
Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws
2022-04-06 01:31NadeemLilVipulMakwanaTirthPatelArjavPatel
World Journal of Orthopedics 2022年3期
INTRODUCTION
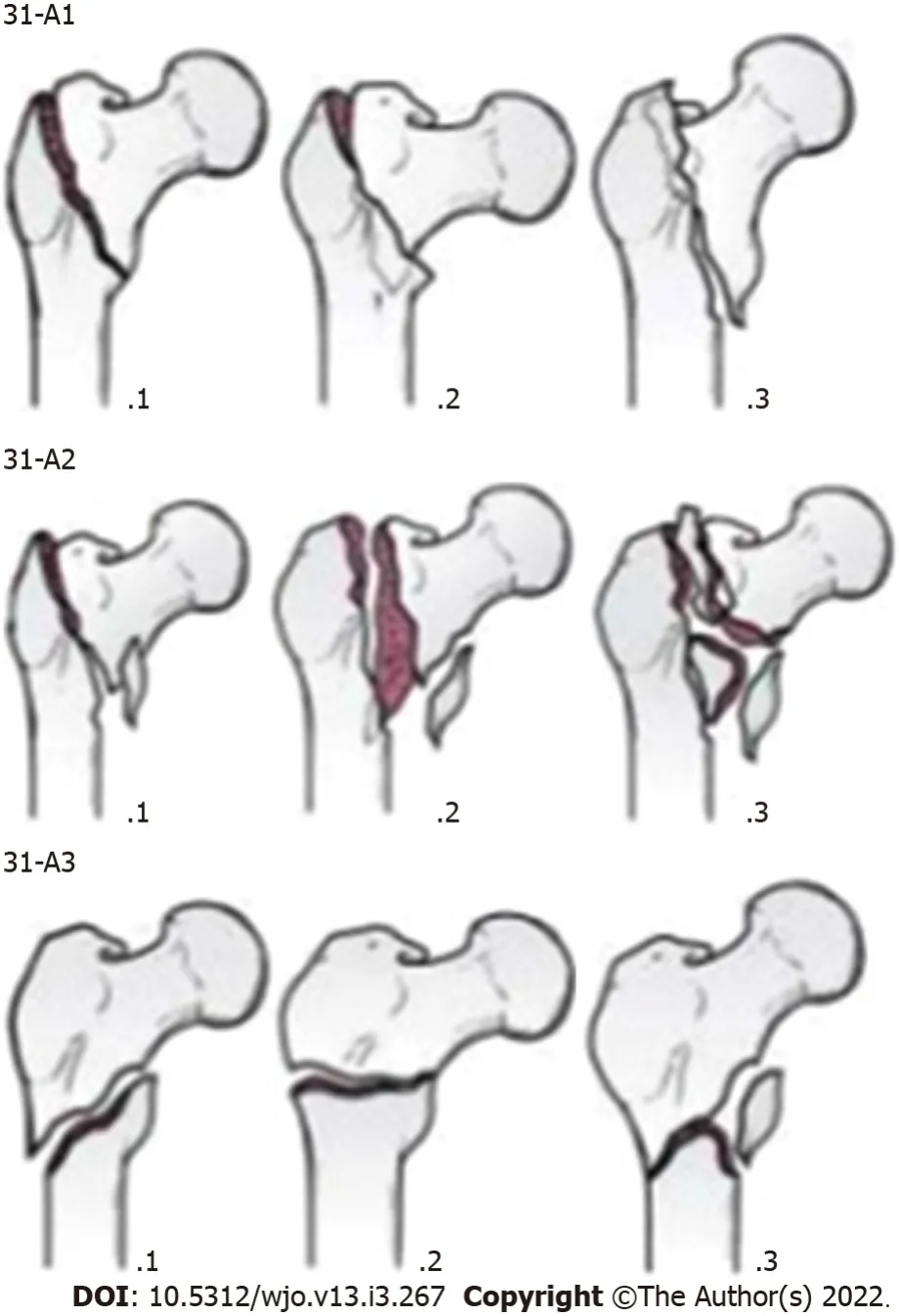
The incidence of fractures in the trochanteric area has risen with the increasing numbers of elderly persons with osteoporosis[1].Intertrochanteric(IT)fracture is one of the most common fractures seen in orthopaedic practices,and proximal femoral nailing(PFN)has become a popular modality for its treatment.As per the Orthopaedic Trauma Association(OTA)classification system,these fractures are classified as Arbeitsgemeinschaft für Osteosynthesefragen(AO)/OTA 31-A and are further subdivided into groups A1,A2 and A3(Figure 1).A1 fractures consist of two-part fractures,A2 fractures have multiple fragments,and A3 fractures include reverse oblique and transverse fracture patterns[2,3].
