
Effect of non-steroidal anti-inflammatory drugs on fracture healing in children: A systematic review
2022-05-30 05:51SarahStroudToshaliKatyalAlexGornitzkyIshaanSwarup
World Journal of Orthopedics 2022年5期
lNTRODUCTlON
Non-steroidal anti-inflammatory drugs (NSAIDs) are among the most commonly prescribed medications in the United States as well as some of the most frequently purchased over-the-counter analgesics. They workinhibition of cyclooxygenase (COX) isoforms, including COX-1 and COX-2, to decrease downstream production of pro-inflammatory prostaglandins and thromboxane, a mediator of thrombogenesis and platelet function. COX-2 is involved in chondrocyte differentiation and is expressed in both osteoblasts and fracture callus[1,2]. Relating to fracture healing, a study of human callus found a thirteen-fold decrease in COX-2 expression in the callus of nonunions as compared to that of healed fractures[3].
As a result of these findings, the effects of NSAIDs on bone healing are an active area of study.Although eight animal studies suggest decreased callus formation and quality in animals exposed to NSAIDs[4-11], other investigations have found no difference in callus quality or healing rates[12-15].One possible explanation for these discordant findings is a lack of standardization of agent, COX enzyme specificity, duration of therapy, and dose. Across the adult fracture nonunion literature,NSAIDs have both been associated with nonunion and found to have no effect on nonunion rates[16-20]. Nevertheless, despite these contradictory findings, a recent survey of orthopaedic surgeons found that 86% believe NSAIDs to be a risk factor for nonunion[21].
Additionally, very little is known about the effects of NSAID use on bone healing in children.Notably, nonunions in pediatric patients are exceedingly rare, with one epidemiological study suggesting that only 1 in 500 pediatric fractures goes on to nonunion[22]. This is an order of magnitude lower than the nonunion rate across all fractures in adults, which is estimated at 1.9%-6.8%[23,24]. The biological underpinnings of this difference in risk are theorized to include a robust periosteum which provides centripetal blood flow, greater innate regenerative potential, ongoing osteogenesis, and increased vascularity with greater fracture hematoma formation[25]. Further supporting their use,evidence has arisen indicating that NSAIDs are equally or more effective for post-fracture pain control than opiates while also leading to fewer side effects[22,26-29]. Reported side effects include bleeding complications due to inhibition of thromboxane formation and gastritis, which are common in adults but rare in children.
Clinically, there is considerable variation in the use of NSAIDs in pediatric fractures, likely due to varying reports in the literature and extrapolation of results from studies in other populations. There have been recent publications focusing on the use of NSAIDs for pediatric fractures and the goal of this systematic review was to assess whether NSAID exposure is a risk factor for fracture nonunion inchildren. In doing so, we hope to clarify the safety profile of NSAIDs in order to optimize their use in standard, multimodal analgesic regimens across pediatric orthopaedic fracture care.
MATERlALS AND METHODS
We performed a computerized search using MEDLINE (PubMed platform), Cochrane Database, and Web of Science. The author (Katyal T) identified and utilized a combination of keywords and MeSH terms for “fracture”, “bone healing”, and “pediatric” patient population. The searches were performed in November 2020. Results were limited by language, English, but not by publication date. We included all English language, full-text articles of human subjects focusing on pediatric patients with fractures,post-fracture NSAID exposure, and control cohorts without NSAID exposure. Outcomes of interest were the reported rates of delayed unions, malunion, growth disturbance, and nonunions. Case reportsand case series with less than 10 patients were excluded. All relevant randomized controlled trials,retrospective reviews, cohort, and case-control studies were included.
