
lnsufficient lateral stem contact is an influencing factor for significant subsidence in cementless short stem total hip arthroplasty
2022-05-30 05:51YingyongSuksathienPattawatChuvanichanonThanutTippimanchaiJithayutSueajui
World Journal of Orthopedics 2022年5期
lNTRODUCTlON
Cementless femoral stem in total hip arthroplasty (THA) is one of the most successful procedures in orthopaedic surgery[1]. Short stem THAs are commonly used in young and active patients. The advantages of these stems include more proximal load transfer which reduces stress shielding and,thigh pain, and they provide better options should revision surgery become necessary[2]. Short stem THA has shown excellent results in patients with primary osteoarthritis[3-5], osteonecrosis of the femoral head (ONFH)[6-9] and developmental dysplasia of the hip (DDH)[10,11] in many previous studies.
Subsidence is one of the concerning complications in cementless femoral fixation. It can lead to limb length discrepancy, decreased hip stability, or even implant failure. In conventional cementless stems,several previous studies have revealed the relationship between subsidence and stem survivorship[12,13], and some studies demonstrated the relationship between percentage of canal fill and subsidence[14,15]. However, few publications have studied the influencing factors for subsidence in short cementless stems, due to their metaphyseal anchoring without diaphyseal invasion, they might demonstrate different subsidence patterns than with the conventional stems. The purpose of this study is to analyze the factors associated with subsidence in short stems, including any radiographic parameters after a minimum of two years follow-up.
MATERlALS AND METHODS
This research has been approved by the IRB of the authors’ affiliated institutions. The digitized radiographs of patients who had undergone short stem THA in our institute between January 2011 and December 2018 were retrospectively reviewed. According to previous study showed that the short stem subsided at the initial phase of about 3-6 mo after implantation and then no further subsidence was observed at two years follow-up[16]. Therefore, the inclusion criteria in this study were patients aged >18 years with complete radiographic data at a minimum of two years follow-up. Because the Metha stem was designed for metaphyseal fitting without diaphyseal anchorage which suitable for patients with good bone quality, therefore, we excluded patients with osteoporotic bone. Patients with history of previous surgical treatment on the hip was also excluded.
It was an automobile3 accident when I was twelve, Amy explained. I was readingto my younger brother in the back seat and suddenly my mother screamed and tried frantically6 to miss the truck that had pulled out in front of us. When I woke up in the hospital, my mother was screaming again outside the door. This time she was trying to escape the fact that I would never walk again.
All THAs in this study were performed using Metha short stem by two experienced surgeons(Suksathien Y, Sueajui J), through a modified Hardinge approach. The Metha short stem is cementless,tapered, collarless, and made of titanium forged alloy (Ti6A14V) with suggested metaphyseal anchorage within the closed ring of the femoral neck. This stem is available in 5 sizes (0, 1, 2, 3 and 4)and 3 caput-column-diaphysis angles (120, 130and 135). The Metha short stem is round coated with Plasmapore, a calcium phosphate layer, for osseointegration (Figure 1). In all cases the femoral neck was cut above the notch of the femoral neck at an angle of 50to the femoral axis to create a closed cortical ring[17]. Intra-operative calcar cracks that occurred incidentally were routinely treated with cerclage wire. The Metha short stem was classified as type IIA according to Khanuja[18]; type I is femoral neck only, type II is calcar loading, type III is calcar loading with lateral flare, and type IV is shortened tapered stem. Additionally, type 2 stems are categorized into 4 subtypes: A, trapezoidal; B, round; C,threaded; and D, thrust plate. The cementless acetabular cup (Plasmafit, B.Braun Aesculap, Tuttlingen,Germany) with polyethelene liner (Vitelene, Vit E Stabilized Highly Crosslinked Polyethelene, B.Braun Aesculap, Tuttlingen, Germany) and metal head was used in all cases with the target angles for acetabular cup abduction and anteversion were 40° and 15° respectively. The femoral head diameter depended on cup size, 32 mm for cup diameter 50 mm or less, and 36 mm for cup diameter 52 mm or more.
Insufficient lateral stem contact was a statistically significant influencing factor on significant subsidence when using short stem. Therefore, it is a particularly important step to create proper lateral cortical contact when performing the Metha stem THA.

The seating height was also not a significant influencing factor for significant subsidence in this study(OR = 0.91; 95%CI: 0.3-2.9;= 0.87). Consistent with Floerkemeier[17], who studied synthetic bone using Metha stem and demonstrated that the deeper the resection, the more similar the strain patterns when compared to a non-implanted synthetic bone.
