
Common psychological disorders in elderly and their correlations with social support, Shiraz, Iran, 2018†
2022-03-31 07:00FiroozehAsiSeyyedMnsourKshfiHosseinAliNikkhtMsoudKrimi
Frontiers of Nursing 2022年1期
Firoozeh Asi, Seyyed Mnsour Kshfi, Hossein-Ali Nikkht, Msoud Krimi,*
aDepartment of Health Promotion, School of Health, Shiraz University of Medical Sciences, Shiraz, Fars 7134814336, Iran
b Research Center for Health Sciences, Institute of Health, Department of Public Health, Shiraz University of Medical Sciences, Shiraz, Fars 7134814336, Iran
c Department of Biostatistics and Epidemiology, Faculty of Medicine, Social Determinants of Health Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Mazandaran 4717647745, Iran
Abstract: Objective: To recognize and screen common mental disorders in elderlies and determine their relationship with social support in Shiraz, Iran.Methods: In this cross-sectional analytical study, 400 elderlies aged >60 years from Shiraz were selected through stratified random sampling. Data collection was done by 3 demographic data, Medical Outcome Study (MOS), social support, and standardization of mental disorders symptoms checklist 90 (SCL-90) questionnaires. The collected data were analyzed with SPSS 22, using descriptive statistics, Pearson correlation coefficient, and univariate and multivariate linear regression analyses. A P value <0.05 was regarded as statistically significant.Results: A total of 400 elderlies (mean age = 67.39 ± 6.89), among whom 204 individuals were female (51%), participated in the study. Somatization and phobic anxiety were the most (68.9%) and least (14.2%) prevalent disorders, respectively. The average total score of social support was 85.59 + 3.5. Social support and its 5 subscales showed statistically significant negative correlation with SCL-90 total scores and its 9 domains (P < 0.05). A 1-point increase in social support score results in reduction in the psychological disorders score by 0.35 point (P < 0.001).Conclusions: It seems necessary to plan and make policies by the authorities to increase social support and reduce the burden of common mental disorders in the elderly.
Keywords: elderly · psychological disorders · mental health · aging · SCL-90 © Shanxi Medical Periodical Press.
1. Introduction
The aging phenomenon is considered as one of the important economic, social, and public-health challenges for healthcare service providers, family members, and the community in recent years.1,2The World Health Organization (WHO) has estimated that the population of elderlies in the world will increase to 1100 million in 2025; for comparison, in 1975, the same figure amounted to 350 million.3Based on the last national census in Iran, Iranian elderly were 9.27% of total population and the percentage of elderly population in Shiraz, which is located in southwestern Iran, was 9.81%.4
A set of changes such as the loss of power, life purposes, physical skills, and social position and death of close relatives can occur in elderly life more than in other age groups. Further, the fact of approaching the final days of life and impending death places double pressure on elderly individuals, and increases the possibility of physical and mental diseases.5
Mental disorders such as depression, anxiety, and drug abuse are considered as the most prevalent disorders among elderly people.6,7In the DSM-5, mental disorders are defined as a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning.8
Psychological disorders promote the possibility of physical and mental diseases in the elderly.9Although 14% of the world’s population suffers from psychological disorders, the prevalence of these disorders is increasing in the elderly.6,9In some studies, the prevalence of these disorders was reported as >60% in the age group of ≥60 years in Iran.10
In situations where older adults lose control over their environment due to the lack of independence and autonomy, and inability to perform daily activities, psychological disorders can increase rapidly. Some researchers put forth the view that social support is considered as a main factor for determining different dimensions of health and a parameter for increasing the quality of life.11In the elderly, social support can play an important role in reduction of physical, mental, and cardiovascular diseases,12,13and in improving the quality of life.11The lack of social support and limited social relationships may cause an increase in mental disorders.14
Social support is regarded as a type of awareness in which the individual believes in his respectability, value, and dignity, and depends on a network of mutual communications and commitments.15Perceived social support or individual perception about the amount of support which can be received, when needed, from friends, relatives, and family, is regarded as the most important element of social support.16Social support results in sensing tranquility, security, and comfort by individuals during stressful situations.17,18Kim et al.19introduced social support as a more effective method that helps individuals to deal with problems and stressful issues.
