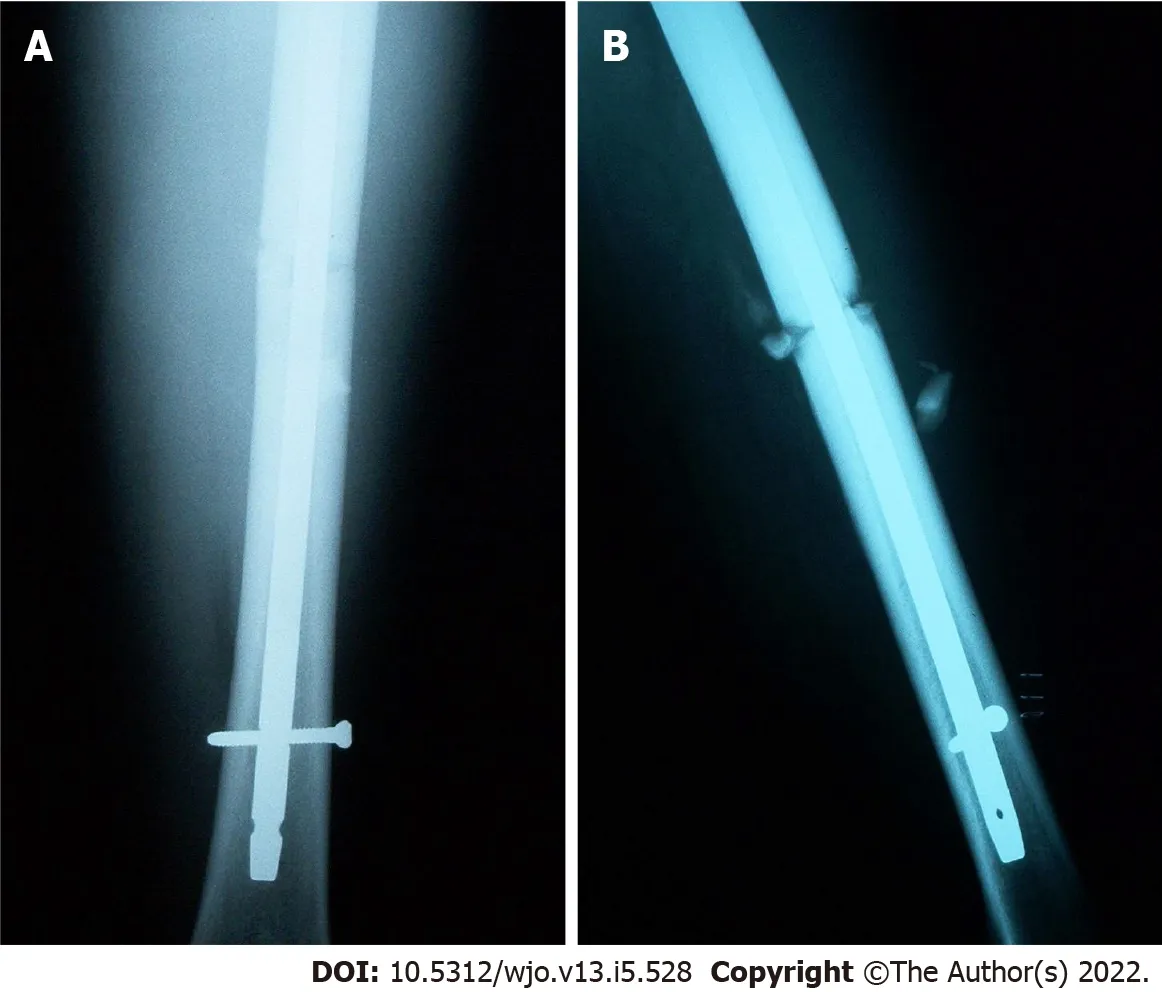
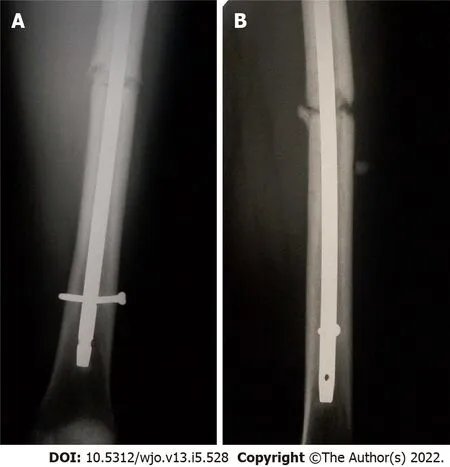
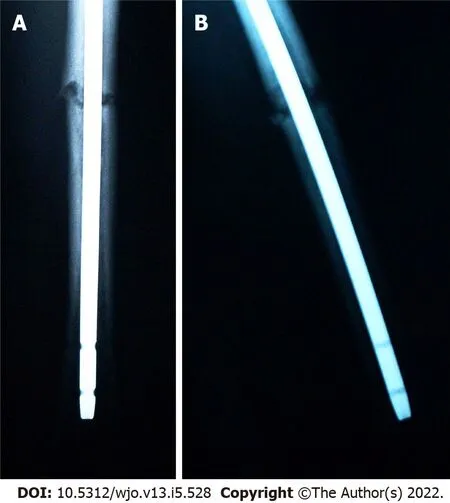
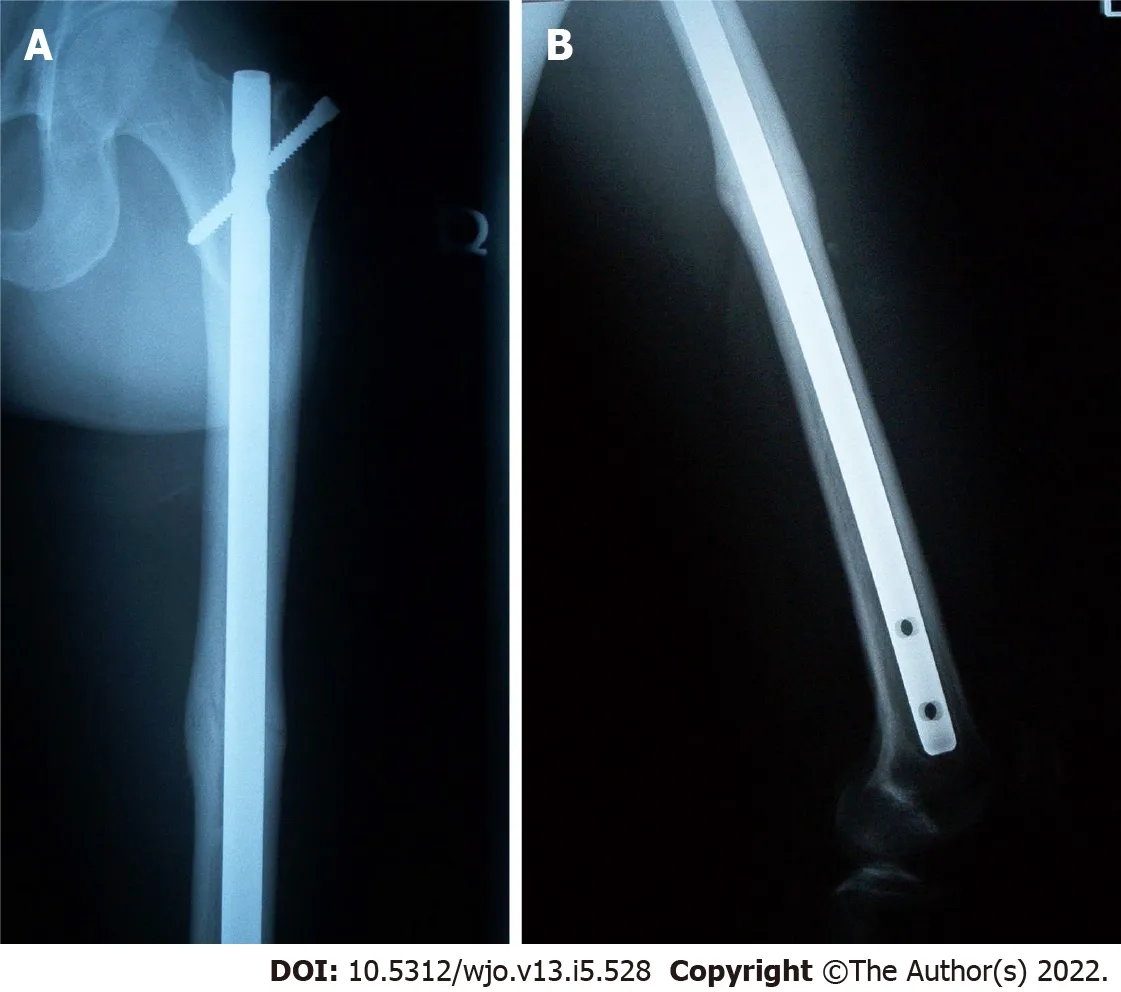
Post-operative radiographs from the outside hospital showed placement of 9 mm × 380 mm Russell-Taylor Delta II antegrade intramedullary nail through a left transverse mid-shaft femur fracture with single distal interlocking screw (Figure 1A and B). Radiographs obtained four months post-operatively at the outside hospital revealed breakage of the distal interlocking screw and no evidence of fracture union (Figure 2A and B). After presentation to our clinic, the decision was made to continue with normal weight bearing activity and obtain serial radiographs. Radiographs obtained 8 mo postoperatively continued to reveal no evidence of fracture union (Figure 3A and B).