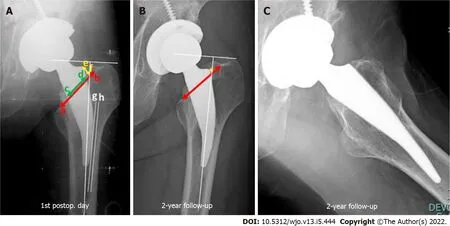
Pre-operative radiographs were assessed by using mediolateral cortical index as per Dorr[19].Post-operative AP digital radiographs were calibrated with known femoral head size to minimize magnification error. The line from upper border of lessor trochanter to the notch of the femoral neck was defined as the base of femoral neck level. The Metha stem is designed for metaphyseal anchorage within the cortical ring of the femoral neck[17]; therefore, the neck-filling ratio (NFR) at the base of femoral neck level was defined, as the implant width divided by the distance from the inner cortex of the medial femoral neck to the inner cortex of the notch of the femoral neck. The distance from the shoulder point of the stem perpendicular to the base of the femoral neck level in millimeters was defined as the seating height of the femoral stem. Stem subsidence was calculated as the different distance from the shoulder point of the stem to the most prominent point of the greater trochanter between the first post-operative day and at two years follow-up by AP radiograph[20]. The subsidence threshold of more than 3 mm was considered as clinically significant subsidence[21,22]. A lateral stem contact was defined as the distance between the most lateral point of the stem and the inner lateral femoral cortex; a distance of less than 1 mm was defined as sufficient contact[23] (Figure 2).
What can be the reason for such a crowd close by the pigsty? said theEmperor, who happened just then to step out on the balcony; he rubbed hiseyes, and put on his spectacles. They are the ladies of the court; I must godown and see what they are about! So he pulled up his slippers at the heel,for he had trodden them down.
Two independent observers (Tippimanchai T, Chuvanichanon P) measured each radiograph, and measurements were averaged into one final value after confirming that data reliability between the observers was sufficient. For the intra-observer reliability, the intraclass correlation coefficients (ICCs)for NFR were 0.85 (95%CI: 0.72-0.93) and 0.83 (95%CI: 0.68-0.91), for seating height they were 0.99(95%CI: 0.99-0.99) and 0.98 (95%CI: 0.98-0.99), for lateral stem contact they were 0.98 (95%CI: 0.97-0.99)and 0.97 (95%CI: 0.95-0.99) and for subsidence they were 0.99 (95%CI: 0.99-0.99) and 0.99 (95%CI: 0.99-1.0) for observer 1 and observer 2, respectively. For the inter-observer reliability, the ICC for NFR was 0.77 (95%CI: 0.71-0.81), for seating height it was 0.99 (95%CI: 0.99-0.99), lateral stem contact was 0.97(95%CI: 0.96-0.98), and subsidence was 0.99 (95%CI: 0.98-0.99) (Table 1).
The prince was not a little surprised, but he consented to hide himself with Asmund behind the panelling of the room, from where they could see all that went on through a little slit24

Statistical analysis
The mean, SD, lowest and highest values, and ratio were used in the descriptive statistics of data. Mean subsidence between NFR < 0.8 and ≥ 0.8, seating height < 5 and ≥ 5 mm and lateral stem contact < 1 and≥ 1 mm groups were compared using unpaired-test. Univariate regression analysis was used to identify the factors related to significant subsidence including age (≥ 60 yr), diagnosis, body mass index(BMI) (≥ 30 kg/m), Dorr’s type B, NFR (< 0.8)[24], seating height (< 5 mm)[17], and insufficient lateral stem contact (≥ 1 mm)[23]. Multivariate regression analysis was also conducted to assess the effect of insufficient lateral stem contact on significant subsidence. SPSS version 25.0 (SPSS Inc., Chicago, IL) was used for all statistical analyses with< 0.05 defined as statistically significant.
RESULTS
Many previous studies have shown satisfactory results using conventional total hip arthroplasty (THA), there may have some clinical problems related to proximodistal dimensional mismatch, thigh pain, stress shielding, periprosthetic fracture and difficulty during removal when revision is necessary. In an effort to reduce these problems, short-stem THA was developed, because the short stem has a metaphyseal fitting and no diaphyseal anchoring, so these problems may be minimized.
The store owner smiled and whistled and out of the kennel2 came Lady, who ran down the aisle3 of his store followed by five teeny tiny balls of fur. One puppy was lagging considerable behind. Immediately the little boy singled out the lagging limping puppy and said, “What’s wrong with that little dog?”
