
Psychometric properties of the Persian version of the European heart failure self-care behavior scale
2022-03-31 07:00:00RezNorouzdehMohmmdrezHeidriAnoshirvnKzemnejd
Frontiers of Nursing 2022年1期
Rez Norouzdeh, Mohmmdrez Heidri,*, Anoshirvn Kzemnejd
aDepartment of Nursing, Nursing and Midwifery Faculty, Shahed University, Tehran 3319118651, Iran
bDepartment of Biostatistics, Faculty of Medical Sciences, Tarbiat Modares University, Tehran 1411713116, Iran
Abstract: Objective: To investigate the psychometric properties of the self-care behavior scale in heart failure (HF) patients. The development of self-care behaviors is one of the goals of non-pharmacological care management programs. Methods: After translating the European Heart Failure Self-care Behavior scale (EHFScBS), validity was assessed through explanatory factor analysis; additionally, reliability was assessed through Cronbach alpha and test-retest. The samples comprised of 120 HF patients admitted to hospitals in Tehran during 2017-2018. Results: The mean age of the samples was 67.3 ± 14.04 years. Fifty-four patients (45%) were female. All items of the scale had an acceptable factor loading. Cronbach alpha coefficient was 0.72. The intra-cluster correlation coefficient (ICC) was 0.69. Conclusions: Nurses and clinicians could benefit from the Persian version of HF self-care scale since it would enable them to rapidly assess patients’ self-care behaviors and to evaluate the effectiveness of the HF management.
Keywords:heart failure · questionnaire · reliability · self-care · validity © Shanxi Medical Periodical Press.
1. Introduction
Heart failure (HF) is one of the major health problems in the world, ranging from 1% to 2% of adults and is projected to reach 25% by 2030.1,2HF is a complex syndrome3with high mortality.4To improve health outcomes, self-care as an important component of HF intervention5is always emphasized in these patients.6Self-care is a key strategy in the long-term management of chronic HF.7Self-care includes choosing behaviors that offer an appropriate response to the signs and symptoms of HF.8Successful treatment of HF depends on complete self-care and adherence to treatment regimen.9Selfcare increases the quality of life and reduces hospital readmission, mortality, and costs.1,10It will be difficult to cure HF patients with poor self-care.11In a way, noncompliance with treatment recommendations leads to increased readmission of these patients.12
The development of self-care behaviors is one of the goals of non-pharmacological care management programs. These programs are often recommended to improve the quality of life. In this regard, the European Heart Failure Self-care Behavior scale (EHFScBS) has been presented to measure the self-care behaviors of HF patients.13The EHFScB-12 is a self-report scale that was designed for HF patients.14This scale has satisfactory psychometric properties and is a valid and reliable tool for measuring health behaviors in HF patients.15Considering the lack of a similar scale in Iran, and the need for a valid tool to determine self-care behaviors of HF patients in Iran, this study aimed to investigate the psychometric properties of the self-care behavior scale in HF patients.
