
Development and psychometric evaluation of the nurse behavior toward confirmed and suspected HIV/AIDS patients (NB-CSHAP) scale
2022-03-31 07:00:04JantAlxislosSantosNorbrtoMillaCyruzTuppalLooroLabragu
Frontiers of Nursing 2022年1期
Jant Alxis D los Santos, Norbrto Milla, Cyruz Tuppal, Looro Labragu
aDepartment of Nursing, Visayas State University, Visca, Leyte 6521, Philippines
bGraduate School, St Paul University Philippines, Tuguegarao, Cagayan Valley 3500, Philippines
cDepartment of Statistics, Visayas State University, Visca, Leyte 6521, Philippines
dCollege of Health Allied and Medical Professions, University of San Agustin, Tuguegarao, Iloilo, Visayas 5000, Philippines
eFundamentals and Administration Department, Sultan Qaboos University, Muscat, Muscat 112, Oman
Abstract: There is a scarcity of literature discussing nurses’ behaviors toward caring for suspected or confirmed human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) patients. The development of a scale specific to measure nurses’ behaviors will allow health institutions to assess the disposition of their nurses in terms of HIV care. This study aims to present the rigors of developing and validating a reliable instrument to contextualize these nurses’ behaviors. This study utilized a sequential exploratory mixed method design to develop the NB-CSHAP scale. Thematic analysis was done on the qualitative data from the interviews with persons living with HIV/AIDS (PLHA) from which items were selected to be included in the scale. Exploratory factor analysis was utilized to extract the factors and Cronbach’s alpha was used to assess the reliability of the instrument. Four factors were extracted and are categorized as either caring or discriminatory behaviors. These include: (1) service-oriented, (2) openhanded, (3) perceptive, and (4) discriminatory. The scale has an internal consistency of 0.73. The scale shows acceptable psychometric properties, hence can be used to assess the nurses’ behaviors in caring for confirmed or suspected HIV clients. The scale may be used by health institutions to determine the quality of the patient care provided by their nurses to clients with confirmed or suspected HIV.
Keywords: caring behaviors · HIV/AIDS care · nursing · scale development · sequential exploratory mixed method design © Shanxi Medical Periodical Press.
1. Introduction
The essence of nursing is caring, which identifies the lifeline of the profession. As discussed by scholars in the field, the culture of caring in nursing should be initiated during the formative years of a prospective nurse where the concept of caring should be cultivated and nurtured to rear a culture of humanistic and caring behaviors.1In practice, it is essential that a competent nurse does not only possess the necessary theoretical knowledge but also imbibe the discernment of caring in her workstations, especially toward patients under her care.
1.1. Review of literature
Caring can be classified into two generalized types as follows: instrumental caring and expressive caring.2Instrumental caring involves behaviors that are related to the technical aspects of care, such as performance of nursing intervention at bedside, and performing other professional expertise in providing care. In contrast, an expressive caring behavior pertains to the psychoemotive role invested by a nurse toward the patient. Examples of such behavior may refer to actions such as active listening, offering emotional support, and ensuring genuine presence.2In nursing practice, caring is universal and nondiscriminatory. However, its vulnerability to being influenced by several human and social factors is indisputable. Undeniably, the existence of stigma and discrimination in health care settings, particularly toward human immunodeficiency virus or acquired immunodeficiency syndrome (HIV/AIDS), continuously grow in number, causing late presentation and poor health outcomes of persons living with HIV (PLHIV).3,4Ideally, it is projected that by the year 2030 90% of those with HIV will be diagnosed, and 90% of those diagnosed will be on HIV antiretroviral therapy (ART), and 90% of them shall be undetectable of HIV.5Although there are efforts initiated by different health sectors such as government, private, and non-government organizations in controlling the incidence of stigma and discrimination in their countries to meet the global goal of 90-90-90, the issue remains a challenge up to the present time, especially among low resource countries.