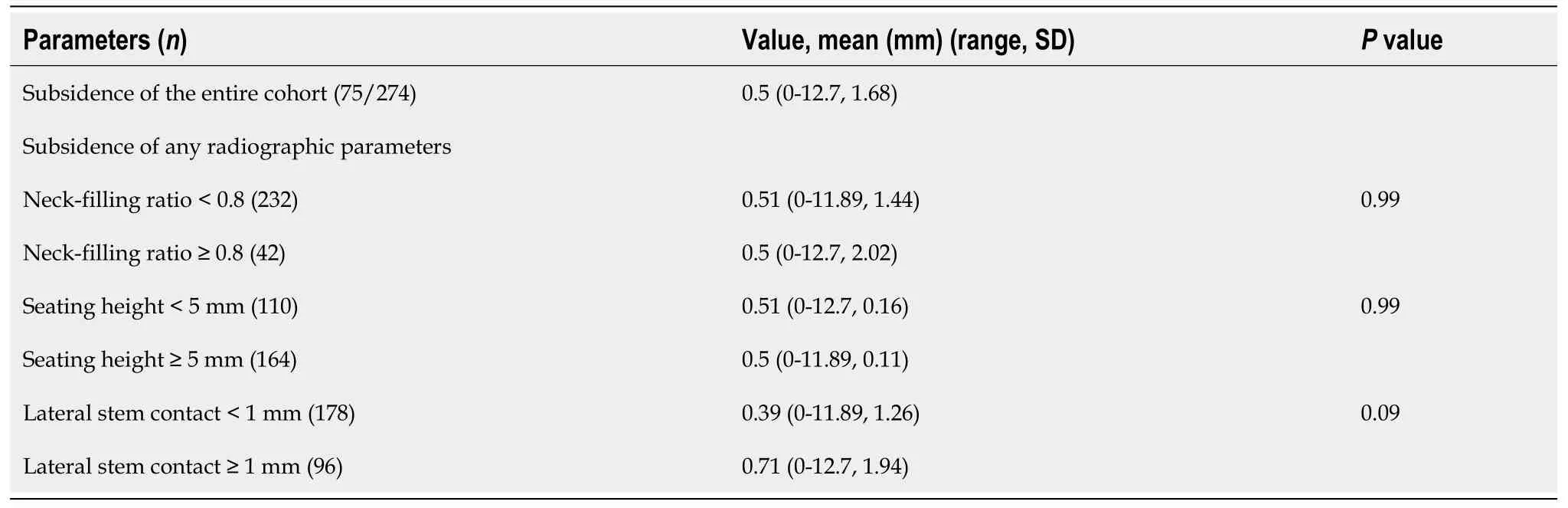
For the entire cohort, subsidence occurred in 75 cases (27.4%) with the mean stem subsidence of 0.5 mm. (0-12.7, 1.68). In most subsided cases the subsidence was occurred at the initial phase of about 3-6 mo after surgery and then no further subsidence was observed at two years follow-up. For the radiographic parameters, the mean subsidence of NFR < 0.8 and ≥ 0.8 groups were 0.5 mm. (0-11.89,1.44) and 0.5 mm. (0-12.7, 2.02), of seating height < 5 and ≥ 5 mm groups were 0.51 mm. (0-12.7, 0.16)and 0.50 mm. (0-11.89, 0.11) respectively, there was no statistically significant difference with= 0.99 in both compared groups. The mean subsidence of lateral stem contact < 1 and ≥ 1 mm groups were 0.39 mm. (0-11.89, 1.26) and 0.71 mm. (0-12.7, 1.94) respectively, there was no statistically significant difference (= 0.09) (Table 3). Lateral cortical hypertrophy was detected on two years follow-up APradiograph in 10 cases (5.03%) of non-subsided group and 3 cases (4%) in subsided group.
In the entire cohort, we found higher subsidence in insufficient lateral stem contact group than in sufficient group, but did not reach statistical significance. In significant subsidence cohort, the only statistically significant influencing factor for significant subsidence was insufficient lateral stem contact.Therefore, it is a particularly important step to create proper lateral cortical contact when performing the Metha stem THA and intra-operative fluoroscopy should be considered mandatory in some cases with doubtful lateral contact. Initial partial weight bearing should be recommended in patients whose post-operative radiographs demonstrate insufficient lateral cortical contact for preventing stem subsidence.
At the latest follow-up, there were 3 cases of revision. One case of femoral stem revision due to periprosthetic fracture, 4 years after index surgery from trauma, we revised using conventional stem with plate and screws and there were 2 cases of cup revision due to aseptic loosening, 2 and 5 years after index surgery. There was 1 case of significant subsidence (5.6 mm) with posterior dislocation, 5 years after index surgery from minor trauma, which was successfully treated with closed reduction. There was no femoral stem revision for aseptic loosening in our cohort.