2. Methods
This study is a descriptive study of psychometric and test validation. In this study, the validity and reliability of the EHFScBS were evaluated. Given that self-care was likely to be influenced by cultural differences,16-18the city of Tehran was divided by random method into the following regions: north, center, and south; and then from each region one hospital was selected randomly. Forty HF patients were randomly selected from each hospital to complete the questionnaire. The number of samples varied according to the analysis steps: 10 patients to determine the face validity and 120 patients to determine the construct validity (10 times the number of items in the final questionnaire).19Inclusion criteria were: (1) aged ≥18 years; (2) diagnosis of HF based on Framingham criteria (at least two major criteria or one major symptom with two minor symptoms); (3) pharmacologically stable with standard medication for HF. Exclusion criteria were (1) inability to complete the questionnaires; (2) incapable of understanding; and (3) reading Farsi and inability or unwillingness to give informed consent.20
The EHFScB-12 scale, which has one dimension and 12 items, has been developed and tested to measure the self-care behaviors of patients with HF. The scoring of this tool is on a 5-point scale from 1 (strongly agree) to 5 (strongly disagree). This questionnaire was developed by Jaarsma et al. in 2003,14and after evaluation of its psychometrics characteristics, it was introduced as a valid and reliable tool to measure behavior change over time. The demographic data sheet was used to assess age, sex, education, marital status, living with others, job, housing, walking, diet, smoking, and daily activity, and daily exercise. Daily activity was classified in two groups “without problem” and “troubled.” To evaluate the psychometric properties of the scale, face validity, content validity, and construct validity and reliability were evaluated. To evaluate face validity, the scale was provided to 10 members of nursing faculty with sufficient experience in designing tools and cardiovascular diseases, and they were asked to comment on the difficulty and clarity of the items, the appropriateness of the classification of responses, and the ease of completing the scale. After several steps of revising and making changes, a Persian scale was prepared for the research and Professor Jaarsma confirmed the final version, which is now available on her site. To determine the qualitative content validity, 5 experts with knowledge of and experience in the subject were asked to provide their detailed and written corrective views of the items in terms of language, appropriate words, relevancy, clarity, and simplicity.21To determine construct validity, exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were performed using SPSS (ver., 16). Cronbach alpha coefficient was used to determine the reliability of a scale with an emphasis on internal consistency. For a good internal consistency, Cronbach alpha was considered between 0.70 and 0.80.22For reproducibility, a scale was administered to 20 patients within 2 weeks, and the intra-cluster correlation coefficients (ICC) were calculated between the two-time steps. The reliability coefficient was 95% andP< 0.05 was considered significant. Kaiser-Meyer-Olkin (KMO) was calculated for sampling adequacy for EFA. Bartlett test for Sphericity was used to determine if correlations between items were sufficiently large for EFA. To verify that the test was saturated with several factors, Varimax rotation was used after performing principal components extraction. The scree plot with the eigenvalue ³1was used to determine the number of factors retained in EFA.
3. Results
In this study, the data of 120 HF patients were included in statistical analysis. The mean age of the samples was 67.3 ± 14.04 years (range: 30-92 years). Sixty-six (55%) were male and 54 (45%) were female. 82 (68%) were under the diploma. Housekeeping was the most frequent occupation (n= 39, 33.6%).Among the sample, 110 (91.7%) lived in private homes and the remaining were tenants (8.3%) (Table 1).
In the EHFScB-12 scale, responses to each item on the Likert scale ranged from 1 (strongly agree) to 5 (strongly disagree). The mean and standard deviation (SD) scores of the Persian version of EHFScB-12 are given in Table 2.
Face validity was checked through a panel of experts’ comments about the style of writing and the clarity. It should be noted that the content of the items was not changed and that the only changes made were editorial ones. Patients with HF did not report difficulty in response or interpreting items. The response time for the scale was 5 min. To determine the content validity of the scale, a form was prepared to examine its simplicity, transparency, and relevance. It would be acceptable if 80% of the participants considered it clear and simple. Davis proposes that researchers should consider ≥80% agreement among judges for new instruments.23EFA was used to evaluate the construct validity. Data from 120 subjects were analyzed on 12 items of EFA. The calculated value of KMO is 0.610 indicating the adequacy of the sample size selected for the factor analysis. Bartlett Spearman test (Chi-square value = 246.537,Pvalue = 0.000) indicates a non-zero correlation between the items and the ability of the scale to perform factor analysis and that a detectable relationship exists among the variables that were analyzed by factor analysis (Table 3). The second output shows the commonality of the variables based on principal component analysis and includes the value of initial and extraction amounts (Table 3).

Continued

Table 1. Demographic characteristics of patients.

Table 2. The mean and SD of the scores of the Persian version of EHFScBS.