Then it suddenly dawned on me. God was speaking to me the entire time I was attempting to be still. I remembered the music playing as I d begun my quiet time. He sent a sparrow to lighten my life with song. He sent a gentle breeze. He sent a neighbor to let me know that I had a friend. He sent my sweetheart to offer sincere sentiments of love. He caused my heart to flutter to remind me of life. While I was trying to count my blessings, God was busy multiplying them.

In 1996,for the treatment of unstable per-,intra- and subtrochanteric femur fractures the AO/Association for the Study of Internal Fixation designed the PFN as an intramedullary(IM)device[4].It is routine practice to perform distal interlocking for fracture fixation while using PFN.Distal interlocking screws of the IM nail were made to avoid longitudinal or rotational instability as well as movement of distal tip of nail in cases of a broad canal for the IT fracture[5].Nonetheless,drawback of the distal interlocking screw,like loosening,breaking and subsequent peripheral injures,and secondary femur fractures could not be ignored due to the minimal advantages gained[6].
The purpose of this study was to compare the outcomes of IT fractures(AO/OTA 31-A1 and 31-A2)treated by PFN with and without distal interlocking.We hypothesized that PFN without distal interlocking could be a dependable and acceptable option for IT fractures(AO/OTA 31-A1 and 31-A2).
MATERIALS AND METHODS
We conducted a retrospective study among 140 patients with AO/OTA 31-A1 and 31-A2 fractures treated with PFN at our institute from November 2016 to November 2019.The patients were divided into two equal groups,as follows:70 patients treated with PFN with distal interlocking screws(group 1);and 70 patients treated without distal interlocking screws(group 2).The same chief surgeon performed the operations of all of the patients.
Inclusion criteria included AO/OTA 31-A1 and AO/OTA 31-A2 fracture pattern,age more than 20 years,no other injury or fracture,and those treated with long anatomical design PFN.Exclusion criteria included AO/OTA 31-A3 fracture pattern,age less than 20 years,patients lost to follow-up,patients having surgical site infection,and those treated with short PFN.
