
Plate vs reverse shoulder arthroplasty for proximal humeral fractures:The psychological health influence the choice of device?
2022-04-06 01:31:34GiuseppeMaccagnanoGiuseppeSolarinoVitoPesceGiovanniVicentiMicheleCovielloVittorioSaverioNappiOrazioValerioGiannicoAngelaNotarnicolaBiagioMoretti
World Journal of Orthopedics 2022年3期
INTRODUCTION
Proximal humeral fractures account for 6%-8% of all fractures and around 85% occurs in patients over 50 years old[1].Most patients sustaining these fractures are women above the age of 60.These fractures represent the third most common observed osteoporotic fracture in elderly patients,after wrist and hip fractures[2-4],with an incidence of 82 per 100000 person-years.It has been suggested that the overall fracture rate is increasing along with the increase in the elderly population[5,6].Furthermore,a Finnish study estimated the incidence of fall-related proximal humerus fractures has tripled since 1970[7].The Neer classification,based on the number of bone fragments,is used for the therapeutic decision[8].This remains the most commonly used classification,but additional systems have been described more recently,giving other useful indications to surgeon for type of surgery to adopt.About 80% of the proximal humeral fractures is nondisplaced or minimally displaced,therefore in these cases the treatment is conservative.In the remaining 20% of cases,the surgical strategy probably is the first option,although conservative treatment is chosen by some surgeons[9].In relation to different factors,such as age,daily activity,and fracture pattern,operative treatment options include:synthesis and joint replacement[10-13].Many studies compared the clinical and radiological outcomes of three and fourpart proximal humeral fractures in patients over 65 years old treated with open reduction and internal fixation(O.R.I.F.)and joint replacement.Giardella[14],in their retrospective study enrolling patients over 65 years old,reported better clinical and functional results in patients treated with reverse shoulder arthroplasty(R.S.A.)respect to O.R.I.F,confirming that R.S.A.is the best treatment in proximal humeral fractures in elderly patients,especially in case of a rotator cuff tear or degeneration.
The aim of our study was to compare O.R.I.F.with R.S.A.in terms of clinical and psychological outcomes of three- and four-part proximal humeral fractures in patients older than 65 years evaluating whether post-operative psychological symptoms may influence the clinical results after surgery.
MATERIALS AND METHODS
The Authors conducted a prospective observational study with a sequential recruitment of subjects affected by proximal humeral fractures,which was approved by the local Ethics Committee(No.6809).The study was also registered on ClinicalTrials.gov,Protocol Registration and Result System(NCT04821180).
When Sonali came home from school, I let her play for an hour before I told her the news. I wanted to savor8 the innocence9 of her not knowing Daddy was dead. When she heard Alan s plane had crashed and he was not coming home, she wailed10 a cry so deep and heartbreaking, a cry I pray I will never hear again from any living being. She sobbed11 for an hour straight, and then she looked me in the eyes and said, I am so sad. But I m not the saddest girl in the world. Some children have lost their mommy and their daddy, and I still have you.
At the University Hospital of Bari,63 patients who had undergone shoulder surgery between January 2016 and January 2019 were enrolled.
The inclusion criterion for enrollment was:(1)three and four-part proximal humeral fractures according to Neer classification system;(2)patients seventy years or older;and(3)shoulder surgery within one week after trauma.
The exclusion criteria were:(1)exposed fractures;(2)pathological fractures;(3)proximal humerus fractures with metaphyseal or diaphyseal extension;(4)contraindications to surgery associated with organ dysfunctions or with coagulopathy,allergy or hypersensitivity to the orthopedic implants;(5)patients who were unable to attend the different follow-ups;and(6)patients with psychiatric disorders.
The type of treatment was due to rotator cuff status,and shoulder clinical history.
The room was only 13 square meters with two nails on the wall next to the door, one for her to hang her bag and the other for hanging umbrellas. At that time, she threw all her stuff such as her bag and umbrella on the floor once she entered the room, staring at the whole mess and feeling terribly upset.
All patients were properly informed of the nature of the study and they signed an informed consent document according to the Declaration of Helsinki.
The study group was stratified according to age class(class 1:70-74 years;class 2:75-79 years;class 3:80-85 years)and gender differences(Table 1).
After Fred Astaire’s first screen test, the memo1 from the testing director of MGM, dated 1933, said, “can’t act! Slightly Bald! Can dance a little!” Astaire kept that memo over the fireplace in his Beverly Hills home.