Table 3 shows the extent to which the selected factors explain the variance of each variable. The first column lists commonalities before factor extraction. All initials are equal to 1. EFA showed that the calculated extraction ranged from 0.358 to 0.734 for all items, indicating the ability of the factors to explain the variance of the variables. The extraction coefficient of the first item is 0.46; this item can explain (0.46)2or 21% of the variance of the 4 factors (Table 4). The first 4 factors have an eigenvalue ³1. The variances of these factors were 20.68%, 15.94%, 11.35%, and 9.92%, respectively. In total, the 4 extracted factors account for 57.89% of the total variance of items (Table 4).

Table 3. Commonality of items.
The result shows that 4 factors were statistically significant and could be used for analysis and interpretation. Also, the scree plot shows that the first 4 factors account for most of the total variability in the data (Figure 1).
The rotated component matrix indicates the factors that were loaded on each item after rotation (Table 5). Factors’ naming was based on the commonality of variables with the larger factor loadings. In this study, factor loading was considered at ≥0.5. All 12 items of the scale had an acceptable factor load (≥0.5). Therefore, the scale has appropriate construct validity. The highest weights in the first factor were related to the items: I weigh myself every day (0.592); I contact my doctor or nurse if my shortness of breath becomes worse (0.826); and I get the flu vaccine every year (0.562). In the second factor, the following items had the highest weight: I contact my doctor or nurse if I gain 2 kg in a week; I contact my doctor or nurse if I feel very tired; and I exercise regularly. Similarly, in the third factor, the highest weight was found to be attributed to the following factors: I take time to rest during the day; I eat low-salt food; I take medication according to the physician’s order; and I restrict fluid intake (0.836). Items 6, 9, 10, 11, and 12: adherence to treatment; items 3, 4, 5, and 8: seeking help; and items 2 and 7 were designated as moderating activities. The sixth item was placed in one factor; however, based on its meaning this item was considered in “adherence to the treatment regimen”; as a result, 3 factors were identified. The internal consistency of the scale showed a Cronbach alpha of 0.72. The item “I get the flu vaccine every year” (α = 0.703) and “I contact my doctor or nurse if I feel very tired” (α = 0.861) had the highest and lowest reliability, respectively. To complete the retest, 22 scales were completed in 2 weeks. ICC were calculated between the two-time steps. The ICC was calculated at 0.69.
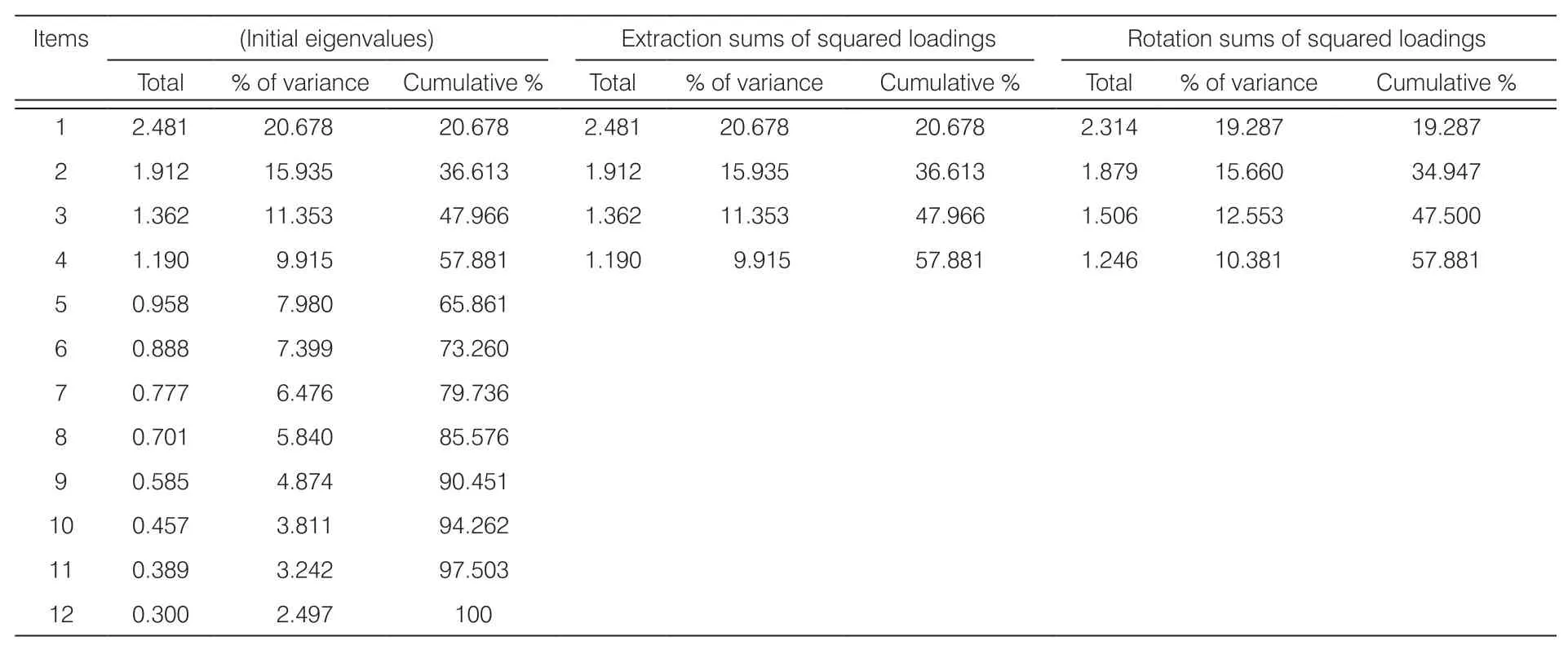
Table 4. The total of variance explained in the Persian version of self-care behavior questionnaire in patients with HF.