In our institute,standard preoperative workup included radiographic evaluation of the fracture type along with blood,medical and anaesthetic assessments.Postoperative protocol included intravenous antibiotics given for 48 h followed by oral antibiotics.On postoperative day 1 of surgery,bedside knee bending,static quadriceps exercises and ankle toe mobilisation exercises were started under supervision of a physical therapist.Regular stitch dressings were completed every third day,and stitches were removed between 12-14 d postoperatively.All patients were sent to the same rehabilitation program.Patients were followed up weekly for the first month after surgery.After that,they received follow-up care every 15 d for the next 2 mo and then monthly follow-up for 14 mo.
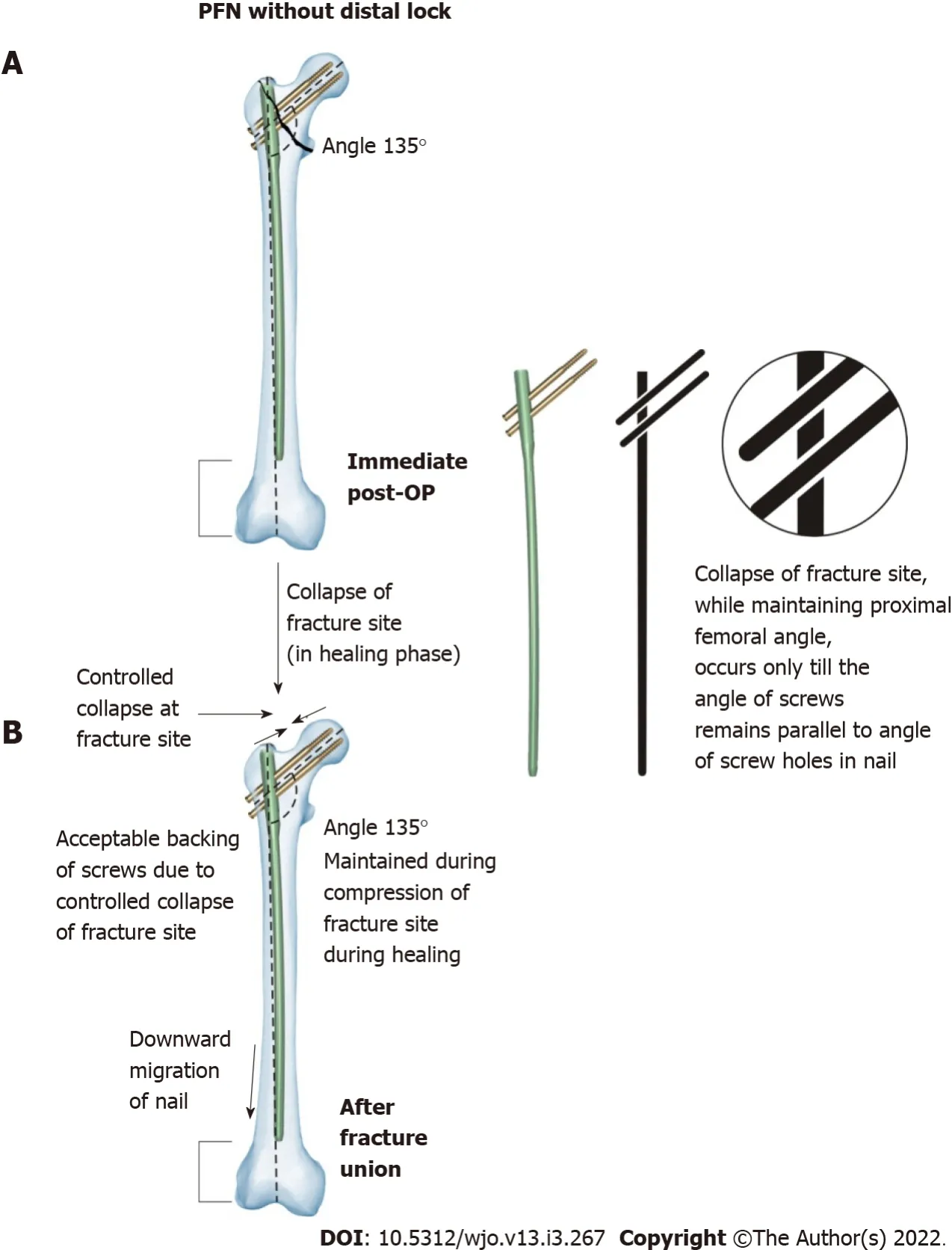
Figure 5 shows a scenario where PFN with distal locking was not performed.It was observed during the postoperative period that the proximal femoral neck shaft angle was maintained.In the healing phase,controlled collapse of the fracture site occurred.During controlled collapse of the fracture site,the proximal neck shaft angle was maintained until the angle of the screws remained parallel to the screw holes in the nail.Parallelism of the screws in the screw holes was maintained due to downward migration of the nail in the canal during the healing phase.Also,there was acceptable backing-out of screws due to collapse of the fracture site.
6.Scrivener: A scrivener is someone employed to make written copies of documents and manuscripts (WordNet). A scrivener would be used to write up the contract and agreement for the division of the inheritance.Return to place in story.
RESULTS
Out of 140 patients,the 70 patients in group 1 were treated with PFN with distal interlocking screws.Among these,24 were male and 46 were female,and 32 patients had AO/OTA 31-A1 fracture pattern and 38 patients had AO/OTA 31-A2 fracture pattern.In group 2,70 patients were treated with PFN without distal interlocking screws.Among these,29 were male and 41 were female,and 28 patients hadAO/OTA 31-A1 fracture pattern and 42 patients had AO/OTA 31-A2 fracture pattern.(Table 1)


Operative time and IITV radiation time
IT femur fractures amount to almost half of total hip fractures caused by a low-energy injury,like a fall from standing height.These fragility hip fractures occur in a population with risk factors including elderly age,female sex,osteoporosis,history of trauma and gait problems[7].IT fractures are not common in young age patients and require investigation;in this population,IT fractures are caused by high-energy injuries or from a pathological process.Thus,secondary injuries or malignancies must be ruled out[8].Surgery is typically the recommended treatment as the morbidity and mortality associated with non-operative treatment has been high historically.Patients often have pre-existing comorbidities that dictate the ultimate outcome.