DlSCUSSlON
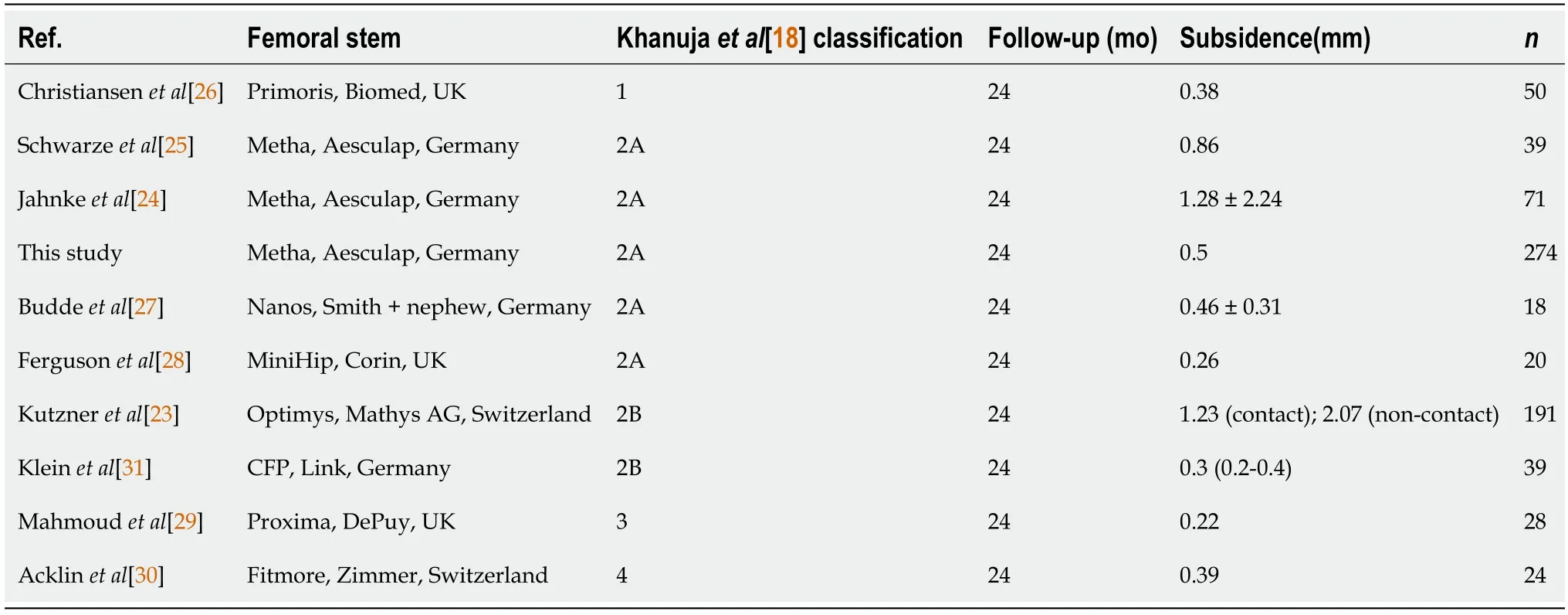
Subsidence is one of the concerning early complications when using the cementless short stem. In this study we found subsidence occurred in 75 cases (27.4%) with the mean stem subsidence for the entirecohort of 0.5 mm, (0-12.7, 1.68), a finding consistent with Jahnke[24], who demonstrated mean subsidence of 1.01 ± 1.27 mm (0.05-8.23) at two years follow-up. Schwarze[25] also showed the mean subsidence of 0.86 mm with two years follow-up using Metha stem. Different results of subsidence at two years follow-up were reported from many previous studies[23-30] using different types of short stem according to Khanuja[18]. Klein[31] who studied short stem with collar,CFP stem (LINK, Germany) (type IIB), demonstrated that the mean subsidence was 0.3 mm (0.2-0.4) at two years follow-up (Table 5).
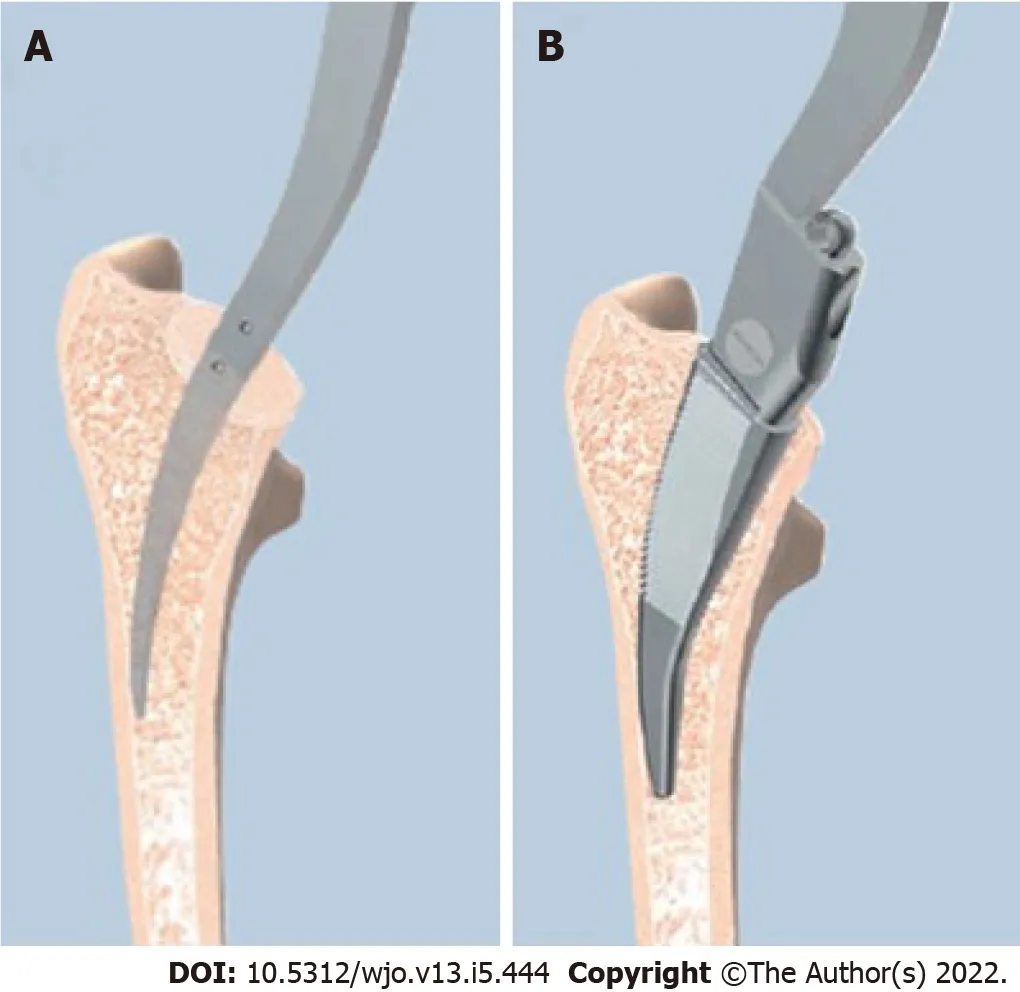
It is particularly important to identify the key intraoperative decision criteria to predict postimplantation subsidence of the short stem, which should be useful for choosing the proper size and position of the short stem and for allowance of early weight bearing post-operatively. In this study we demonstrated that the insufficient lateral stem contact group (≥ 1 mm) seemed to have higher subsidence than the sufficient lateral stem contact group (< 1 mm) in the entire cohort, but did not reach statistical significance (= 0.09). For significant subsidence cohort, the only significant influencing factor was insufficient lateral stem contact, the univariate and multivariate regression analyses showed statistical significance, (OR = 5.02; 95%CI: 1.3-18.9;= 0.017) and (OR = 5.5; 95%CI: 1.4-21.4;= 0.014)respectively. This is consistent with Kutzner[23], whose study using Optimys stem (type IIB according to Khanuja[18]), demonstrated that the mean subsidence was significantly higher in the no-contact group (≥ 1 mm) (2.07 mm, range -7.7 to 1.7) than in the sufficient lateral contact group (< 1 mm) (1.23 mm, range -4.5 to 1.8) at five years follow-up. According to our findings, sufficient lateral contact should always be the intra-operative aim when using Metha short stem. It is a particularly important step that when starting to prepare the femoral stem with a curved awl, the surgeon should carefully check that it be in contact with the lateral cortical bone, then followed by rasping in the same direction until reaching the designed femoral size (Figure 3). Therefore, intra-operative fluoroscopy might be considered mandatory in some cases with doubtful lateral contact. Nevertheless, if postoperative radiographs show that the patient has insufficient lateral contact, initial partial weight bearing should be recommended for preventing stem subsidence.