Non-steroidal anti-inflammatory drugs (NSAIDs) are among the most commonly prescribed medications in the United States. Although they are safe and effective means of analgesia for children with broken bones, there is considerable variation in their clinical use due to persistent concerns about their potentially adverse effect on fracture healing.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: http://creativecommons.org/Licenses/by-nc/4.0/

RESULTS
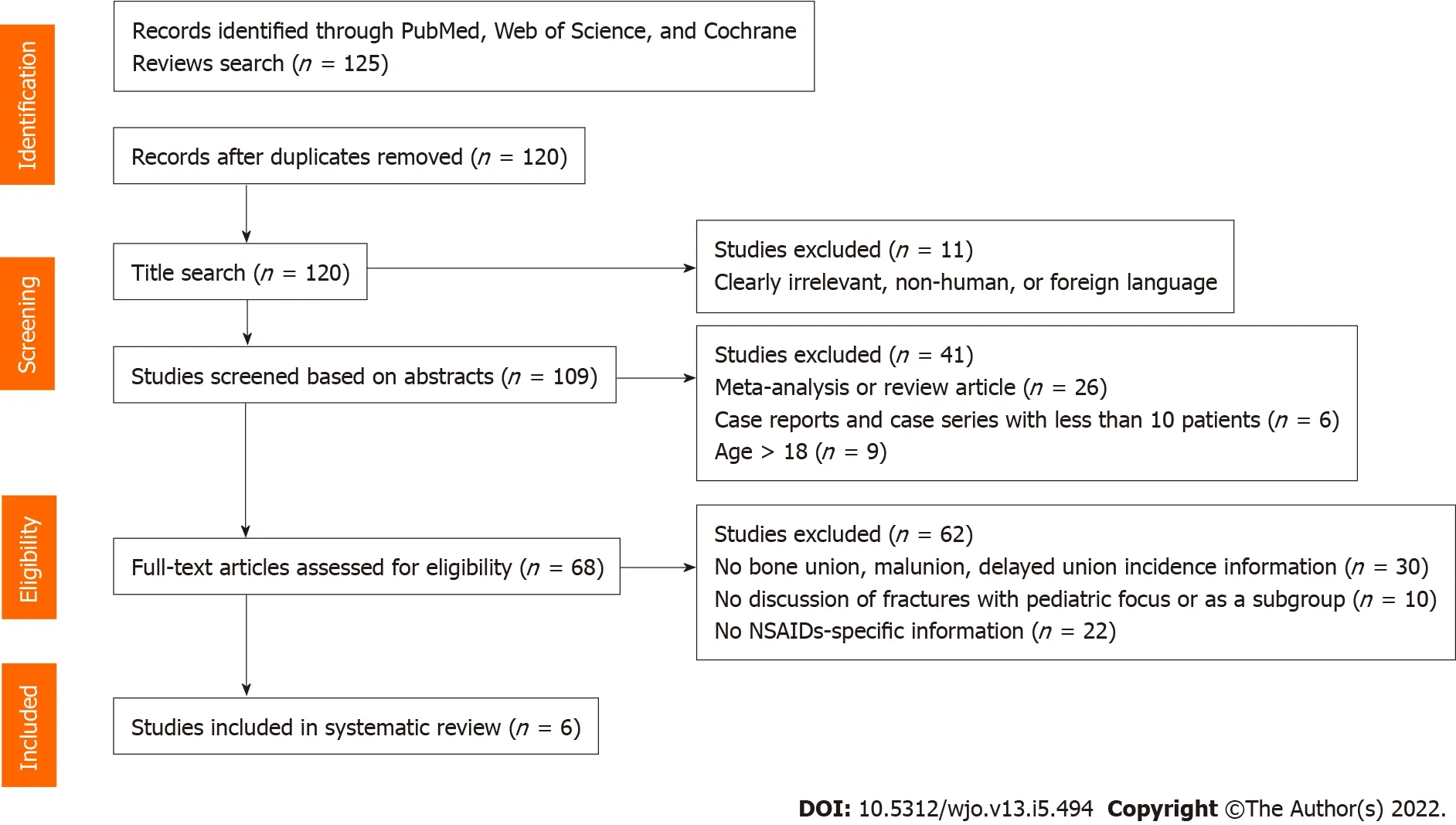
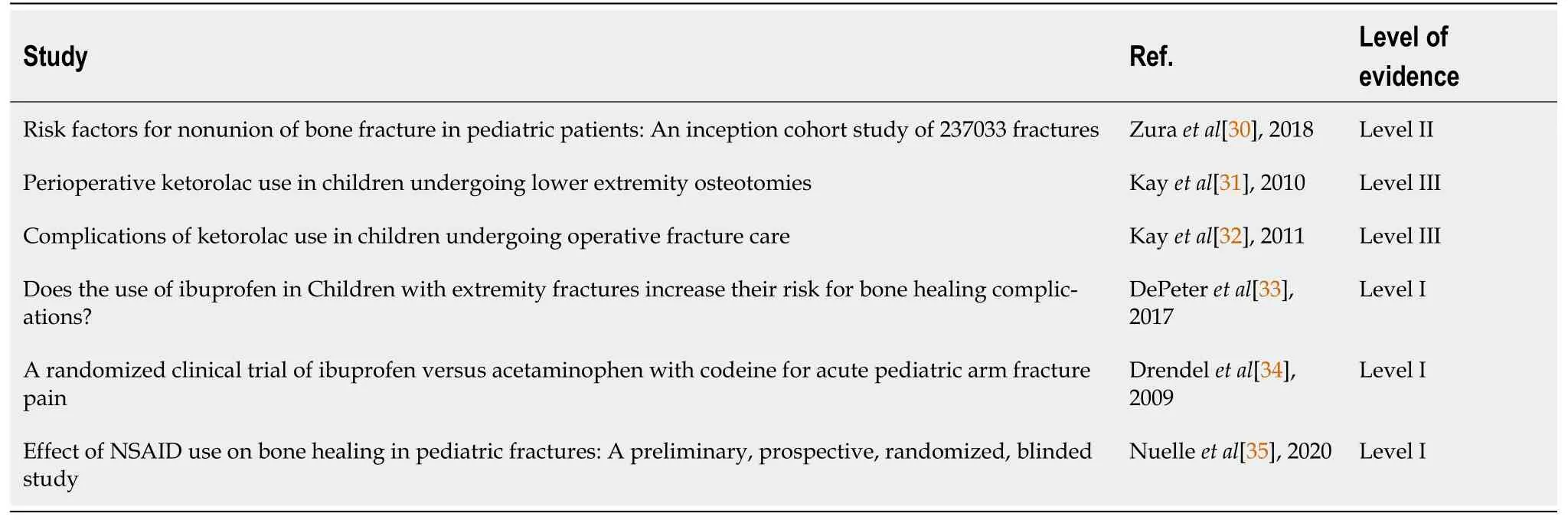
In total, 120 unique articles were identified. As demonstrated in the PRISMA flow diagram (Figure 1),114 articles were excluded from final analysis, including 11 articles after review of titles, 41 studies after screening of abstracts and 62 studies after assessment of full-text articles. Six studies were included for final analysis review (Table 2).