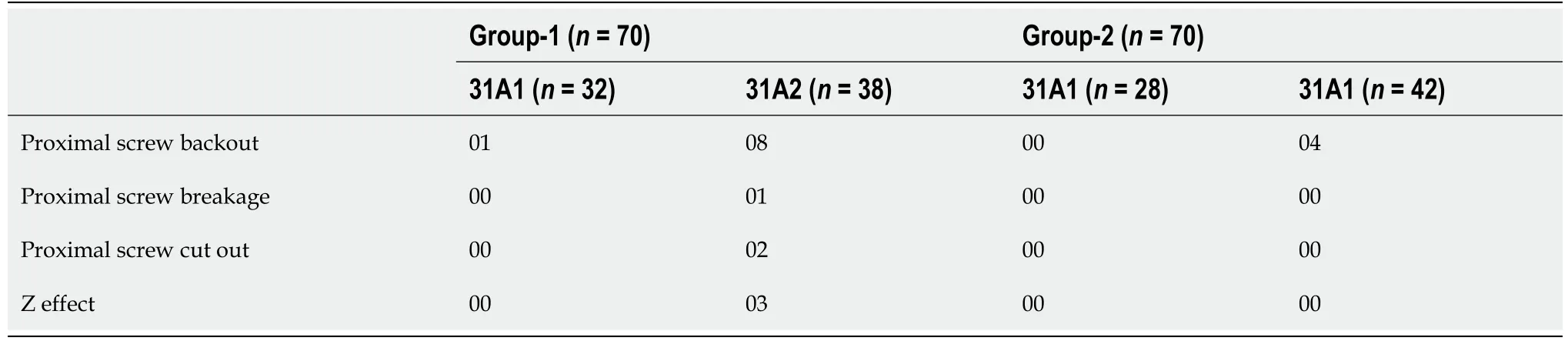
Proximal lock-related complications
As shown in Table 3,In group 1,2 out of 70(2.85%)patients had screw cut-out(Figure 2A),3 out of 70(4.28%)patients had Z-effect(Figure 2B),9 out of 70(12.85%)patients had a proximal screw back-out(average back-out = 14 mm)(also Figure 2C),and 1 out of 70(1.42%)patients had proximal screw breakage(also Figure 2D).In group 2,4 out of 70(5.71%)patients had a proximal screw back-out(average back-out = 7 mm).There was no Z-effect,screw breakage or proximal screw cut-out.
Time for radiological union
Average time of union was 14-16 wk in both groups for patients having fracture pattern AO/OTA 31-A1.However,in fracture pattern AO/OTA 31-A2,the average union time was 16-18 wk in group 1 and 15-16 wk in group 2(<0.001).There were 3 cases of non-union in group 1 and no cases of non-union in group 2.
Rotational alignment of the proximal femur
From this study,we concluded that in IT fractures AO/OTA type 31-A1,use of long anatomical PFN with or without distal interlocking screws gives similar results in terms of radiological union,postoperative proximal femur anatomy,and rotational alignment.However,in AO/OTA type 31-A2,use of long anatomical PFN without distal interlocking screws gave better results and less proximal lock-related complications than PFN with distal interlocking screws.
Anatomy of proximal femur
Varus rotation of the proximal femur was less than 5 degrees in both groups for all patients with AO/OTA 31-A1(= 0.81).In AO/OTA 31-A2,the mean neck shaft angle in group 1 was 117 degrees(114-125 degree),and the mean neck shaft angle in group 2 was 126 degrees(124-135 degree)(<0.001).This suggests that there was better control of the neck shaft angle where distal interlocking was not performed.
Downward migration of nail
We consider downward migration of the nail as a decrease in distance between the tip of the nail and the upper border of the intercondylar notch of the femur on the AP view of the radiograph.In group 2,6 out of 70 patients had downward migration of the nail due to controlled collapse of the fracture site,which averaged 5 ± 2 mm.Moreover,in 3 out of 70 patients in group 1,we observed that there was a change in position of the nail in relation to the distal dynamic interlocking screw.There was no downward migration of the nail in the patients in group 1 with static distal locking.
My son, go and lift your father s arm up on the bench, said the queen to one of the princes, for she easily knew the king again, although she was afraid to make herself known to him
Distal lock-related complications
In group 1,we noted thigh pain over the distal locking site in 19 out of 70(27.14%)patients,and 1 out of 70 patients had breakage of the distal lock due to downward migration of the nail resulting in autodynamization(Figure 3).No thigh pain was reported for any patient in group 2.In the postoperative period,5 out of 70 patients in group 1 had knee joint effusion,and no patient had knee joint effusion in group 2.
Clinical evaluation
In group 1,6 out of 70 patients had limb length discrepancy with mean shortening of 12 mm(6-18 mm),10 out of 70 patients had implant impingement,and 5 out 70 patients had decreased range of movement.In group 2,there was an average of 10 mm of limb shortening(5-15 mm),1 patient had implant impingement,and all patients had near to normal range of movement as compared to the opposite site.
DISCUSSION
The average operation time in group 1 was 42 min,and IITV radiation time was 59 s.In group 2,the average operative time was 28 min(<0.001)and IITV radiation time was 45 s(<0.001).This suggests that there was a significant reduction in operative time and IITV radiation time in group 2.(Table 2)
9.Axe6: The axe is connected to the Saints Joseph and Boniface [see below] (Biedermann 23). Both elder sons lack compassion and charity which the saints exhibited.Return to place in story.