4. Discussion
The purpose of this study was to investigate the psychometric properties of the EHFScBS. This 12-item tool is rated on a 5-point scale from 1 (strongly agree) to 5 (strongly disagree). The total score is the sum of the items in the 12-60 range. The mean score of the Persian version was 34.43 ± 1.27. The mean score of the Brazilian version24of the tool was 24.7 ± 8.5 and in Turkish version25it was 34 ± 7.99. The mean score of our study is closer to the values presented by Baydemir (Turkish version) and Jaarsma (original version). Jaarsma determined the mean score of the EHFScBS at 33.3 ± 7.8.14. In the Japanese26and Spanish versions,27this value was reported at 32.6 ± 9.1 and 24.8 ± 7.6, respectively. However, the difference in mean score between these studies can be attributed to the differences in the patients’ characteristics and health conditions (i.e., illness severity or comorbidities). The internal consistency of the questionnaire showed a Cronbach alpha of 0.72 and the ICC was 0.69. Kato et al.26reports a Cronbach alpha of 0.71 and a Kappa coefficient between 0.33 and 0.87 in the Japanese version of the questionnaire and cites it as satisfactory. In the psychometric evaluation of the Brazilian version of EHFScBS, the Cronbach alpha was 0.70 and the ICC was 0.87.24Baydemir et al.,25in the Turkish version, reported a Cronbach alpha of 0.69. In her original (2003) version of the tool, Jaarsma developed and tested the scale on 442 patients in 2 centers in Sweden, 3 in the Netherlands, and 1 in Italy. The Cronbach alpha was 0.81. She classified the 12 items into 3 subscales through EFA . The first subscale, diet adherence (6 items) (α = 0.81); the second subscale, seeking help (4 items) (α = 0.81); and the third subscale, adaptation of activities (2 items) (α = 0.81).14Scale evaluation in the United Kingdom by Shuldham et al.28showed that internal consistency is moderate (Cronbach alpha 0.69). Pulignano et al.29showed a Cronbach alpha of 0.82 in the Italian version of EHFScBS. In the Chinese version, Cronbach alpha was 0.82 and all items (except for the item, I rest during the day) had a score >0.30, indicating homogeneity in measuring self-care in patients with HF.30In this study, reliability was evaluated by comparing patients’ responses in two-time points. However, Jaarsma et al.14only examined the consistency between questionnaire items in their initial study. Estimates regarding reliability are different due to varied demographic characteristics and time intervals allocated for answering the questionnaires. Although the alpha coefficient in this study was lower than the value in the original version (i.e., 0.81), it is within an acceptable range. The results show a good reliability in the instrument for self-care assessment in Iranian HF patients, similar to the findings of other related studies.