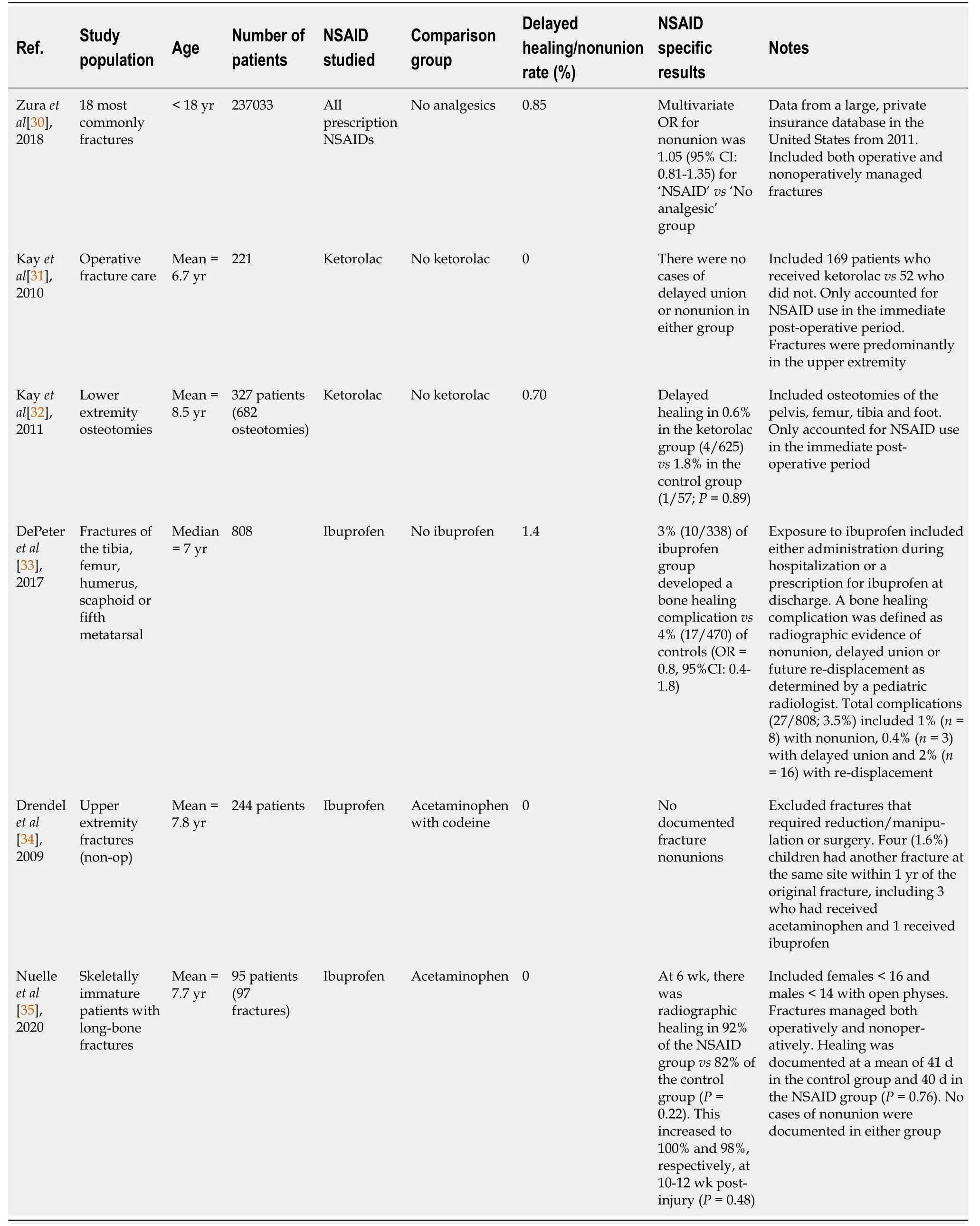
Analyzing an insurance claims database including more than 237000 pediatric fractures, Zura[30]reported a cumulative pediatric nonunion rate of less than 1%, which was 80% lower than adults.Specifically, age was directly related to risk of nonunion, increasing from 0.20% in those 0-6 years old to 0.26% in those 7-11 years and 1.63% in those 12-17 years old. With respect to NSAIDs, the authors found that prescription NSAID use alone did not increase the risk of nonunion [odds ratio (OR) = 1.05; 95%confidence interval (CI): 0.81-1.35; Table 3]. In comparison, the risk of nonunion did increase when NSAIDs were combined with opioids (OR = 2.52; 95%CI: 2.18-2.91), including a more than two-fold increase for those using opioids alone (OR = 2.47; 95%CI: 2.18-2.78)[1].