Diagnosis is confirmed by plain radiographs in the AP and lateral views.Traction with internal rotation radiograph view is helpful in assessing significant fracture displacement if the patient is able to tolerate.The antero-posterior and lateral X-ray views of the whole femur are required for long anatomical PFN fixation.
The treatment of proximal femoral fractures with sliding hip screw implants involving an extramedullary or an IM device is a universally accepted method of fixation[4].In IM fixation there is minimal soft tissue dissection,less blood loss,a lower chance of infection,and fewer wound complications than extramedullary fixation,which has popularized PFN in IT fractures.
Her godmother only just touched her with her wand, and, at the same instant, her clothes were turned into cloth of gold and silver, all beset28 with jewels. This done, she gave her a pair of glass slippers30,40 the prettiest in the whole world. Being thus decked out, she got up into her coach; but her godmother, above all things, commanded her not to stay till after midnight,41 telling her, at the same time, that if she stayed one moment longer, the coach would be a pumpkin again, her horses mice, her coachman a rat, her footmen lizards, and her clothes become just as they were before.
At present,PFN is a favourable minimally invasive technique for treating proximal femur fractures,especially where closed reduction is achievable.Nonetheless,proximal lag screw cut-out,Z-effect,reverse Z-effect,femur fracture at the tip of nail or at the site of distal screw insertion,thigh pain as a result of iliotibial tract irritation or cortical hypertrophy and difficulty in insertion of distal interlocking screw are among the probable complications that can occur[1].
There was no pre-established treatment protocol for choosing a long nail or short nail for femoral IT fractures.However,many surgeons are reluctant to use short nails based on the historic literature showing high fracture rates.They also believe that long nails will avoid diaphyseal stress risers and make peri-prosthetic fracture rates acceptable[9].Short PFNs do not follow the anatomical curvature and the tip may impinge the endosteum of the anterior femoral cortex giving rise to anterior thigh pain.Long PFNs follow the anatomical shape of the femur and would not cause such a problem.At our institute,we have been using long anatomical PFNs.We routinely use long PFN with two proximal interlocks that maintain IT fracture reduction in good valgus position and provide excellent rotational control of the proximal fragment.
He took the precaution of surrounding the palace with a dense32 cloud, and then hastened to his Court, where his prolonged absence was causing much anxiety
Hardware or fixation failure is not related to the type of nail,implant material or AO/OTA classification,but a neck shaft angle of <125 degrees leads to a significant increase in fixation failure[10].The influence of varusmal reduction for femur neck fractures and trochanteric fractures was described previously[11].An increased varus reduction is associated with a higher cut-out rate after sliding hip screw fixation.An increased valgus reduction is beneficial for screw positioning resulting in stable fixation of the femoral head and neck[12].Kashigar[13]showed a significant association between an increased varus reduction and cut-out for cephalo-medullary nailing.In addition to nail design,surgical method is also an important factor in determining the incidence of the above-mentioned complications.
The motivation of this study was to assess the clinical and radiological outcomes of PFN with or without distal interlocking screws in fracture pattern AO/OTA 31-A1 and 31-A2,which were performed by the same chief surgeon.
There are few studies comparing clinical and radiological outcomes between proximal femoral nail(PFN)with or without distal interlocking screws in fracture pattern Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association(AO/OTA)31-A1 and 31-A2.
In unstable IT fractures(31-A3),the lateral cortex of the femur is fractured.This includes reverse oblique and transverse fracture patterns with particular anatomical and mechanical properties.Weight bearing on the affected limb gives rise to shearing movement at the fracture site that results in telescoping of the implant[15].When IM nailing of this unstable fracture pattern was done without distal interlocking screws,neither longitudinal nor rotational stability was attained.Thus,this fracture is not fixed firmly without a distal interlocking screw.However,we concluded that distal interlocking screws are needed for unstable IT fractures(31-A3),particularly those with subtrochanteric extension of the fracture or those with wide IM canals.
Hardy[16]stated that use of two static locking screws during IM fixation of IT fractures is correlated with a higher rate of cortical hypertrophy,while the use of a dynamically locked nail significantly decreases the rate of this complication.On the basis of these findings,we discontinued the use of distal interlocking screws in AO/OTA 31-A1 and 31-A2 IT femur fractures.