“No, no,” I said. “I’ll be all right. Just bring me a glass of water.”“Yes, sir, right away,” he said. “Would you prefer imported mineral water, sparkling water or club soda15 with a wedge of lime?”
Some studies have demonstrated the relationship between percentage of canal fill and subsidence in conventional cementless stems[14,15]. In short stems, Jahnke[24] studied fit and fill ratios in 40 patients using Metha stem with one year follow-up. They found 100% of cases had a tight fit and fill ratio (≥ 0.8) at the proximal level, and the mean subsidence in the whole cohort of their study was 1.28 ±2.24 mm. In our own study, we could not find a significant correlation between NFR (< 0.8) and significant subsidence (OR = 1.98; 95%CI: 0.2-15.7;= 0.52). One possible explanation might be that we found the cortical ring of the femoral neck in some patients had a flat oval shape, with the result that the proximal stem had stable fixation with the anterior and posterior neck, instead of mediolateral.
Patients were allowed to stand and progress to full weight-bearing using crutches on the second postoperative day. The standard protocol for anteroposterior (AP) digital radiograph of both hips with both legs at 15° internal rotation and lateral cross-table, to control femoral stem rotation, was taken on the first post-operative day and at each follow-up radiograph. Patients were routinely contacted every three months in the first post-operative year and then every six months thereafter.
In our cohort, age (≥ 60 yrs.), diagnosis, BMI (≥ 30 kg/m), and Dorr’s type B had no statistically significant influence on significant subsidence. Interestingly, patients with ONFH and Dorr’s type B seemed to have higher chance of having significant subsidence, but did not reach statistical significance,(OR = 3.3; 95%CI: 0.4-25.8;= 0.26) and (OR = 2.29; 95%CI: 0.6-7.9;= 0.19) respectively. Similar to Schaer[32] who studied Optimys stem (type IIB according to Khanuja[18]) with subsidence of2.04 ± 1.42 mm at five years follow-up, reported that age (≥ 65 yrs.), BMI (≥ 30 kg/m), and Dorr’s type B did not have a statistically significant impact on the amount of stem subsidence.