One of the most discussed topics in the literature that is linked to HIV/AIDS stigma and discrimination is the attitude of the health care workers toward these patients. A study strongly suggest the importance of an organization-led intervention to implement strategies where all of its constituents and not only those on direct patient care, practice quality improvement in responding to organization-wide mitigation of HIV stigma and discrimination.6The literature discussed that the lack of proper training and education on HIV among nurses contributes to the stigmatizing and discriminatory attitudes.7-9When there is a repeated opportunity to care for these patients, it is revealed that training and education reduce prejudicial attitudes and fear of HIV/AIDS.10When nurses feel more confident and have enough awareness of how they can protect themselves, they display more willingness to care for HIV positive patients.11,12
There are instruments and scales developed by various researchers that can be used in measuring the nursing practices in HIV care, which will help in improving it. There are valid and reliable scales assessing HIV stigma among nurses and their interaction with patients, and this includes the HIV stigma instrument-nurse (HASI-N).13Similarly, the provider perception inventory (PPI)14assesses health provider stigma on HIV/AIDS, substance abuse, and behaviors of men having sex with men. There are also scales measuring three dimensions, including self-stigma of the patients, their social stigma, and stigma in health facilities.15Another study came up with a scale that measures not only the inducer to stigma in health facilities but also the attitudes of the health personnel toward PLHIV.16There are also studies examining the attitudes of the care providers such as those conducted in Iran,17Egypt,18and Italy.19
Notably, however, there is a scarcity of observational studies, especially on the use and development of scales measuring the behaviors of care providers, particularly the nurses caring for both suspected and confirmed HIV/AIDS patients. There is a growing number of reports suggesting the lack of awareness of nurses of them being perceived as discriminatory by their patients.20-22It is on this note that the authors came up with this preliminary study to identify these behaviors and develop a measure on the nurses’ behaviors toward people with confirmed or suspected diagnosis of HIV/AIDS.
1.2. Study aim
The apparent lack of a necessary instrument that centers on the nurses’ behaviors toward these population (confirmed and suspected HIV) prompted this initiative. This study aims (1) to explore the experiences of nurses in caring for patients with suspected or confirmed HIV; (2) to develop a valid and eliable instrument to measure nurses’ behaviors toward these clients, and (3) to explain the relevance of utilizing a mixed method design in the conceptualization and development of a scale.
2. Methods
The study utilized a sequential exploratory mixed method design, which uses a descriptive approach in the qualitative phase and an exploratory factor analysis in the quantitative phase (Figure 1).
Following this sequential method, we implemented two separate procedures of data collection and participant selection. Logical approaches guide the sequential exploratory mixed method design in the collection, analysis, and integration of both quantitative and qualitative data in a single study.23The method is thought of as an ideal protocol to be used in tool development24-26(Table 1).
2.1. Qualitative phase
In this phase, descriptive qualitative inquiry was utilized to assess their experiences. The participants were asked to use the guide question, “How was your experience in caring for a suspected or confirmed HIV patient?” Subsequent probing questions were asked from our informants, which facilitated gathering of rich qualitative information.
2.1.1. Participant recruitment, sampling, and setting
There were 17 key informant nurses who were purposively selected and interviewed face-to-face after their hospital duty. The nurses from private and government hospitals were pre-selected to represent different hospital areas or workstations. Inclusion criteria are as follows: (a) a registered nurse, with experience in caring for both suspected and confirmed patients diagnosed with HIV/AIDS; (b) has willingness to share their experiences of patient interaction. The nurses who do not have clinical functions and those who have no actual experience in caring for patients with HIV/AIDS are excluded.

Figure 1. Sequential exploratory mixed method design.
2.1.2. Data collection
A letter of intent to conduct the study, the university approved research protocol, and ethical clearance were forwarded to the different hospitals for institutional approval. Once secured, an initial discussion with the Chief Nurse was made to identify key nurses who fit in the inclusion criteria for the interview. A participant informant packet and an informed consent were secured before the interview. An audio recorder was utilized to facilitate data gathering.
2.1.3. Data analysis and item development
The recorded interview was transcribed and translated into English, which was counterchecked by an English major. The qualitative texts were analyzed using thematic analysis. The transcripts were analyzed and coded by the researchers to find embossed patterns identified through the reading and re-reading process guided by Braun and Clark’s framework.27The codes that share the same meaning were grouped into one, along with the transcripts which were utilized for item pooling to be used for the NB-CSHAP instrument. Initially there were 36 items that were identified in the raw pool of items. Transcripts that share the same meaning were removed to ensure that unique items were included in the tool. There were 16 items included in version 1 of the NBCSHAP instrument.