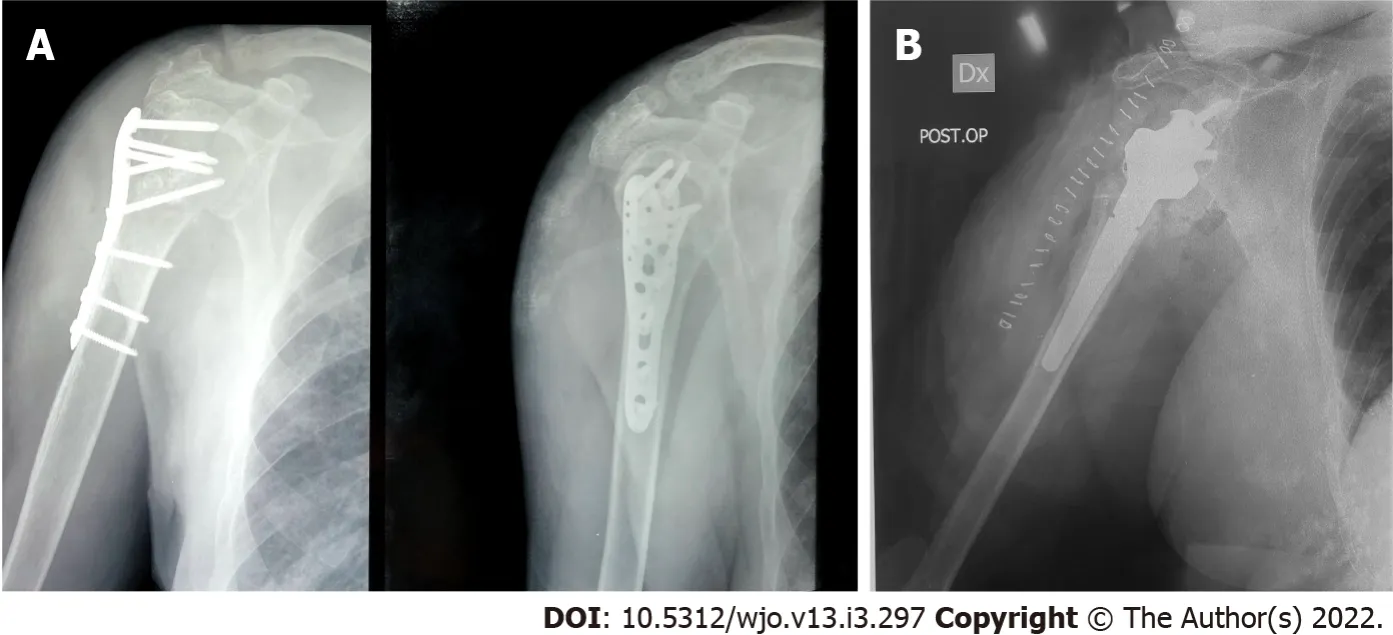
All patients were then divided into two groups according to the choice of surgery treatment:Group A:O.R.I.F.by angle-stable plate PHILOS(PHLPSYNTHES,Oberdorf,Switzerland)(Figure 1A);and Group B:reverse total shoulder arthroplasty by Modular Shoulder Replacement SMR(LIMACorporate,San Benedetto del Friuli,Italy)(Figure 1B).
All patients were treated by the same surgical team with more than five years of experience in upper limb surgery.
We assumed that all enrolled patients suffered cuff tear arthropathy based on biological and anagraphic age.
We introduced a control group(Group C),made up of patients with the same characteristics of the study groups,but treated conservatively.
One independent observer performed clinical[Constant score and Disabilities of the Arm,Shoulder and Hand(DASH)score[15,16]]evaluation at one-month(T0),six months(T1)and at one year(T2)post operatively for each groups.
Furthermore the Clinical Psychology Service of our University Hospital performed a psychological evaluation(General Anxiety Disorder-7 scale and Caregiver Strain scale[17,18])at the same follow-ups for each groups.
The Constant score determines the shoulder functionality and a higher score is indicative of high functional outcomes.The DASH score analyzes individual ability to perform certain activities and a higher score is indicative of worse functional outcomes.
The General Anxiety disorder 7 scale and the Caregiver Strain scale are two screening psychological tools used to define the level of stress.A higher score is indicative of poor outcomes.