In a series of retrospective studies looking at NSAID use in children, some studies concluded that routine perioperative ketorolac use after orthopaedic surgery is not associated with an increased risk of delayed bone healing or nonunion[31,32]. This included both routine operative fracture care (0%nonunion rate after ketorolac use)[31] and lower extremity deformity correction[32]. Looking further at the high-risk osteotomy cohort, only 5 out of 682 osteotomies (0.7%) were complicated by delayed union or nonunion, with all 4 delayed unions in the ketorolac group (4/625; 0.6%) going on to heal completely without surgery[32]. Similarly, DePeter[33] retrospectively analyzed all children who presented to their emergency department with a fracture of the tibia, femur, humerus, scaphoid or fifth metatarsal.Comparing those who received ibuprofen to those who did not, the authors found no differences in the rate of nonunion, delayed union or fracture re-displacement on follow-up radiographs, leading them to conclude that ibuprofen administration is not associated with an increased risk for clinically important bone healing complications following traumatic fractures in kids.
There have been two prospective, randomized clinical trials in children looking at fracture healing following ibuprofen administration. First, Drendel[34] reported no instances of nonunion at minimum 1-year follow-up in 244 children managed nonoperatively with either ibuprofen oracetaminophen with codeine for pediatric upper extremity fractures. Of those who did have a refracture at the same site within 1 year of the original injury (= 4; 1.6%), only 1 had received ibuprofen. Finally,Nuelle[35] compared ibuprofen to acetaminophen administration following long-bone fractures in 95 skeletally immature children. Overall, they reported no difference in radiographic healing at 6- or 12-wk post-injury, including 100% healing in the NSAID group by 12 wk post-fracture.
The present review identified six studies that examined the effects of NSAID exposure on nonunion or delayed union in pediatric patients. Among the studies included, there were 2011 nonunions among 238822 fractures (0.84%). Of these studies, three examined the effects of ibuprofen in the acute postfracture period, three studied ketorolac in the same time frame, and one was a database study that did not capture the specific agent or the timing of NSAID exposure. None of the six studies found NSAID exposure to be a risk factor for nonunion or delayed union in children, including a retrospective review that focused on bones with an innately higher risk for nonunion[33]. In contrast, in their large database study, Zura[30] found age (especially over 11 years), bone (scaphoid, femoral neck, tibia or fibula), male sex, higher body mass index, open fracture, or multiple concomitant fractures to be risk factors for pediatric nonunion.
DlSCUSSlON
Overall, the included studies show that nonunion in children is extremely rare, and no published study to date has documented an increased risk of nonunion or delayed bone healing in those children who are treated with NSAIDs in the immediate post-injury or peri-operative time period.
Once I digested this insight my feelings changed from those of a needy19 child to ones of a very proud daughter. Looking at my father more objectively allowed me to view him clearly: he was a man of few words; he was intelligent, kind and extremely modest. Ironically I began to feel closer to him in death than I had while he was alive.
When she says to the goat in the field, Little goat, bleat, Little table, appear, a table stands before her, spread with the best food, much better than we have; and when she has had enough, she says, Little goat, bleat, Little table, away, and everything disappears again
Despite these limitations, however, it is still possible to draw several meaningful conclusions. First,nonunion in children is extremely rare across most age groups and fracture types, including those deemed ‘high risk’. Second, at standard doses in the acute post-injury/surgery period, both ibuprofen and ketorolac do not appear to be associated with an increased risk for nonunion or delayed union in pediatric patients. These findings are specific to upper extremity and long bone fractures. Moreover,children are likely to take these medications for only a few days after injury, another factor which decreases their exposure to any potential deleterious effects on osteogenesis. For example, Nuelle[35] reported that ibuprofen was used for only 4 d on average in their prospective cohort.