Press-fit is one of the key factors for stability of cementless stems. The surgeon is guided by visual,sensory, and auditory clues during insertion of the short stem; a good balance between perfect press-fit level and not fracturing the calcar remains challenging. In this study, the incidence of intra-operative calcar crack was 6.6% (18/274) and all cases were treated with cerclage wire with no further subsidence.We believe this was because of the relatively narrow neck diameter of patients in our country. As in our previous mid-term study of Metha short stem in patients with ONFH, Suksathien[9] reported 4.8%of intra-operative calcar crack treated with cerclage wire without any complication. Lateral cortical hypertrophy was detected in both non-subsided and subsided groups at two yeas follow-up, 10 cases(5.03%) and 3 cases (4%) respectively. This finding demonstrated that lateral cortical hypertrophy had no influence for stem subsidence. In most subsided cases the subsidence was occurred at the initial phase of about 3-6 mo after surgery and then no further subsidence was observed at two years followup.
14. Seven: The number seven is the number of completeness and totality - it is the sum of three (the number of the heavens - the triple goddess, the trinity) and four (the number of the earth which has four corners, four elements, four winds, four seasons, etc). Seven is a manifestatin of the cosmic order, a symbol of perfection and fullness, and also of introspection, meditation and understanding.
In a few minutes the toad stood in front of him and asked, What s the matter with you now, my dear Prince? Oh, Puddocky, this time you can t help me, for the task is beyond even your power, replied the Prince
This study had some limitations. First, we used digital radiographs to measure all radiographic parameters, which is less accurate than radiostereometric analysis. Nevertheless, the aim of this study was to describe intraoperative key decision criteria with respect to proper positioning of short stems,that are suitable for intraoperative use by all surgeons, solely by performing intraoperative fluoroscopy,and post-operative radiographic evaluation of influencing factors to prevent stem subsidence. Second,our cohort was a consecutive study of Metha stem, which was classified as type IIA according to Khanuja[18], the surgical technique for femoral preparation might be different from type I, III and IV. Third, there were many patients which loss before two years follow-up in our cohort, most of them were young workers, after fully recovery from THAs they moved to work in any remote area which unable to contact. However, there was no record of any complication at their last follow-up. Fourth, our cohort was relatively small which we had only 12 cases with significant subsidence to analyze, resulting in a relatively low power to detect statistically significant difference. Finally, this study was a single institute experience; different outcomes might have been obtained by different surgeons with varying levels of experience in any type of short stem THA.
CONCLUSlON
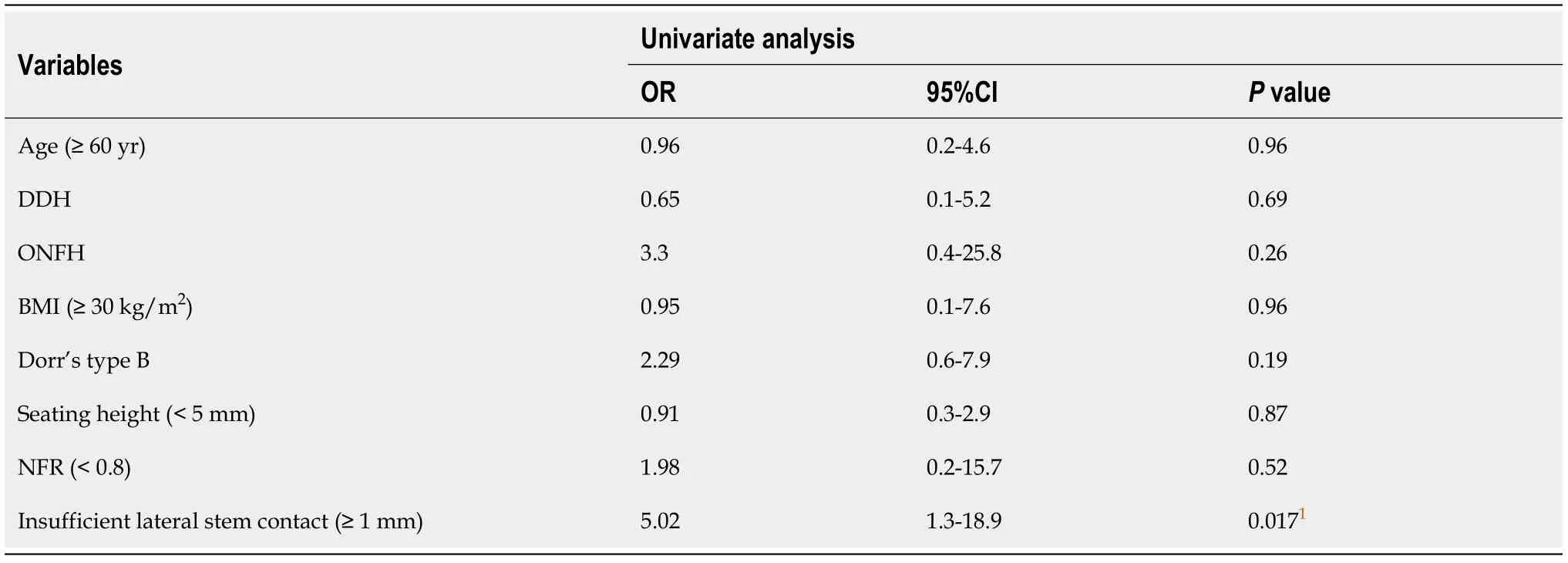
Twelve hips (4.4%) had significant subsidence (> 3 mm) with the mean of 6.7 mm. (3.21-12.7),including 7 cases of Dorr’s type A and 5 cases of Dorr’s type B, 11 cases of ONFH and 1 case of DDH.The univariate regression analysis demonstrated that age, diagnosis, BMI, Dorr’s type B, NFR, and seating height had no significant influence on significant subsidence, whereas insufficient lateral stem contact did have a statistically significant influence [Odds ratio (OR) = 5.02; 95%CI: 1.3-18.9; P = 0.017](Table 4). The multivariate regression analysis also demonstrated that insufficient lateral stem contact was a statistically significant influencing factor (OR = 5.5; 95%CI: 1.4-21.4; P = 0.014). The intra-operative calcar crack incidence was 6.6% (18/274) and all were treated with cerclage wire with no further subsidence.