In each case we evaluated the antero-posterior,lateral and transthoracic humerus X-rays at the T0,T1 and T2.
Statistical analysis
All data were collected electronically and were analyzed using R version 3.5.2(released on 2018-12-20).In order to account for non-normality(Shapiro-Wilk test),continuous variables were reported as median and interquartile range(IQR)and compared(univariable analysis)through Wilcoxon rank sum test.Categorical variables were reported as absolute and relative frequencies.A multivariable linear regression model was then fitted for each score and time in order to evaluate the effect of PI intervention compared to O.R.I.F.intervention(“beta” coefficients)adjusted for age and sex.Linearity of dependent variable and normality and homoscedasticity of residuals were checked for each model through a test of significance.Statistical significance “alpha” was fixed to 0.05.The primary endpoint examined was psychological outcomes of proximal humeral fractures using General Anxiety disorder 7 scale.The secondary endpoint was clinical and shoulder functionality using Constant score.In addition,the Caregiver Strain scale and DASH score were used to complete psychological and clinical outcomes.
Near his house stood the ancient barn that housed the family s goats and chickens. Reuben found a rusty6 soda7 tin and dropped his coins inside. Then he climbed into the loft8 of the barn and hid the tin beneath a pile of sweet smelling hay.
RESULTS
The study group was made up of sixty-three patients,5 males(7.9%)and 58 females(92.1%).Theaverage age was 76.0(4.0)years,range 70-82.Median(IQR)age was 76.0(4.0)years.
In 70% of cases the right limb was involved and in 65.1% of cases(41 of 63 cases)were three-part proximal humeral fractures(Table 2).
The analysis showed a prevalence of the four-part proximal humeral fracture in the class 3 age group whilst the three-part proximal humeral fracture in the class 2(Table 3).
Domestic accident was responsible for 70% of cases whilst road traffic accident was the commonest mechanism in 30% of cases.
Based on the results obtained,we highlighted the best results for group A in terms of psychological results respect to group B.
For the group A,the average values at T0 were:DASH score 50.8(range 44-62),Constant score 36.1(range 22-49)(Table 4);as regards the psychological test,the average values at T0 were:General Anxiety Disorder-7 scale 5.4(range 2-9),Caregiver Strain Scale 5.0(range 2-9)(Table 4).
For the group B,the average values at T0 were:DASH score 54.6(range 28-65),Constant score 32.0(range 23-53)(Table 4);as regards the psychological test,the average values at T0 were:General Anxiety Disorder-7 scale 6.4(range 3-9),Caregiver Strain Scale 6.2(range 2-9)(Table 4).
For the group A,the average values at T1 were:DASH score 42.1(range 32-58),Constant score 47.3(range 25-63)(Table 5);as regards the psychological test,the average values at T1 were:General Anxiety Disorder-7 scale 4.3(range 1-8),Caregiver Strain Scale 3.9(range 1-8)(Table 5).
Several days later, when Jenny s father came in to read her a story, Jenny was sitting on her bed and her lip was trembling. Here, Daddy, she said, and held out her hand. She opened it and her beloved pearl necklace was inside. She let it slip into her father s hand.
For the group B,the average values at T1 were:DASH score 39.1(range 21-60),Constant score 43.2(range 28-65)(Table 5);as regards the psychological test,the average values at T1 were:General Anxiety Disorder-7 scale 5.7(range 3-9),Caregiver Strain Scale 5.5(range 2-9)(Table 5).
2. Using a snappish() tone. I have a very short fuse(,) and become irritable4 extremely easily – but my husband really doesn’t like it when I snap at() him (big surprise). I’ve done a lot to try to keep my temper in check. I don’t let myself get too hungry or too cold (I fall into these states very easily); I try to keep our apartment in reasonable order, because a mess makes me crabby(); when he tries to make a joke out of my temper, I try to laugh along; I try to control my voice to keep it light and cheery(,) instead of accusatory(,) and impatient. Confession5: I haven’t made much headway(,) here.
At T2 in the group A,the mean values were:DASH score 32.8(range 16-60),Constant score 60.0(range 30-80)(Table 6);as regards the psychological test,the average values at T2 were:General Anxiety Disorder-7 scale 3.2(range 1-7),Caregiver Strain Scale 3.1(range 1-7)(Table 6).