CONCLUSlON
Finally, NSAIDs are safe in children and are associated with a decreased risk of adverse effects and equivalent analgesia to opioid-containing agents. Taken together, this systematic review suggests that NSAIDS can be safely prescribed to pediatric orthopaedic patients absent other contraindications without concern for increased risk of fracture non-union or delayed healing. Additional prospective studies are needed focusing on higher risk fractures and elective orthopaedic procedures such as osteotomies and spinal fusion.
Of note, most of the included studies have methodological limitations. First, Zura[30] did not capture whether NSAID exposure was acute or chronic and was focused only on a specific cohort whose parents had employer-supplied health insurance, which may not be generalizable to all patients. Next,while two of the three retrospective reviews were able to report a standardized dose of ketorolac, the third did not. Additionally, none of the three were able to control for concomitant opioid use or medications that may have been purchased over the counter and administered by parents after discharge[31-33]. In one of the two randomized controlled trials, each experimental group was sent home with both drugs and instructed to take the other group’s medication if they experienced breakthrough pain, thus making it difficult to exclude potential cross-over effect[34]. Third, none of the included studies examined COX-2 specific inhibitors or the effects of longer-term NSAID exposure on pediatric nonunion risk. For this reason, conclusions are limited to ibuprofen and ketorolac use in the acute period. Finally, nonunion in children is very rare, and many of the included studies reported zero nonunions, thus suggesting an overall limitation in study power.
ARTlCLE HlGHLlGHTS
Research background
Each title from the performed search was assessed for inclusion based on the specified criteria described above (Figure 1). The relevant abstracts were then independently reviewed by two authors(Katyal T and Stroud S) for inclusion, and if there was any doubt regarding the relevance and applicability, the full-text article was obtained. Full-text articles of the selected abstracts were then appraised by two authors (Katyal T and Stroud S) for inclusion in the systematic review. Any conflicts in screening were resolved by a third author (Gornitzky AL). Two authors (Stroud S and Gornitzky AL) then independently extracted relevant data including age, number of patients in sample size, NSAID class,comparison group, rate of delayed healing and/or nonunion rate, results specific to NSAID type, and details concerning duration of exposure, length of follow-up, and definition of delayed union or nonunion. Study quality was assessed independently using the Newcastle-Ottawa scale (NOS) for the nonrandomized studies from the final list of articles (Table 1). Nonrandomized studies with an NOS score of five or greater on the nine-point scale were included.
Research motivation
The goal of this systematic review was to assess whether NSAID exposure is a risk factor for fracture nonunion in children.
Research objectives
The goal of this systematic review was to assess whether NSAID exposure is a risk factor for fracture nonunion in children.
From a clinical perspective, NSAID exposure is not associated with increased risk of bleeding, blood transfusions, or wound complications[31,32,35]. Specifically, of the six studies included, four did not examine the rate of wound complications and the two studies that did found no difference between the NSAID and non-NSAID groups[31,32]. In fact, NSAIDs are associated with both a lower risk of adverse effects and a lower rate of functional impairment[34]. Furthermore, NSAIDs are safe, cheap and effective opioid-sparing analgesics[22,26,27,34]. Unfortunately, due in part to persistent concerns regarding delayed fracture healing, they are a frequently underutilized medication[36].
Research methods
We systematically reviewed the literature reporting the effect of NSAIDs on bone healing. We included all clinical studies that reported on adverse bone healing complications in children with respect to NSAID exposure. The outcomes of interest were delayed union or nonunion. Study quality was assessed using the Newcastle-Ottawa scale for non-randomized studies. A final table was constructed summarizing the available evidence.
Research results
A total of 120 articles were identified and screened, of which 6 articles were included for final review.Nonunion in children is extremely rare; among the studies included, there were 2011 nonunions among 238822 fractures (0.84%). None of the included studies documented an increased risk of nonunion or delayed bone healing in those children who are treated with NSAIDs in the immediate post-injury or peri-operative time period. Additionally, children are likely to take these medications for only a few days after injury or surgery, further decreasing their risk of adverse side-effects.