2.1.4. Rigors and trustworthiness
The results of this study were made credible through bracketing which was done prior to the first encounter with the participants. As a nurse, the researcher poured all her perceptions and biases in caring for patients with HIV in a journal. The researcher ensured that the data that will be utilized is grounded on the data gathered from the nurse participants. The researchers achieved data saturation to ensure transferability. Dependability and confirmability was achieved through intercoder reliability checks to minimize biases.

Table 1. Implementation matrix.
2.2. Quantitative phase
In this phase, the first draft of the instrument was explored for content validity and reliability.
2.2.1. Content and face validity
The first draft of the instrument was returned to the interviewees for member checking and initial face validation. There were 11 subject matter experts in the field of nursing, HIV/AIDS care, statistics, and research instrumentation who took part in the evaluation of the instrument. The experts assessed the instrument’s item coherence, grammar, appropriateness to the construct the scale intends to measure as well as the scoring instructions. The validity of the content was computed using the content validity index (CVI). The CVI was calculated following the standard computation for both item and scale CVI. Specifically, item-CVI (I-CVI) was computed by counting the number of experts who gave a“very relevant”score on the item, divided by the total number of experts who rated. On the other hand, the scale-CVI (S-CVI) was computed using averaging. This was done by summing up the I-CVI score of the item divided by the total number of items. An excellent S-CVI is described for scales scoring ≥ 0.9.28
2.2.2. Sampling and sample size
Following DeVellis’29protocol of 1:5 item-sample ratio, a minimum of 85 samples will suffice for the factorial analysis. However, this study was able to get 400 nurse participants or an excess of 125 samples making the sample size highly adequate for the factorial analysis.
2.2.3. Participant recruitment and setting
The instrument was field-tested online via Surveymonkey. The link was forwarded to different nurse organizations, cell groups, as well as nurses known to the researchers. The link was subsequently sent to their group chats for answering. A total of 400 nurses working in various health facilities participated in the survey. Inclusion criteria are nurses who are in service for at least 6 months, and had experience in caring either a suspected or confirmed case of HIV/AIDS. Excluded are nurses who do not have clinical functions. The researchers ensured the faculty of each participant by verifying from their affiliations.
2.2.4. Statistical data analysis
The data was analyzed for intercorrelations using Bartlett’s test of sphericity, and Kaiser-Meyer-Olkin (KMO) test was used to determine if data is suited for factor analysis. We utilized the principal component factor as the extraction method. The Kaiser’s criterion (eigenvalue >1) was used to determine the number of factors to retain in the factor solution. Varimax rotation was used for easy interpretation of the items in each of the retained factors. The identified factors, as well as the entire scale, were tested for internal consistency and reliability using Cronbach’s alpha. These were analyzed using the STATA v15.1 software.
3. Results
3.1. Qualitative findings
There were two overarching dichotomous themes revealed from the textural interview data. The first overarching theme found throughout the nurse participants’ stories were theirquintessential behaviors:The positive or quintessential behaviors were related to the following clusters coded as Compassion, Nondiscrimination, Connecting, Self-preservation, Mentoring, Professional Competence, Confidence, Humor, Generosity, Altruism, and Presence. The second overarching theme found throughout the nurse participants’ narratives were related to some of theirnegative behaviors.These negative behaviors were mostly related to the following clusters: gossiping, excessive personnel protective equipment (PPE) use, refusing to care, detachment, anxiety, and fear.
3.2. Quantitative results
3.2.1. Profile of nurses
The nurse participants of this study are mostly females (71%), with a mean age of 29.9 years old (SD = 6.8), unmarried (72.5%), finished BS Nursing degree (83%), and have joined the profession in the last 8.2 years (SD = 6.4). Most of the nurses are holding a permanent position (67.5%) and has been working for <5 years in their present assignment (71.5%) as a staff nurse (88.3%) in medical-surgical stations (f =130) in private hospital facilities (52.5%) located in urban areas (68.5%) (Table 2).
3.2.2. Content and face validity
The I-CVI of the NB-PHG Scale ranges from .80 to 1 point. This suggests that the items are considered as relevant items.28The S-CVI (Ave) of the NB-PHG Scale revealed 0.95 points indicating that the scale has excellent content validity.30

Table 2. Continued

Table 2. Characteristics of the nurse participants.