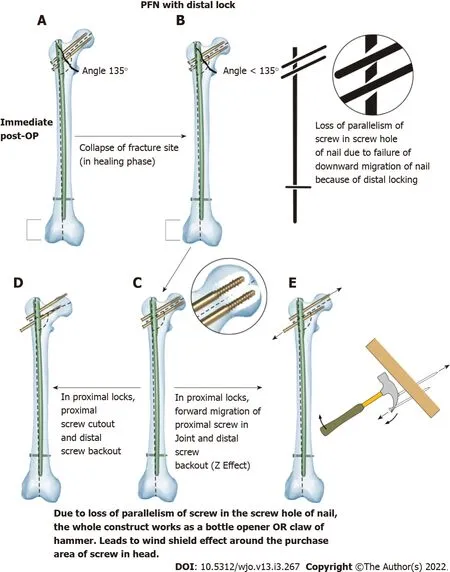
Figure 4 shows a typical case where PFN with distal locking was performed.In the immediate postoperative period(Figure 4A),the proximal femoral neck shaft angle was maintained.In the healing phase,there was collapse of the fracture site,but the proximal femoral neck shaft angle was not maintained.There was loss of parallelism of the screw in the screw hole of the nail due to failure of downward migration of the nail because of distal locking(Figure 4B).The whole construct works as a bottle opener or hammer claw,that leads to a windshield wiper effect around the purchase area of the screw in the head(Figure 4C)resulting in forward migration of the proximal lag screw and back-out of the distal lag screw.Due to this loss of parallelism,there can be screw back-out,screw cut-through from the femoral head(Figure 4D),Z-effect(Figure 4E),reverse Z-effect,and screw breakage.
In the meantime, good fortune returned to the miller s house. He succeeded in everything that he undertook. It was as though the trunks and strongboxes filled themselves of their own accord, and as though money in a chest multiplied overnight. Before long his wealth was greater than it had ever been before. However, it did not bring him happiness without concern, for his agreement with the nixie tormented8 his heart. Whenever he passed the pond he feared she might appear and demand payment of his debt.
The patients were evaluated based on the following clinical and radiological parameters:(1)Fracture patterns according to the AO/OTA classification;(2)Duration of surgery(starting from skin incision to skin closure);(3)Time of IITV radiation exposure;(4)Time to radiological union;(5)Implant-related complications like backing-out of proximal screws from the lateral cortex of the femur,‘Z’ effect,screw breakage,cut-through of implant from femoral head,breakage of distal interlocking screw,and breakage of nail;(6)Anatomy of the proximal femur(neck shaft angle of femur);(7)Level of the distal lock screw in relation to the nail in the anterior posterior(AP)view of the postoperative radiograph and radiograph after union were compared in group 1 and the downward migration of the nail in the IM canal in the AP view of the postoperative radiograph and radiograph after union were compared in group 2;and(8)Length and rotation of the limb after healing.
Metaphyseal fractures heal by direct bone contact and creeping substitution.In comminuted IT femur fracture,controlled collapse at the fracture site is desirable for fracture union because of resorption and comminution at the fracture site.Therefore,in such situations,if there is a static implant bone construct,then there would be an increase in friction at the junction of the nail and screws(Figure 4).This would increase probability of Z-effect,reverse Z-effect,implant breakage,cut-through of screws and back-out of lag screws in the proximal femur.Whereas in cases where distal locking was not performed,the parallelism between the screw hole and screw will be maintained,and the controlled desired collapse with a maintained neck shaft angle would occur,which would increase the chances of fracture union(Figure 5).
18.Asked to speak with his majesty: For a low ranking subject, gaining an audience with the king is not usually such an easy task, often requiring an appointed time except in the case of an emergency. Puss skill with diplomacy and words are part of his cunning success.Return to place in story.

In PFN that is done without distal locking,it is desirable to keep the nail length up to the superior border of the patella.A nail with a length up to the intercondylar notch of the femur will not allow downward migration.Therefore,it is desirable to keep a nail short to allow downward migration of the nail with controlled collapse of the fracture.
In our study,it was noted that in the cases for which distal interlocking was performed,there was a gradual decrease in the neck shaft angle,which led to varus collapse and failure of bone implant construct in 21.40% of patients.
There was no significant difference in radiological union,postoperative rotational alignment and proximal femur anatomy between both groups with fracture pattern AO/OTA 31-A1,but the incidence of proximal lock-related complications was increased in group 1 patients with fracture pattern AO/OTA 31-A2 than in group 2 patients with fracture pattern AO/OTA 31-A2(Table 3).
In the distance I saw some little houses which seemed to be built in a most singular fashion, but as I was by this time very hungry I set out towards them, but before I had walked many steps, I saw that the air was full of shining objects which seemed to be fixed, and yet I could not see what they hung from
The limitations of our study were a short follow-up period and a small sample size.We also used only one type of long anatomically designed PFN with two proximal locks.