ARTlCLE HlGHLlGHTS
Research background
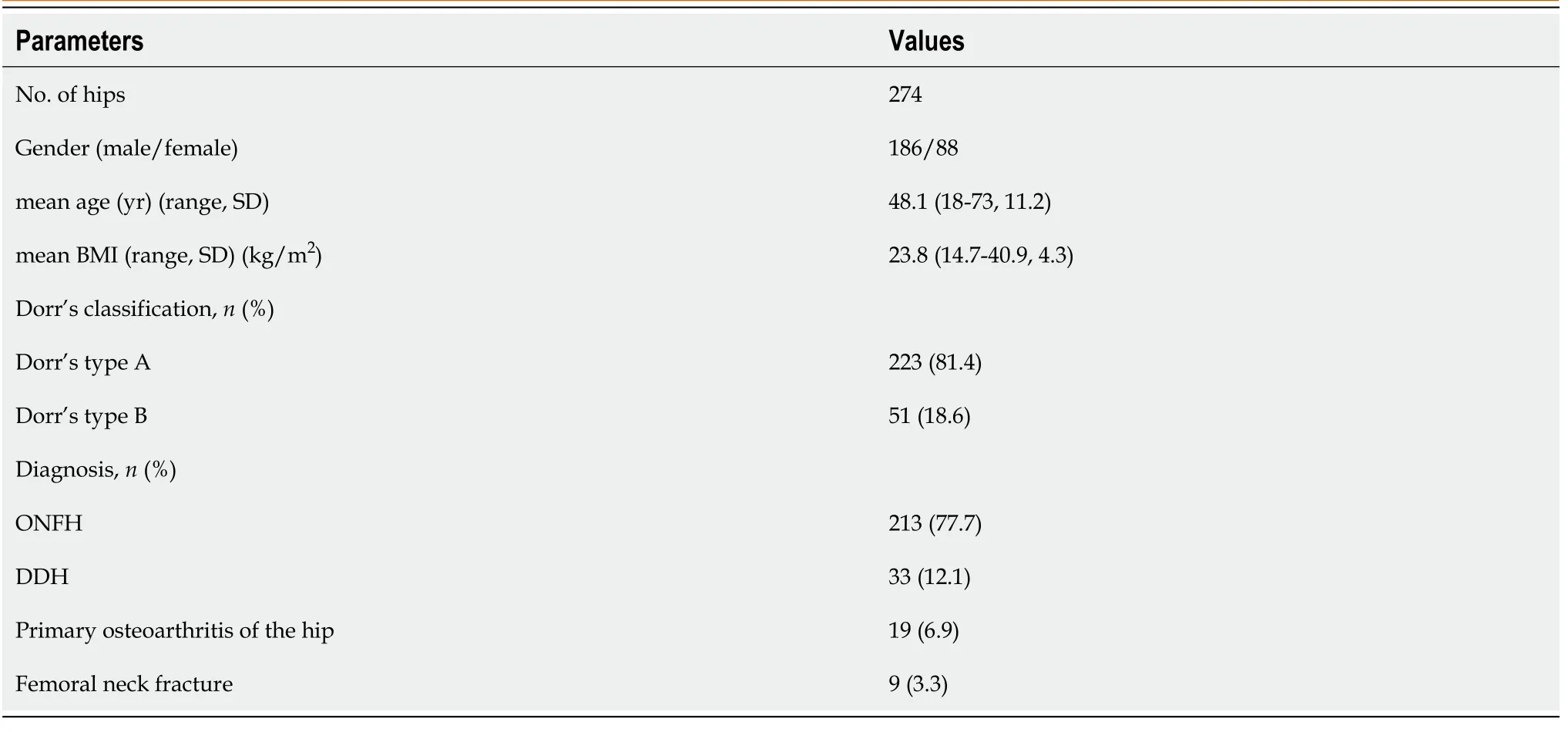
There were 322 Metha stem THAs in the study period, 1 case died 1 year after surgery from a condition unrelated to the arthroplasty, 47 cases were lost before a minimum of two years follow-up, leaving 274 cases which including 186 males (67.9%) and 88 females (32.1%) to study. Their mean age was 48.1 years(range, 18-73 years) with a mean BMI of 23.8 (range, 14.7-40.9). There were 223 cases (81.4%) of Dorr’s type A and 51 cases (18.6%) of type B. The diagnoses included 213 cases (77.7%) of ONFH, 33 cases(12.1%) of DDH, 19 cases (6.9%) of primary osteoarthritis of the hip and 9 cases (3.3%) of femoral neckfractures (Table 2).