Table 3. Intercorrelation coefficients of the NB-CSHAP Scale.
3.2.3. Assessment of item-intercorrelations
Using Bartlett’s test of sphericity, it revealed that the data on the scale is significant (p =0.000). To further verify this, the measure of sampling adequacy test was done and revealed a KMO value of 0.84, indicating a sufficient amount of shared variance among the item scores (Table 3).
3.3. Extraction of factors
We utilized the principal component factor as the factor extraction method in the developed instrument. There were two methods utilized to assist the researcher in the decision of retaining factors. The first step used was the Kaiser’s criterion or the eigenvalue rule, which suggests that factors with an eigenvalue of 1.0 or more are retained for further analysis. The eigenvalue of a factor represents the amount of the total variance explained by that factor. The results revealed that there were four factors that have eigenvalues of >1.00. This suggests that four factors may be extracted from the NB-CSHAP scale (Table 4). When these four factors are extracted, this can explain 59.3% of the scale’s total variance. To verify this, the researcher used the second approach, which is Cattell’s scree test. This is a more visual guide in determining the number of factors that were retained (Figure 2).
3.4. Reliability score
Cronbach’s alpha was determined twice (Table 5): (1) totality of the scale, and (2) per factor (subscale). Results revealed an acceptable internal consistency of 0.73 reliability score31for the entire 16-item scale. However, when per factor internal consistency was examined, it showed that Factors 1 and 2 have acceptable reliabilities, while Factors 3 and 4 have low-reliability scores. This may be because of the low number of items in the subscale.
3.5. Scoring
The behaviors which are negatively stated are reversescored such that the highest score of 5 are scored as 1, and the lowest score of 1 is scored as 5. The items for reverse coding are those that belong to discriminatory behaviors subscale. The highest possible score for this scale is 80. Specifically, the scores are described as appropriate/caring behaviors (53-80 points); mediocre behaviors (26-52 points), and undesirable/stigmatizing behaviors (0-25 points).
3.6. Mixed-method results
The sequential exploratory mixed method on this study is an appropriate method in unifying techniques in designing and developing an instrument. The qual-quan sequence observed on this study illuminated qualitative exploration of the nurses’ experiences in caring for patients with HIV/AIDS which were the basis on which a reliable scale can be developed.
4. Discussion
This study aimed to develop a valid and reliable tool to assess nurses’ behaviors in caring for suspected or confirmed HIV/AIDS patients. A sequential exploratory mixed method is a useful method in developing healthrelated scales32,33which was the primary method utilized in this study. The current study was able to produce a valid and reliable instrument composed of 16 items with four distinct factors. The face-to-face interview, which the researchers did as a preliminary step, broadened our understanding of the nurses’ experiences, views, and perceptions in their care toward patients who are suspected or confirmed case of HIV/AIDS. The sequential approach from the key informant interviews and the use of experts in the field substantiate that the items generated in the scale are concise and non-ambiguous. It is a common practice to request the expertise of subject matter experts in developing quality scales and measurements.34,35Hence, it is essential to select qualified and esteemed experts in the field to evaluate a tool being developed to ensure that relevant suggestions and critical points can be integrated for an improved version of the instrument.

Table 4. Factor loadings of the NB-CSHAP Scale items.