Figure 1. Screen plot diagram.

Table 5. Rotated component matrix.
In this study, the questionnaire was provided to 10 expert members in instrumentation and cardiac nursing. Subsequently, changes were made to items in accordance with the Iranian socio-cultural context, and these changes were notified and approved by Professor Jaarsma. Some members of the expert panel stated that patients with a history of hospitalization would come to the health center and call the nurse for advice. But in general, physicians do not provide patients personal contact numbers. This implies that most patients would be unable to get in touch with their physicians. It is in any case a nurse or a physician who must respond to the patient’s needs. Therefore, the item “contact with a doctor or nurse” was retained in the analysis. The title “I restrict fluid consumption to 1.5-2 L/d” has been changed to “I restrict fluid intake to <6-8 glasses a day”; because Iranian people don’t use the liter unit for drinking water/liquids. Also, this change was approved by Professor Jaarsma. Likewise, there have been changes to the articles while translating into other languages. For example, in the Chinese version, since patients do not have access to a specific physician or nurse, the item “I consult a physician or get advice from a nurse” was substituted for “I call my doctor or nurse”. In the same way, in the Brazilian version, the item “I call my doctor or nurse” has been replaced by “I am going to seek medical help.” In this study, patients had no problem answering the questionnaire, in terms of not having enough time to complete the items. Kato et al.,26in examining the face validity of EHFScBS in a pilot study on 5 patients, found that they had no problem answering or understanding the items. The response time for the Japanese version of the questionnaire was approximately 5 min.26In the Chinese version, the mean duration of the questionnaire was 4-6 min,30and in the Brazilian version, it was reported to be 10 min.24The results of EFA in this study showed that all items explain the variance of the studied variables. Kato et al.26reported a single-factor questionnaire in their analysis of the Japanese version of the scale. Kato measured Spearman rank correlation coefficient between the Japanese version of the EHFScBS and the Self-Care Agency Questionnaire (SCAQ) subscale. Yu (2010) conducted a confirmatory factor analysis based on the hypothesis that the EHFScBS has a 3-factor structure for measuring self-care behaviors (diet adherence, seeking help, and adjusting activities) and also used the Chinese version of medical outcomes study social support survey. Jaarsma et al.14divided the 12 items into 3 subscales. The first subscale, diet adherence, measures behaviors related to daily weighing, water and sodium restriction, medication adherence, influenza prevention, and exercise. The second subscale, seeking help, comprises the behaviors that the patient performs in response to an increase in the symptoms of HF. The third subscale, adaptation of activities, measures the adaptation of behaviors to the limitations caused by HF. Shuldham et al.28and Baydemir et al.25present “adherence to treatment,” “adherence to activities,” “adherence to recommendations,” and “seeking help” as the subscales of the EHFScBS. In the study of Yu et al. (2010), 3 subscales were developed, namely “adherence to treatment,” “adaptation of activities,” and “seeking help.” However, these minor differences may be due to cultural differences between the communities studied. Shuldham et al.28showed the 4 components accounted for approximately 60% of the variance. These 4 components were examined for similarities and differences between items to identify items within the questionnaire. Calling a doctor or nurse because of weight gain (0.731), shortness of breath (0.702), swelling of the legs (0.663), and fatigue (0.691), had the highest weight for the first component content. Examination of the items in the second component showed that there are similarities between items related to patient behavior, such as taking medication (0.661), resting during the day (0.510), and taking the illness seriously (0.459), and seeking help from others for shortness of breath (-0.111), leg swelling (-0.118), and fatigue (-0.354). Overall, the findings showed that although the questionnaire had some correlated responses, no distinct items could be identified. The component analysis showed that the 3 conceptually explored themes were clearly identifiable; so, the total score should be used in the English version of the questionnaire, as in the Dutch and Swedish versions presented by Jaarsma et al.14Recently, a new version of this questionnaire has been developed by its creators, in which 3 items, namely “I rest if I feel shortness of breath,” “I rest during the day,” and “I get the flu vaccine annually,” have been removed. The authors conclude that these behaviors are followed by a progression of the disease or worsening of symptoms and do not indicate the better ability of patients to self-care. In addition, they argue that influenza vaccination is not a specific self-care measure for HF. In the Brazilian version, the scores of these items were similar to those in the original study and did not pose a problem for the questionnaire. In the Brazilian version, items related to “resting” do not indicate better self-care ability, but vaccination against influenza was presented an important self-care behavior.