At T2 the group B shown these mean values:DASH score 33.6(range 17-55),Constant score 52.9(range 35-79)(Table 6);as regards the psychological test,the average values at T2 were General Anxiety Disorder-7 scale 4.3(range 1-7),Caregiver Strain Scale 4.5(range 1-8)(Table 6).





At T0 median(IQR)DASH score was 53.0(11.0),Constant score was 34.0(10.5),General Anxiety Disorder-7 scale was 6.0(2.0)and Caregiver Strain Scale was 6.0(3.0).
At T1 median(IQR)DASH score was 38.0(12.0),Constant score was 44.0(11.5),General Anxiety Disorder-7 scale was 5.0(2.5)and Caregiver Strain Scale was 5.0(3.0).
At T2 median(IQR)DASH score was 32.0(13.5),Constant score was 55.0(20.0),General Anxiety Disorder-7 scale was 4.0(2.5)and Caregiver Strain Scale was 4.0(3.0).
For the group C,the mean values are reported separately(Table 7).
The univariable analysis(Table 8)showed a significant difference between the two treatment groups for Dash score at T0(O.R.I.F.PI,median 50.057.5,= 0.002),Constant at T0(O.R.I.F.PI,median 38.031.5,= 0.008),GAD-7 at T0(O.R.I.F.PI,median 5.06.0,= 0.015),CSS at T0(O.R.I.F.PI,median 5.06.5,= 0.008),GAD-7 at T1(O.R.I.F.PI,median 4.06.0,= 0.002),CSS at T1(O.R.I.F.PI,median 4.06.0,= 0.001),Constant at T2(O.R.I.F.PI,median 60.051.0,= 0.049),GAD-7 at T2(O.R.I.F.PI,median 3.04.0,= 0.012)and CSS at T2(O.R.I.F.PI,median 3.04.0,=0.005).
As pointed out by the Authors,it is very important to perform a psychological analysis of each patient,in order to identify correctly the patient and to reserve the shoulder arthroplasty for a very limit case in which the bone stock is very poor.
We did not observe complications in the study and control group.
DISCUSSION
Three- and four-part fractures account for 21% to 23% of proximal humerus fractures[19,20],are usually treated surgically by O.R.I.F.in younger patients and by arthroplasty in the elderly[21,22].
Many risk factors patient-related such as osteoporosis,degenerative joint disease of the shoulder,rotator cuff dysfunctions,comorbidities and non-modified risk factors such as gender and age class may influence the choice of treatment[23,24].
In accordance with the literature,we reported a gender differences and age class stratification in favor of female and first class which was most represented(Table 1,Table 3)[25,26].
Due to the poor outcomes associated with conventional anatomic replacement of the humeral head,an extended use of the reverse shoulder arthroplasty has emerged in the literature,linked to good results as both a primary procedure and as a secondary procedure for failed open reductions[27-29].
Until now all the studies described in the literature comparing open reduction and osteosynthesis with reverse shoulder arthroplasty as surgical options of treatment for three and four-part proximal humeral fractures in patients over 65 years old,used clinical and radiological methods of evaluation[30-33].
Our study is the first in literature that compares the psychological and functional results in order to underline the importance of each one or both for the pre-operative planning.
According to the literature,the functional results of the two surgical options(O.R.I.F.reverse prosthesis)overlapped at 1 year post operatively[34].
The univariable analysis(Table 8)showed a significant difference between the two treatment groups in favor of Group A as regards DASH score at T0(O.R.I.F.PI,median 50.057.5,= 0.002)and Constant at T0(O.R.I.F.PI,median 38.031.5,= 0.008).
The Authors linked these results to reach more confidence with the plate respect to the prosthesis.Furthermore,we did not report any statistically significance difference between the two groups at T1(= 0.256;= 0.110).
The univariable analysis(Table 8)did not show a statistically significant difference between the two treatment groups for DASH score at T2(O.R.I.F.PI,median 30.032.0,= 0.587);as regard the Constant score at T2(O.R.I.F.PI,median 60.051.0,= 0.049),there emerged a statistically significant difference in favor of group A who obtained better results but these were very near to the significance limit.
In our study,the Authors reported a tendency to the improvement of functional outcomes for the two groups.As regards the DASH and the Constant score,the Authors reported good results in both groups from T0 to T2 by analyzing the average value of Table 4,Table 5,and Table 6.