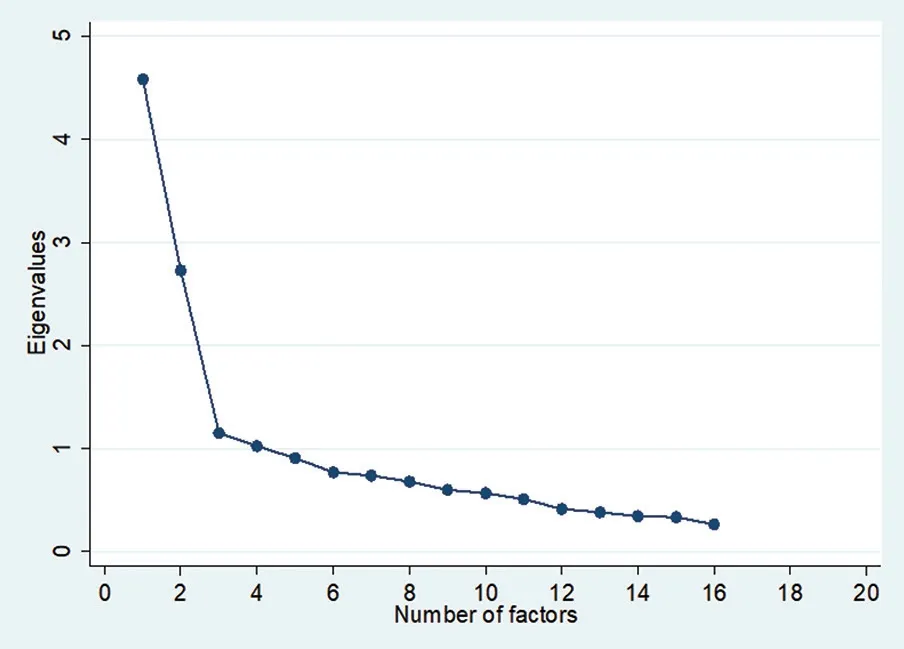
Figure 2. Scree plot on the factors identified in the NB-CSHAP.
Multiple approaches were utilized to test the validity of the instrument in this study. Although a weak valuation, the initial assessment through the face and content validation of the tool, suggests that the newly developed tool is a valid instrument. The constructive suggestions and recommendations of the panel of subject matter experts significantly improved the readability and coherence of the NB-CSHAP instrument. Items that seemed vague and insignificant were excluded, which enhanced the integrity of the scale.

Table 5. Psychometric properties: Alpha coefficient of internal consistency of the NB-CSHAP scale.
Based on the number of subjects, we were able to meet the minimum criteria of 1:5 item-to-subject ratio to proceed for factor analysis and assess the psychometric properties of the newly developed instrument. Furthermore, both the KMO and Bartlett’s test of sphericity suggests that the data is adequate for factor extraction. The acceptable internal consistency as derived after using the Cronbach’s alpha is an indication that the items in the scale measure the same construct it intends to measure. The acceptable Cronbach’s alpha suggests that the scale is a reliable instrument to measure the construct of nurses’ behaviors.
4.1. The NB-CSHAP scale structure and contents
The four identified factors were named discriminatory behaviors, service-oriented behaviors, openhanded behaviors, and perceptive behaviors, which were described based on the items the factor categories.
Factor 1. Refers to behaviors showingserviceorientedbehaviors.The seven items under this factor describes a nurse who displays behaviors true to her professional calling. Nursing is a profession that provides caring services to patients who are in need. Typical examples discussed in the literature highlights the importance of these behaviors in nurse-patient interaction.36-38Service-oriented behaviors in the nursing profession are acts that imbibe the expression of compassion, professionalism, nondiscrimination, and mentoring. An example under this category is item number three that states, “I offer guidance to my junior nurses who are new in handling critical cases.” Communicating with colleagues such is vital for quality patient care.39The behavioral exchange that transpires during this process is anchored on the goal of patient safety.
Factor 2refers to discriminatory behaviors. These are items that describe stigmatizing and discriminatory behaviors. Here four items are included that depict acts of gossiping, avoidant behavior, and detachment. Literature explicitly discussed that care providers such as nurses are prone to display negative behaviors especially when they lack adequate knowledge of HIV.11,40
Factor 3refers toopenhandedbehaviors. These are benevolent behaviors that reflect the acts of presence, generosity, and the provision of holistic care. Holistic caring behaviors are always emphasized in nursing as a necessity to be practiced by those in the profession. To be a holistic nurse entails the provision of care on the entirety of human facets comprising the physiological-psycho-social and spiritual needs. Bakar et al.41suggest nurses have more caring attributes when they are spiritually rooted.
Factor 4refers toperceptivebehaviors. These are behaviors that pertain to being sensitive when the need arises. These are behaviors of humor and altruism. A sympathetic nurse can inject humor while at work, especially in stressful situations. Similarly, altruistic actions such as risking the self when necessary are selfless behaviors where a nurse prioritizes what is for the best interest of patients under her care. Alavi et al.42discussed how nurses tend to possess empathetic tendencies and self-sacrifice in their workstations. Perceptive behaviors are related to the sense of the sensitivity of a nurse to make difficult situations as pleasing as possible.