In the final examination19, four of us got the scholarship (7 in all). To be honest, I should have been proud of them, but not, because I didn t get it because of the bad train scores. In this aspect I am selfish. At the same time it s a motivation for me to work hard. The atmosphere of studying in our dormitory is good, and we encourage each other! This is a very positive aspect. And negative one, maybe there is no. So I consider our dormitory() perfect.
Research conclusions
This systematic review suggests that NSAIDS can be safely prescribed to pediatric orthopaedic patients absent other contraindications without concern for increased risk of fracture non-union or delayed bone healing. Additional prospective studies are needed focusing on higher risk fractures and elective orthopaedic procedures such as osteotomies and spinal fusion.
If he loves me truly, she used to say, what use would life be to him then? At the same time she was willing to do the same, and if he died first to be buried with him
Research perspectives
Additional prospective studies are needed focusing on higher risk fractures and elective orthopaedic procedures such as osteotomies and spinal fusion.
FOOTNOTES
Katyal T performed the literature search for the systematic review; Stroud S and Katyal T reviewed the articles using the inclusion and exclusion criteria; Stroud S, Katyal T, and Gornitzky AL collected and analyzed the data and wrote the paper; Swarup I supervised and contributed to the report.
The authors have no conflicts to disclose.
Then all too soon the garden was harvested, the vegetables canned and stored, and the school reopened. Soon the leaves fell and the winds blew cold and gusty12 from the bay. Reuben wandered the streets, diligently13 searching for his hessian() treasures.
The authors have read the PRISMA 2009 Checklist, and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Then a servant fetched in the polluted, blue-eyed headsman, who asked: Whose sun of life has come near its setting? took the prince by the arm, placed him upon the cloth of execution, and then, all merciless and stony52 hearted, cut his head from his body and hung it on the battlements
United States
Sarah Stroud 0000-0003-3791-6816; Toshali Katyal 0000-0003-2200-681X; Alex L Gornitzky 0000-0003-0391-6017; Ishaan Swarup 0000-0003-3481-3408.
After a minute she backed away and pointed very stiffly15 toward the north end of the station. Harry, for three years, for three solid years, I ve been right over there working right in this very station, typing, in the office of the stationmaster. ,,。“,3,3,——,,。”
Pediatric Spine Study Group (PSSG); CORTICES;International Perthes Study Group (IPSG); SCFE Longitudinal International Prospective Registry (SLIP); Pediatric Orthopaedic Society of North America (POSNA); American Orthopaedic Association (AOA) Emerging Leaders Program; American Academy for Cerebral Palsy and Developmental Medicine; American Academy of Orthopaedic Surgeons (AAOS); Alpha Omega Alpha Medical Honor Society (AOA).
Wang JJ
I can quench8 my thirst without you, and bending over the well he lapped up the water so greedily that he plunged9 his face, beard and all, right into the crystal mirror
A
Then he went with her, and inside the castle was a large hall with a marble floor, and there were heaps of servants who threw open the great doors, and the walls were covered with beautiful tapestry8, and in the apartments were gilded9 chairs and tables, and crystal chandeliers hung from the ceiling, and all the rooms were beautifully carpeted
Wang JJ
 World Journal of Orthopedics2022年5期
World Journal of Orthopedics2022年5期
- World Journal of Orthopedics的其它文章
- Coronal plane deformity around the knee in the skeletally immature population: A review of principles of evaluation and treatment
- Update in combined musculoskeletal and vascular injuries of the extremities
- lnsufficient lateral stem contact is an influencing factor for significant subsidence in cementless short stem total hip arthroplasty
- Distal femur complex fractures in elderly patients treated with megaprosthesis: Results in a case series of 11 patients
- Prevalence and factors of work-related musculoskeletal disorders among hand surgeons
- What factors are important to new patients when selecting an orthopedic oncologist?