In the present study, the KMO indicate the adequacy of the sample size for the factor analysis. Bartlett test showed that the correlation between the items of EHFScBS is not zero and that factor analysis can be done for this questionnaire. In the study of Yu et al. (2010), the KMO was 0.96 and the Bartlett sphericity test was significant (P< 0.001). In Baydemir’s study25, the KMO was 0.59 and Bartlett test was significant (P< 0.001, chi-square = 1554.84).
As we see in our findings, the first 4 factors explain a higher percentage of variance. In the context of Iranian HF patients, it seems that many of these patients mainly pay attention to HF management programs in daily weight, take shortness of breath seriously, contact the physician in case of shortness of breath, and follow up with medical and nursing care in case of swollen legs. In any case, attention to fluid intake, low-salt diet, medication adherence, physical tiredness, rest, the use of influenza vaccine, and exercise are the next priorities in self-care in patients with HF. This finding brings out the fact that many Iranian HF patients don’t have a good perception and knowledge of the importance of all aspects of self-care for their chronic disease; thus, in the training provided to these patients, more emphasis is required to be placed on some aspects of self-care. However, all these factors have the same weight to better control and prevent the progression of HF.
5. Conclusions
EHFScB-9 is a self-reported questionnaire commonly used to assess the self-care behaviors of HF patients. Our findings suggest that the Persian version of EHFScBS can be a valid and reliable scale for Iranian HF patients. This questionnaire can be used to assess patients’ needs and to evaluate the effectiveness of HF management programs. A small number of items, quick response, and there being no need to teach the patient to complete the questionnaire are advantages of this tool. This tool can be used to address treatment and care deficiencies based on the needs reported by HF patients. The Persian version of the HF self-care scale would prove beneficial to nurses and clinicians since it would enable them to ensure rapid assessment of selfcare behaviors. So, we can expect reduced readmission, attenuated costs, and improved quality of life in HF patients and their families. Finally, the authors recommend further research on self-care behaviors and the design and development of assessment tools in outpatient units for patients with HF. Also, cardiac rehabilitation facilities and palliative care centers can use the Persian version of EHFScBS to identify the self-care needs of HF patients, which would enable constructive modifications and improvements to be carried out in their treatment programs.
Acknowledgments
We convey our thanks to the Research Ethics Committee of Shahed University for approving this research. Also, we appreciate all patients who completed the questionnaire.
Ethical approval
The study was approved by the Research Ethics Committee of Shahed University (IR. Shahed. REC. 1394.118).
Conflicts of interest
None of the authors disclose any potential conflict of interest.

- Frontiers of Nursing的其它文章
- Frontiers of Nursing Call for Papers
- Common psychological disorders in elderly and their correlations with social support, Shiraz, Iran, 2018†
- Development and psychometric evaluation of the nurse behavior toward confirmed and suspected HIV/AIDS patients (NB-CSHAP) scale
- Experiences of implementing a coping mechanism for the elderly who face chronic diseases while living with the family: a phenomenology study
- Person-job fit and work-life balance of female nurses with cultural competence as a mediator: evidence from Nigeria
- Effects of the self-management training program on self-management behavior and blood pressure levels among elderly people with hypertension