In summary, the NB-CSHAP scale is generally classified into two distinct behaviors: the caring behaviors and stigmatizing behaviors. Caring behaviors comprise the SOP in caring which consists of service-oriented behaviors, openhanded behaviors, and perceptive behaviors. The SOP behaviors are the quintessential behaviors a nurse must possess when caring for patients suspected or confirmed with HIV/AIDS. On the other hand, behaviors considered as stigmatizing behaviors are prone to be misconstrued as offensive and discriminatory.
4.2. Integrated mixed-method findings
The value of the qualitative component in designing the instrument using mixed-method design relies on the fact that the items included in the devised tool were organic on the experience of the participants. Following this premise, it makes the instrument a legitimate and authentic instrument on the construct it intends to measure.
4.3. Implications to nursing practice
The scarcity of a scale to measure the nurses’ behaviors in the literature is an indication that the construct has not been explicitly contextualized, particularly toward patient care with suspected and confirmed HIV/AIDS. This novel initiative in measuring behaviors will provide a deeper understanding of specific actions that are often misinterpreted or challenging to understand. The authors believe that studies related to HIV care can be improved further and not limited to determining only the knowledge and attitudes of nurses but rather include assessment of their behaviors. These behaviors are essential in involving and engaging into the secluded life of persons with HIV.43The newly developed NB-CSHAP scale can support studies and investigations related to the nurse’s interaction with an HIV patient. The scale can be used by health facilities, especially among nurse supervisors, to assess the behaviors of their nurses to foster an improved behavior toward patients with HIV/AIDS. Nurse leaders can strategize measures to enhance the caring behaviors of nurses, which is an essential step in reducing HIV stigma in health facilities. Reducing, if not eliminating stigma prone behaviors, will not only improve the quality of nursing practice but also ultimately achieve improved patient outcomes.
5. Conclusion
Using a sequential exploratory design is an ideal approach to tool development. The scholarly and rigorous method of the tool development process provided a deeper understanding of the nurse behaviors and their interactions with persons suspected or diagnosed with HIV/AIDS. This study was able to contextualize the nurses’ behaviors as they interact with their suspected or confirmed HIV/AIDS patients. The findings of this study provide initial evidence that the newly developed NB-CSHAP scale composed of 16 items is a valid and reliable instrument to assess nurses’ behaviors toward patients with suspected or confirmed HIV case.
Limitations
This study is not without limitations. First is that the NBCSHAP scale was developed in the context of Philippines. There may be cultural differences in behaviors and linguistics used compared to other countries and environments, which delimits the applicability of the items included. Second is the analysis used. The study only utilized EFA and not confirmatory factor analysis (CFA) since the intention of this study was primarily to identify the latent factors in the newly developed scale and its intercorrelation between factors. The high validity and acceptable reliability scores derived from this study were based only on the participants and circumstances when the data was gathered. Future researchers are encouraged to use CFA to test the factors as well as the validity and reliability of the scale in their respective health settings. Furthermore, behaviors are best measured when observed; hence it is suggested that the scale be validated not only by the nurses but must also involve their patients as care recipients.
Acknowledgements
The authors would like to express gratitude to the nurses who participated in this study.
Ethical approval
This study complied to the basic ethical procedures and was technically and ethically evaluated and cleared by the St. Paul University Philippines Ethics Review Committee with protocol code number 2018-01-PhDNS-11. The researchers secured an informed consent prior to initiating data gathering.
Conflicts of interest
All contributing authors declare no conflicts of interest.

- Frontiers of Nursing的其它文章
- Frontiers of Nursing Call for Papers
- Common psychological disorders in elderly and their correlations with social support, Shiraz, Iran, 2018†
- Psychometric properties of the Persian version of the European heart failure self-care behavior scale
- Experiences of implementing a coping mechanism for the elderly who face chronic diseases while living with the family: a phenomenology study
- Person-job fit and work-life balance of female nurses with cultural competence as a mediator: evidence from Nigeria
- Effects of the self-management training program on self-management behavior and blood pressure levels among elderly people with hypertension