Since no previous studies were conducted in this regard on the elderly population in Iran, the present study sought to recognize and screen for common psychological disorders in the elderly population and determine the relationship of these disorders with the elderlies’ perceived social support.
2. Materials and method
2.1. Methodology
The present descriptive study was conducted among the elderly aged >60 years, individuals under the coverage of Shiraz health centers during 2018. Considering the 50% prevalence of psychological disorders in previous studies, the required sample size was estimated at 384 (α = 0.05,d= 0.05). Then, the sample size increased to 400 individuals due to the special conditions of the period of old age and the possibility of responding to questionnaires imperfectly. Stratified random sampling was used as the sampling method, in which Shiraz was divided into 3 regions; then, 10, 8, and 11 health centers were selected in each region based on the population under coverage, and finally, 16 elderlies (preferred 8 males and 8 females) were randomly selected in each health center. The inclusion criteria were community dwelling elderlies aged >60 years who had the cognitive ability to respond to questions, and signing an informed consent form, while the exclusion criterion was providing an incomplete response to the questionnaire.
Elderly people were invited by telephone during a specific temporal range. After assessing the inclusion criteria, an informed consent form was signed by participants, and tools were completed through interviews in the standard places, which were arranged in health centers.
2.2. Instruments
Our data collection tool consisted of 3 sections. The first section involved the demographic characteristics of individuals, such as age, gender, educational level, and other similar elements, and was collected by using a researcher-made demographic questionnaire.
As for the second section, it aimed to gather information concerning the mental symptoms of the participants, and the symptoms were assessed by using a standardization of mental disorders The Symptoms Check-List-90-Revised (SCL-90-R) standard questionnaire, which was introduced by Derogatis and Cleary.20This questionnaire includes 90 questions, of which 83 questions are related to 9 dimensions of somatization (12 items), obsessive-compulsive behavior (10 items), interpersonal sensitivity (9 items), depression (13 items), anxiety (9 items), hostility (6 items), phobic anxiety (8 items), paranoid ideation (6 items), and psychoticism (10 items); and the remaining questions failed to incorporate these dimensions, although they are considered as important clinically and help the general indexes of the test. Questions are scored on a 5-point discomfort scale from 0 to 4. Dragonish et al.20reported that the Chronbach alpha of this questionnaire was 0.74. According to Anis et al.,21the Chronbach alpha of the standardization of mental disorders The Symptoms Check-List-90 (SCL-90) tool among the Iranian population was determined as 0.98.
The Medical Outcome Study (MOS) social support scale, introduced by Sherburne and Stewart,22was utilized in the third section to evaluate the amount of received social support. This tool involves 19 items and 5 subscales of the tangible support which measures financial and behavioral assistance (4 items), emotional support assessing positive affection, sympathy, and encouragement for the expression of emotions (4 items), informational support which evaluates guidance and provision of information or feedback (4 items), affectionate support measuring the expression of love (3 items), and positive social interaction which assesses engaging in recreation activities (4 items). Questions are scored on a 5-point Likert scale from 1 to 5. The possible score is considered between 19 and 95 and higher scores represent greater social support. The Chronbach alpha values pertaining to the constructs of this questionnaire were 0.91 and 0.96 in the studies of Sherburne and Stewart22and Mohammadzadeh and Sayehmiri,23respectively.
2.3. Data analysis
The collected data were analyzed with SPSS 22. After confirming the normality of data, the characteristics of participants were reported in descriptive statistics. Pearson correlation coefficient was used to assess the correlation between the dimensions of psychological disorders and social support. Univariate and multivariate linear regression analyses (to control confounding variables) were used for the separate assessment (raw effects) and simultaneous assessment (comparative effects) of the anticipating variables and social support as independent variables on psychological disorders as dependent variables and their relationship. Regression coefficients and their 95% confidence interval were provided in this analysis. APvalue <0.05 was regarded as statistically significant.
3. Results
Based on the results in the present study, the statistical population included 400 elderlies (mean age = 67.39 ± 6.89), among whom 204 individuals were female (51%) and the rest were male (49%). In addition, 93.2% of the participants lived with their families while 6.8% lived alone. Other demographic characteristics of participants are summarized in Table 1.