History of past illness
The patient had no relevant previous medical history.
Personal and family history
The patient had no relevant personal or family medical history.
No, said the youth; he thought he had done enough, and was anxious to go to some other place to serve, and learn other people s ways; but he would, perhaps, come back to the troll some other time
Physical examination
The strengths of this case report include radiographs of the clinical course, a detailed description of the surgical techniques with deviations required to overcome the encountered complication, a discussion of how to clinically manage and prevent such pathology, and a review of all available literature on clinical management of femoral shaft fracture nonunion after intramedullary nail fixation.Weaknesses include limited access to some of the patient files from the outside hospital.
Well, Heavens. Didn t you ever come down here to the station? He pointed14 across to his magazine stand. I ve been there all the time. I own it. I ve watched everybody that came up the stairs. “,——?”。“。。。”
Cognac s leash and put the basket in his mouth. He was off like a shot, racing15 toward Brad with his beautiful golden ears streaming behind him, as if he was hot on the trail of a speeding rabbit. There was a swell16 of laughter as our guests appreciated the dedication17 of our furry18 ring- bearer.
Laboratory examinations
Baseline laboratory studies including an erythrocyte sedimentation rate were unremarkable.
Imaging examinations
4. Middle-sized Bear: As the three bears transformed into a nuclear family through various retellings, the middle-sized bear acquired feminine traits and became the mother/wife in the family.Return to place in story. #p#
FlNAL DlAGNOSlS
Aseptic nonunion of left femoral shaft fracture.
TREATMENT
The decision was made to proceed with exchange intramedullary nailing of the left femur.
Surgery
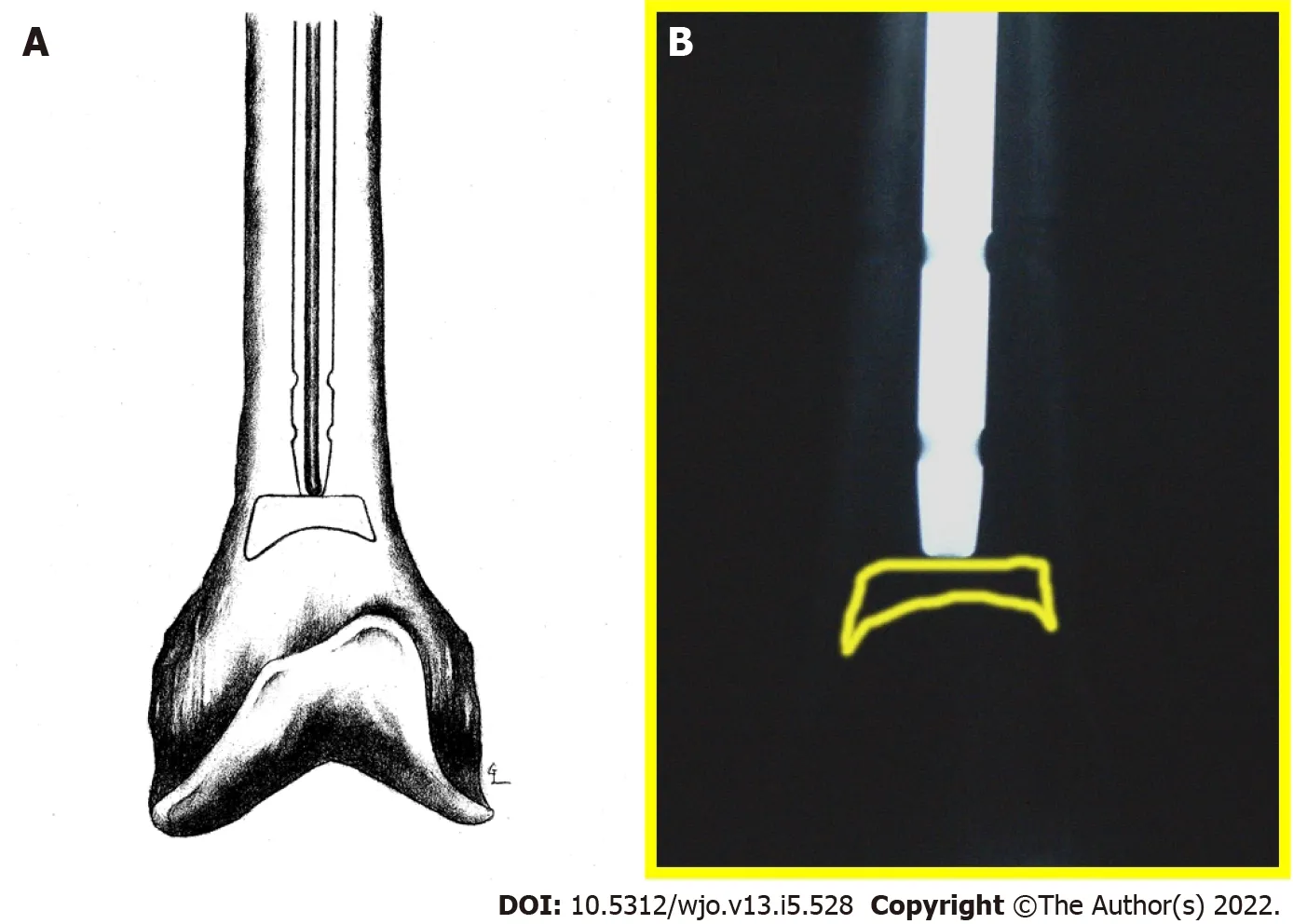
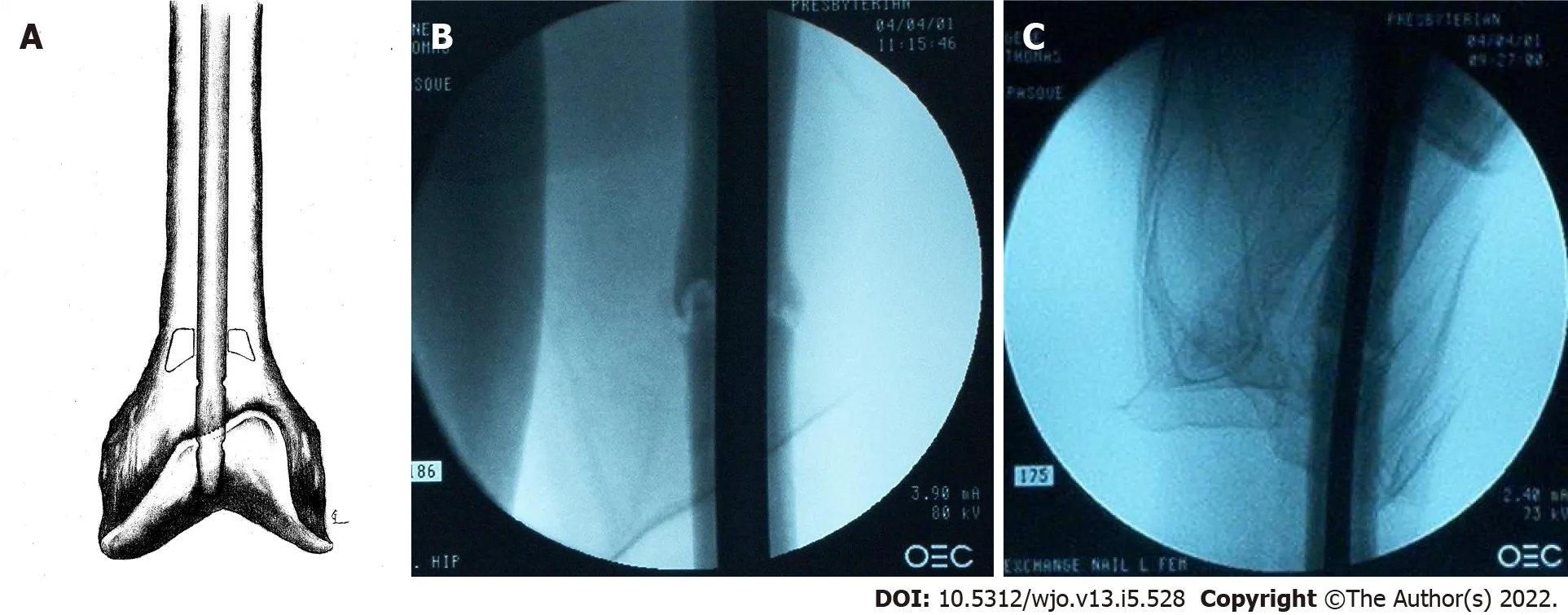
During nail extraction, attempts to pass a smooth-tip guide wire through the nail prior to removal were unsuccessful due to resistance at the nail tip (Figure 4A and B). The nail was subsequently removed with an appropriate nail extractor. Following nail removal, a standard guide wire was inserted into the canal without difficulty until it reached the point in the distal femur where the nail tip was previously seated. Again, the guide wire met resistance. Under magnified fluoroscopy, it appeared that there was a pedestal of cortical bone formation in the canal at this point (Figure 5A).
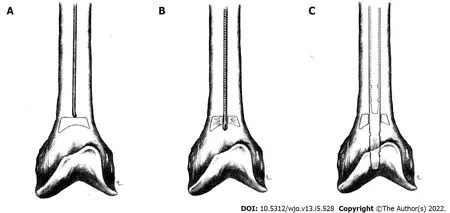
In order to breach the bony pedestal, the starting reamer was used to ream past the obstruction into the distal femoral meta-diaphyseal flare (Figure 5B). The ball-tip guide wire was then passed without difficulty to the physeal scar. The intramedullary canal was then reamed over the guide wire sequentially from 9 to 14 mm in 0.5 mm increments. The intramedullary reamings were saved for bone grafting and then inserted to the level of the fracture with the exchange tube. The