55.Forgot:Cinderella breaks her promise to leave the ball before midnight since she is busy with the prince. While forgetfulness is understandable, she does break her promise and is given a small element of humanity. The forgotten time also provides drama, causing Cinderella to run away and leave behind her shoe, providing the means for her identification later. The imagery of Cinderella s elegant clothes transforming back to rags as she runs home is a favorite scene for illustrators and filmmakers.Return to place in story.
As regards the psychological evaluation,the Authors observed a tendency to the improvement for both groups from T0 to T2 according to Table 4,Table 5,and Table 6.
By better analysis,the Authors highlighted an improvement of psychological evaluation for the group A at T0.
Analyzing GAD-7 at T0(O.R.I.F.PI,median 5.06.0,= 0.015)and CSS at T0(O.R.I.F.PI,median 5.06.5,= 0.008),the Authors reported the superiority in terms of results for the group A respect to the group B according to Table 8.
The statistical evaluation was significant for both tests in the group A and also at T1 and at T2 as reported in the Table 8 analyzing GAD-7 at T1(O.R.I.F.PI,median 4.06.0,= 0.002),CSS at T1(O.R.I.F.PI,median 4.06.0,= 0.001),GAD-7 at T2(O.R.I.F.PI,median 3.04.0,= 0.012)and CSS at T2(O.R.I.F.PI,median 3.04.0,= 0.005).



Patients underwent primary reverse shoulder arthroplasty(group B)showed in each postoperative follow-ups a generalized anxiety disorder and a greater irritability then patients underwent osteosynthesis(group A).
We revealed a residual fear during shoulder movement in patients underwent primary reverse shoulder arthroplasty,unlike the group of patients which have done osteosynthesis,who seemed more confident and secure in shoulder movements.
The authors linked these results for group B to the anxiety about loosening of humeral head.In fact,the patients underwent osteosynthesis,showed better results in terms of anxiety due to the idea to preserve their humeral head.The perception of own humeral head could play a role in the genesis of anxiety.
Moreover,the comparison between the surgical(group A and B)and the conservative group(group C)revealed better clinical and functional results at 12 mo for the group C.In fact,with mean values of 3.1 and 3.0 for the GAD-7 and CSS scales respectively,the group C showed less anxiety and fear at T2 notwithstanding at 12 mo no statistically differences were found.These results are consistent with a previous study that underlined the importance of conservative treatment which remains a valid option mainly in the three-part proximal humeral fractures in selected cases with good functional results and low complications[9].
This study has some limitations:the number of participants is limited to 63;the maximum follow-up achieved was 12 mo;the device for open reduction and internal fixation used was a single type of angle stable plate with specific surgical technique.
Many voices joined in, and a hymn34 of praise was sung; then he heard the priest again, and heard his own name and that of the princess, and thought that he was being wedded35 to her
CONCLUSION
The aim of our study was to compare open osteosynthesis and reverse shoulder arthroplasty in the three and four-part proximal humeral fractures,in terms of functional and psychological scores at one,six months and at one year follow-ups in order to underline the importance of each one or both of them for the pre-operative planning.
The 48.2%(31)of patients were treated by angle stable plate PHILOS(PHLP-SYNTHES,Oberdorf,Switzerland)with O.R.I.F.(group A)while the 50.8%(32)of patients were treated by reverse total shoulder arthroplasty SMR(LIMACorporate,San Benedetto del Friuli,Italy)(group B).The Control group,32 patients,was treated conservatively.
More studies are needed in literature,to evaluate before surgical choice not only anatomical parameters but also patient psychological profile.
For this reason,we suggest to evaluate before surgical choice not only anatomical parameters but also patient psychological profile,always evaluating the possibility of a hypothetical conservative treatment.
Simon replied that the king of the country had insisted on giving him one of his daughters as a wife, but that he had refused the honour because he was too old and too frail37
The strong point of our study is the type of the study in fact it is a prospective observational comparative study.
Instead,the weak point is the lack of psychological evaluation for each patient enrolled before the surgery.
Due to the pain after the trauma,the Authors did not administer the psychological evaluation because it may be influenced negatively.
According to recent data of bibliography,we confirm the efficacy at 1 year of the osteosynthesis and shoulder arthroplasty in terms of functional evaluation.