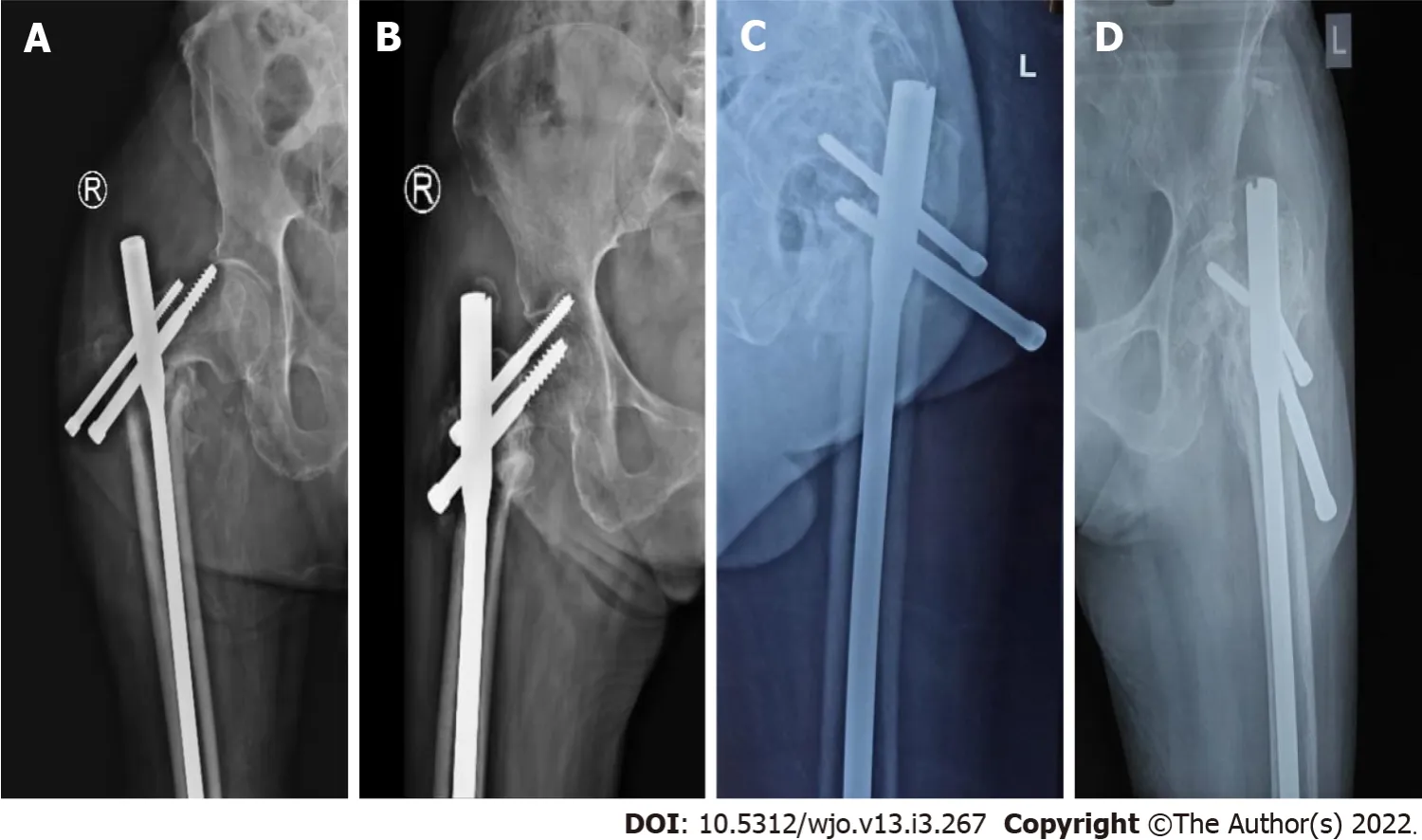
Case 1
A 68-year-old female patient sustained an IT femur fracture(AO/OTA 31-A2)on the right side(Figure 6A).A long anatomical PFN with two proximal screws without distal interlocking were used for the operation,as shown in immediate postoperative X-ray(Figure 6B).The X-ray image in Figure 6C showed a complete union at 12 mo with maintained neck shaft angle and distal downward migration of the nail,as compared to that in Figure 6B.