bone graft was impacted using an 8 mm reamer at the fracture site. A 13 mm × 420 mm Russell-Taylor antegrade femoral nail was then inserted without difficulty. No distal locking screws were placed to allow fracture dynamization. Postoperative films showed adequate fracture reduction and placement of the intramedullary nail and proximal locking screw (Figure 6A-C). Figure 5C shows final nail placement (solid lines) compared to old, more proximal nail placement (dashed lines). Intra-operative cultures were subsequently negative.
Yes, I will gladly go with you, only how am I to get down out of the tower? Every time you come to see me you must bring a skein of silk with you, and I will make a ladder of them, and when it is finished I will climb down by it,36 and you will take me away on your horse.
OUTCOME AND FOLLOW-UP
At 1 year follow-up there was evidence of callus formation at the fracture site but not full cortical consolidation (Figure 7A and B). By 18 mo the fracture appeared well consolidated, and the patient had resolution of his thigh pain (Figure 8A and B).

DlSCUSSlON
Femoral shaft fracture nonunion is uncommon and is usually the result of aseptic etiologies. Nonunion following reamed antegrade intramedullary nail is a rare complication, occurring in 1%-2.2% of cases in early series[1-3]. In a recent systematic review of 38 studies involving 2829 femoral shaft fractures, Koso[4] found a 3.1% rate of nonunion after antegrade nail fixation and nonunion rates of 2.9% and 6.1%for reamedunreamed nail fixation, respectively.