Then he would cry, but what nobody knows nobody cares for; so he would cry till he was tired, and then fall asleep; and while we are asleep we can feel neither hunger nor thirst
A second univariable analysis(Table 9)between conservative and surgical treatment(using values of the two treatments)was made to enhance the relevance of the study.We reported no statistical difference at T0 regarding clinical and psychological outcomes.On the contrary,conservative treatment has shown to have better clinical and psychological outcomes,although not statistically significant at T1 and statistically significant at T2.
The storms threwvessel after vessel on the fatal reefs; there were snow-storm andsand-storms; the sand flew up to the houses, blocking the entrances,so that people had to creep up through the chimneys; that wasnothing at all remarkable here
ARTICLE HIGHLIGHTS
Research background
Patient affected by fractures is evaluated only from a surgical point of view.Psychological aspect is very often underestimated.
Research motivation
The stepmother is a convention added by the Grimms in their successive editions of the tale of Hansel and Gretel. The original draft of the story has both the birth mother and father deciding to abandon the children. Return to place in story.
Research objectives
The aim of our study was to compare open reduction and internal fixation with joint replacement in terms of clinical and psychological outcomes of three- and four- part proximal humeral fractures in patients older than 65 years evaluating whether post-operative psychological symptoms may influence the clinical results after surgery.
Research methods
An observational prospective single-center study with 12 mo follow-up was performed with a sequential recruitment of subjects affected by proximal humeral fractures treated with open reduction and internal fixation and joint replacement.A conservative treatment group,as control,was introduced.
Research results
Patients underwent primary reverse shoulder arthroplasty showed in each postoperative follow-ups a generalized anxiety disorder and a greater irritability then patients underwent osteosynthesis.
Research conclusions
Patient psychological profile should be evaluated by the surgeon before surgery for the choice of surgical devices.
Research perspectives
Future investigations are needed to confirm the role of the psychological profile in the field of orthopedic surgical treatment.In addition,long- term analysis needs to clarify if differences in outcomes are really related to the patient’s mental state.
FOOTNOTES
Maccagnano G drafted the manuscript,and assisted with data analysis;Solarino G participated in design and oversight of the study;Pesce V drafted the manuscript,and assisted with data analysis;Vicenti G participated in study design and performed statistical analysis;Nappi VS participated in design of the study,and was involved with data collection;Coviello M was involved with data collection,and assisted with data analysis;Giannico OV participated in study design and performed statistical analysis;Notarnicola A participated in design of the study;Moretti B participated in design and oversight of the study.
The authors conducted a prospective observational study with a sequential recruitment of subjects affected by proximal humeral fractures,which was approved by the local Ethics Committee(No.6809).
However I look and sound, whatever I say and do, and whatever I think and feel at a given moment in time is me. This is authentic1 and represents where I am at that moment in time.
The study was also registered on ClinicalTrials.gov,Protocol Registration and Result System(PRS)(NCT04821180).
All patients were properly informed of the nature of the study and they signed an informed consent document according to the Declaration of Helsinki.
The authors declare that there are no conflicts of interest regarding the publication of this paper.
No additional data are available.
The authors have read the CONSORT 2010 statement,and the manuscript was prepared and revised according to the CONSORT 2010 statement.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Italy
Giuseppe Maccagnano 0000-0002-8596-2422;Giuseppe Solarino 0000-0001-6325-9691;Vito Pesce 0000-0003-1191-7853;Giovanni Vicenti 0000-0002-7412-7990;Michele Coviello 0000-0003-3585-1000;Vittorio Saverio Nappi 0000-0002-8429-9526;Orazio Valerio Giannico 0000-0001-5375-8841;Angela Notarnicola 0000-0002-8941-8336;Biagio Moretti 0000-0002-1234-8616.
Wang JL
A
Wang JL
 World Journal of Orthopedics2022年3期
World Journal of Orthopedics2022年3期
- World Journal of Orthopedics的其它文章
- Impact of enhanced recovery pathways on safety and efficacy of hip and knee arthroplasty:A systematic review and meta-analysis
- Surgical treatment of femoral deformities in polyostotic fibrous dysplasia and McCune-Albright syndrome:A literature review
- Diagnostic role of Xpert-MTB RIF assay in osteoarticular tuberculosis:A retrospective study
- Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws
- Ilizarov bone transport combined with the Masquelet technique for bone defects of various etiologies(preliminary results)
- Accuracy of shoulder joint injections with ultrasound guidance:Confirmed by magnetic resonance arthrography