CONCLUSION
Compared to the opposite limb,there was an average of 5 degree external rotation difference in fracture pattern AO/OTA 31-A1 in both groups(= 0.66).There was an average of 6 degrees more external rotation in group 1 with AO/OTA 31-A2 fracture pattern,and there was an average of 7 degrees more external rotation in group 2 with fracture pattern AO/OTA 31-A2(= 0.08).Malrotation of the operated limb was less than 10 degrees in all patients in both groups.This suggests that there was a negligible effect of distal interlocking on the rotational alignment of the limb for fracture patterns AO/OTA 31-A1 and AO/OTA 31-A2.
His behavior often left us without funds for other more important things. After the dress incident, there was no money for the winter coat I really needed--or the new ice skates I wanted.
ARTICLE HIGHLIGHTS
Research background
The pattern of the fracture had a significant effect on the distal interlocking of the nail.In stable IT fractures(31-A1 and 31-A2),the lateral cortex of the femur is unaffected.After anatomical reduction when the proximal locks are inserted from the lateral wall of the distal fracture part into the femoral head and the IM nail is matched well to the medullary canal,then varus deformity of the hip joint and rotational instability are controlled by the nail-proximal lock structure.In stable IT fractures,good cortical connection is established after acceptable reduction,and most of the compressive forces on the fracture site are borne by the bony cortex along the axis of neck of femur after surgery.Thus,performing distal interlocking of the nail was found to be unnecessary.
4. Cake, and this little pot of butter: These are the food items originally described by Charles Perrault. Later versions have included other food items, most often a bottle of wine.Return to place in story.
Research motivation
Some personnel have supported the IM nailing without distal locking through their biomechanical studies.A biomechanical study done by Lacroix[14]comprised of 10 paired human cadaveric femurs and gave significant support that an added hole in the distal part of the IM nail could reduce the mean failure load in torsion by 36% because a stress raiser is a factor for peri-implant fracture.
Research objectives
The objective of this study was to compare the outcomes of intertrochanteric(IT)fractures(AO/OTA 31-A1 and 31-A2)treated by PFN with and without distal interlocking screws.
Research methods
We conducted a retrospective study of 140 patients having fracture pattern AO/OTA 31-A1 and 31-A2.We divided the patients into two groups based on distal interlocking.We evaluated patients based on clinical and radiological parameters like fracture type,duration of surgery and IITV radiation time,time for radiological union,proximal lock and distal lock-related complications,femoral neck shaft angle and length and rotation of limb after surgery.
Research results
There was no significant difference in radiological union,postoperative radiological alignment and proximal femur anatomy between patients with fracture pattern AO/OTA 31-A1 treated by PFN with or without distal interlocking.However,the incidence of proximal lock-related complications was higher in patients with fracture pattern AO/OTA 31-A2 treated by PFN with distal interlocking than in patients treated by PFN without distal interlocking.
Research conclusions
PFN without distal interlocking is a reliable and acceptable option for IT fracture types AO/OTA 31-A1 and 31-A2.
Research perspectives
A prospective study with long-term follow-up and a larger number of patients is necessary to draw a definitive conclusion.
FOOTNOTES
Lil NA,Makwana VR,Patel TD and Patel AR made substantial contributions to the study conception and design,to the acquisition,analysis and interpretation of data,and to the drafting of the article and making critical revisions related to important intellectual content of the manuscript;and all authors provided final approval of the version of the article to be published.
This study was reviewed and approved by the NHL institutional review board(NHLIRB).
Patients were not required to give informed consent to the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent.
The authors declare that they do not have any conflicts of interest.
No additional data are available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
India
“Oh, how I have been detained!” said the little maiden, “I wanted to seek for little Kay. Do you know where he is?” she asked the roses; “do you think he is dead?”
Nadeem A Lil 0000-0002-9805-3105;Vipul R Makwana 0000-0002-6656-949X;Tirth D Patel 0000-0002-2354-8007;Arjav R Patel 0000-0001-8064-8517.
He had the miller s daughter put into another room full of straw, much bigger than the first, and bade her, if she valued her life, spin it all into gold before the following morning
Wang JJ
A
Wang JJ
 World Journal of Orthopedics2022年3期
World Journal of Orthopedics2022年3期
- World Journal of Orthopedics的其它文章
- Patient-specific instrumentation in total ankle arthroplasty
- Diagnosis,treatment and complications of radial head and neck fractures in the pediatric patient
- Conservative treatment of knee osteoarthritis:A review of the literature
- Functional and radiological outcomes of different pin configuration for displaced pediatric supracondylar humeral fracture:A retrospective cohort study
- Accuracy of shoulder joint injections with ultrasound guidance:Confirmed by magnetic resonance arthrography
- Ilizarov bone transport combined with the Masquelet technique for bone defects of various etiologies(preliminary results)