There are numerous methods that may be used in the treatment of femur fracture nonunions. With infections, exchange intramedullary nailing should be performed after appropriate irrigation and debridement of the canal followed by an appropriate 4-6-wk course of parenteral or oral antibiotics.Some surgeons advocate a two-stage approach using antibiotic-impregnated beads or rods prior to final nail insertion. Aseptic nonunions may be treated with nail dynamization, exchange nailing (EN), or plate fixation. Several adjuncts may be employed in combination with these techniques, including bonegrafting, electrical stimulation, and bone morphogenetic protein or other bone growth supplements.
The patient underwent reamed antegrade intramedullary nail fixation of his left femur fracture at an outside hospital. Post-operative recovery was unremarkable except that he continued to have problems with left thigh pain during activity. Four months after his initial surgery, he was found to have broken his single distal locking screw, and he underwent distal locking screw removal for nail dynamization at the outside hospital. Left thigh pain with activity persisted five months post-operatively prompting presentation to our clinic.
I had a ticket. I had my passport. And he had cold feet. I might have known fairy tales don t come true. Seven months out of my marriage, I had met the great love of my life. We dated a year. I d always longed to see Europe, and, with my divorce final, we planned the trip together. Then two weeks before takeoff, he took off. Having piggybacked two breakups, I felt as if I d been through a double divorce. Here I was, thirty-nine years old, with two small children, and facing my ultimate fear: a life alone. Was I ready to spend a month in Europe by myself? I had a hard time going to a movie alone! But it did seem now or never. The kids would be with their dad, the money came as part of my property settlement, and I had a job waiting when I returned. Okay, if I was going to be lonely for the next few years, I might as well start by being lonely in Europe.
The treatment of femoral diaphyseal fracture nonunion or delayed union of any etiology has been found to have a varied (53%-100%) rate of union following exchange reamed IM nail fixation (EN)[5,14-25]. Due to the infrequency of nonunion, most case series examining outcomes of EN are of relatively small cohorts (< 105). The largest of these series showed rates of union from 86%-100%[14-21]. Some smaller (= 19) series have shown lower rates of union from 53%-58%[22,23]. Of note, four studies(including three meta-analyses) comparing EN to other methods of treatment for nonunion found rates of union from 64%-86%[5,13,24,25]. Infected nonunions have been shown to have union rates up to 90%-100% with intramedullary nail fixation[26-28]. Despite some small studies reporting poor results, the majority of the literature supports EN as an effective and safe method of fixation.
Advantages of exchange intramedullary nailing include limited soft-tissue dissection and periosteal blood supply disruption, full post-operative weight-bearing, and early active rehabilitation. Complications include persistent nonunion, infection, and hardware failure[12,21,22,26]. Current recommendations call for over-reaming the canal 1-3 mm and replacing the extracted nail with one of a larger diameter[5,7,19-21,23].
No, thank you, said Christian, I will have no more of that! As you please, said the king, you have behaved like a brave fellow, and now you shall have your breakfast
Adjuncts to nonunion surgical interventions include bone-grafting, bone morphogenetic protein,electrical stimulation, and extracorporeal shock. When treating nonunion with AP, bone grafting is recommended and has been shown to produce excellent results with union rates of 88%-100%[24,29,32,35-37]. Bone grafting can be implemented through open or closed (intramedullary over-reaming)techniques with equivalent efficacy (100% union)[38]. Closed methods have a shorter time to union[12] .Open methods require harvest from the iliac crest or the tibial condyle. General indications for open grafting include atrophic nonunions, large bony defects (> 5 mm), and fracture malalignment[33,38].