Research motivation
Few publications have studied the influencing factors for subsidence in short cementless stems, due to their metaphyseal fitting without diaphyseal anchoring, they might demonstrate different subsidence patterns than with the conventional stems.
Research objectives
This study aimed to analyze the influencing factors with subsidence in short stems.
Research methods
Retrospectively reviewed the digitized radiographs of 274 consecutive short stem total hip arthroplasties. Subsidence, neck-filling ratio, seating height and lateral stem contact were evaluated after a minimum of two years follow-up. A threshold of subsidence > 3 mm was considered a clinically significant subsidence.
Research results
In this study we demonstrated that the insufficient lateral stem contact group (≥ 1 mm) seemed to have higher subsidence than the sufficient lateral stem contact group (< 1 mm) in the entire cohort, but did not reach statistical significance. For significant subsidence cohort, the only significant influencing factor was insufficient lateral stem contact, the univariate and multivariate regression analyses showed statistical significance.
Research conclusions
The Queen was well satisfied with the idea, but the armor-bearer, who had overheard everything, being much attached to his young master, went straight to him and revealed the whole plot. I ll soon put a stop to the business, said the tailor. That night he and his wife went to bed at the usual time; and when she thought he had fallen asleep she got up, opened the door, and then lay down again. The little tailor, who had only pretended to be asleep, began to call out in a clear voice: My lad, make that waistcoat and patch those trousers, or I ll box your ears. I have killed seven at a blow, slain two giants, led a unicorn captive, and caught a wild boar, then why should I be afraid of those men standing outside my door? The men, when they heard the tailor saying these words, were so terrified that they fled as if pursued by a wild army, and didn t dare go near him again. So the little tailor was and remained a king all the days of his life.
Research perspectives
Long term follow-up for this study group will be the next study.
ACKNOWLEDGEMENTS
The authors wish to acknowledge Dr. Urawit Piyapromdee MD, for assisting with the statistical analysis and gratefully thank Mr. Jason Cullen for the careful proofreading of the manuscript.
So when the day approached he put on his invisible belt, took a sack of gold pieces with him, and slipping into her room in the middle of the night, he placed the bag of gold beside her bed and returned to his sheep
FOOTNOTES
All authors contributed to the study conception and design; Suksathien Y, Chuvanichanon P and Tippimanchai T contributed to the material preparation, data collection and performed analysis; Suksathien Y wrote the first draft of the manuscript; and all authors commented on previous versions of the manuscript and read and approved the final manuscript.
This study was Approval by the Institutional Review Board of Maharat Nakhon Ratchasima Hospital, Thailand (Approval No. 046/2021).
Well, the passengers came up and I had to get busy. I didn t look toward2 the stairs again until nearly time for the 9:18 and I was very surprised to see that the young fellow was still there.
All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
The authors have no conflicts of interest to declare that are relevant to the content of this article.
No additional data are available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Thailand
Yingyong Suksathien 0000-0001-8300-9411; Pattawat Chuvanichanon 0000-0002-0836-1826; Thanut Tippimanchai 0000-0002-8532-6995; Jithayut Sueajui 0000-0002-2546-1896.
Wang JL
A
As his car passed, one child appeared, and a brick smashed into the Jag s side door. He slammed on the brakes and spun3 the Jag back to the spot from where the brick had been thrown.
Wang JL
 World Journal of Orthopedics2022年5期
World Journal of Orthopedics2022年5期
- World Journal of Orthopedics的其它文章
- Coronal plane deformity around the knee in the skeletally immature population: A review of principles of evaluation and treatment
- Update in combined musculoskeletal and vascular injuries of the extremities
- Distal femur complex fractures in elderly patients treated with megaprosthesis: Results in a case series of 11 patients
- Prevalence and factors of work-related musculoskeletal disorders among hand surgeons
- What factors are important to new patients when selecting an orthopedic oncologist?
- Anterior vertebral body tethering for idiopathic scoliosis in growing children: A systematic review