Plating techniques are sometimes employed in treating nonunions when dynamization and/or exchange nailing have failed. When large bony defects are present and open bone-grafting techniques are employed, plating techniques are often preferred for stabilization. Union rates of 91%-100% are observed with various plating techniques after removal of the failed nail[29-31]. Several case series have shown excellent results in patients treated with augmentative plating (AP) with retained IM nail after femoral shaft fracture nonunion with mean union rate of 86%-100%[24,32-36]. Two recent meta-analyses have shown a significantly higher union rate following AP with retained IM nail when compared to EN alone. In a systematic review of 21 studies involving 448 cases of nonunion after IM nailing for femoral shaft fracture, Medlock[25] reports union rates of 99.8% (190/191) and 74% (190/257) for AP and EN, respectively. In another systematic review of 3 studies involving 232 nonunions, Luo[5] found union rates of 100% (113/113) and 86% (102/119) for AP and EN, respectively. Indications for AP include non-isthmic nonunion or isthmic nonunion with cortical defects or IM canal widening[37].Advantages of AP over EN include lower rates of nonunion, shorter time to union, shorter operative time, and less intra-operative blood loss. Some of the disadvantages of plating include large soft tissue dissection, increased infection rate, and increased hardware failure.
Oh dear, no, said the old man. It would be no good charging that sort of price for a love potion, for example. Young people who need a love potion very seldom have five thousand dollars. Otherwise they would not need a love potion.
This case presentation and literature review covers the most recent literature on causes of femur fracture nonunion and methods of revision after intramedullary nail fixation. We propose a new etiology for femur fracture nonunion caused by intramedullary bone pedestal formation leading to failure of dynamization after distal interlocking screw removal. Through the use of intramedullary nails of maximum length and close fracture follow-up with early intervention when delayed or nonunion of a fracture is suspected, this rare complication can be prevented.
There are several causes for the development of femoral shaft fracture nonunions following IM nail fixation and a number of methods to treat these complications. We propose a new etiology of delayed union or nonunion due to intramedullary cortical bone pedestal formation at the IM nail tip leading to failure of dynamization following distal locking screw removal. This complication may have been prevented with the use of a longer IM nail during the initial fixation or earlier dynamization. With the nail tip resting more distally in an area of increased intramedullary diameter, there would theoretically be a decreased opportunity for formation of an intramedullary pedestal of bone that could bridge the distance between the femoral cortices. Earlier dynamization would have also decreased the time available for bone pedestal consolidation within the femoral canal. If exchange intramedullary nailing is required, it is important to ream past the previous nail tip region to allow appropriate dynamization/impaction of the fracture site. We also recommend not using distal interlocking screws in this situation unless the fracture pattern warrants it. Nonunion adjuncts may also be helpful such as bone graft and bone supplementation products or electrical stimulation.
The patient had a well-healed incisions without evidence of infection. He had left thigh pain to palpation and with weight bearing.
CONCLUSlON
Bai[39] obtained 16/17 fracture unions using plaster of Paris and bovine BMP composite implant at an average of 6 mo for femur fracture nonunion patients. In a systematic review comparing BMP and autologous grafting, Zhou[40] found BMP to have similar healing rates, improved limb function,and lower intraoperative blood loss, but with significantly higher hospitalization costs. While the literature on treatment of femoral nonunion with electrical stimulation is limited, electrical stimulation has shown some benefit for femur fractures[41], but is more commonly used and more successful with the treatment of tibia fracture nonunions[42].
FOOTNOTES
Pasque CB contributed to the conceptualization, design, data collection, methodology, project administration, supervision, writing, and revising of the manuscript; Pappas AJ contributed to the initial data collection and writing of the manuscript; Cole Jr CA contributed to the data analysis, literature review, and revision of the manuscript; and all authors have read and approved the final manuscript.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Each of the authors declare no conflict of interest.
The CARE checklist (2016) statement has been correctly completed. The file was previously sent to the reviewer.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
United States
Charles B Pasque 0000-0003-1205-2927; Alexander J Pappas 0000-0002-9641-7454; Chad A Cole Jr 0000-0001-5564-0476.
Wang JL
A
Wang JL
 World Journal of Orthopedics2022年5期
World Journal of Orthopedics2022年5期
- World Journal of Orthopedics的其它文章
- Coronal plane deformity around the knee in the skeletally immature population: A review of principles of evaluation and treatment
- Update in combined musculoskeletal and vascular injuries of the extremities
- lnsufficient lateral stem contact is an influencing factor for significant subsidence in cementless short stem total hip arthroplasty
- Distal femur complex fractures in elderly patients treated with megaprosthesis: Results in a case series of 11 patients
- Prevalence and factors of work-related musculoskeletal disorders among hand surgeons
- What factors are important to new patients when selecting an orthopedic oncologist?