Regarding reported underlying diseases, the maximum and minimum values of prevalence were obtained in metabolic disorders (55.8%) and disorders of the immune system (9.3%), respectively.
Table 2 represents the prevalence of psychological disorders in elderlies and the mean score of SCL-90 questionnaire dimensions, in which somatization and phobic anxiety were determined as the most (68.9%) and the least (14.2%) prevalent disorders, respectively. Cutting points are based on the study of Bagheri et al.,24which was conducted on 101 Patients with Behcet Disease in Shiraz.
The average total score of social support was 85.59 + 3.5. Table 3 represents the mean (SD) of the 5 subscales of perceived social support.
Based on a correlation analysis of the 9 dimensions of the SCL-90 questionnaire and the related social support subscales (Table 4), the dimensions of somatization, obsessive-compulsive behavior, interpersonal sensitivity, depression, anxiety, phobic anxiety, paranoid ideation, and psychoticism were determined to be inversely and significantly related to all the social support subscales.

Table 1. Demographic profile of participants (n=400).
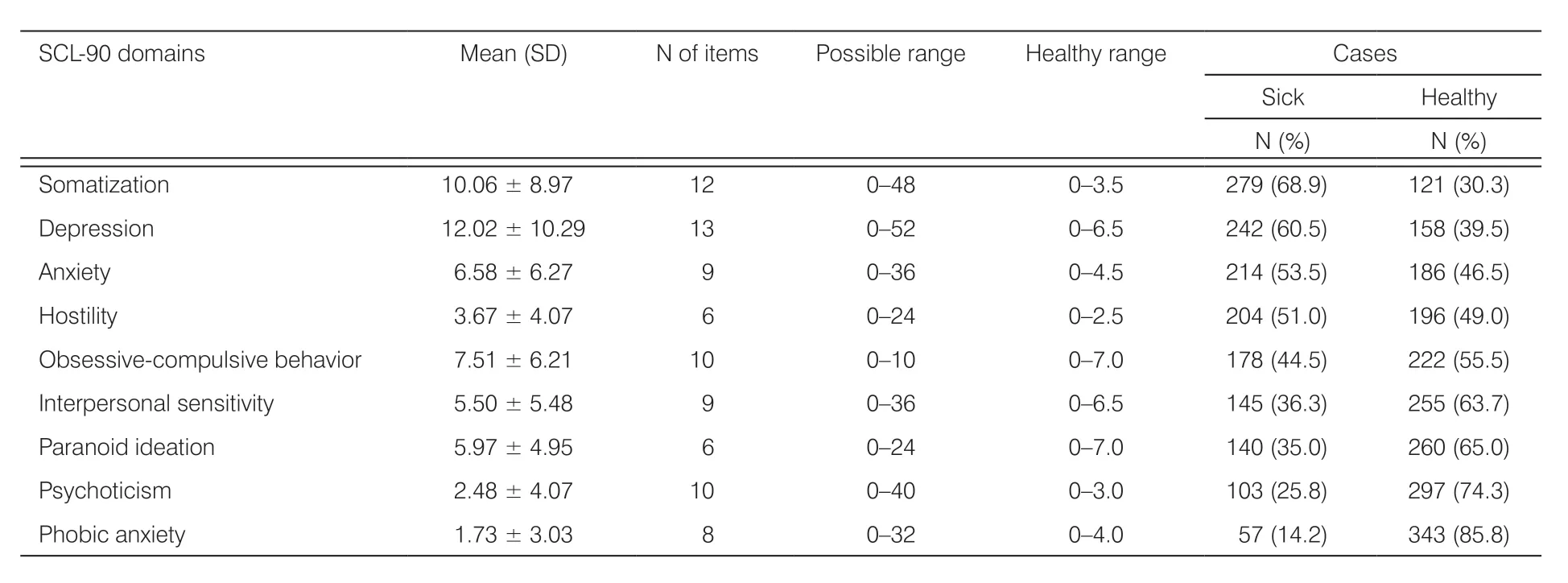
Table 2. The mean scores of SCl-90-R dimensions and frequency of participants’ psychological disorders.
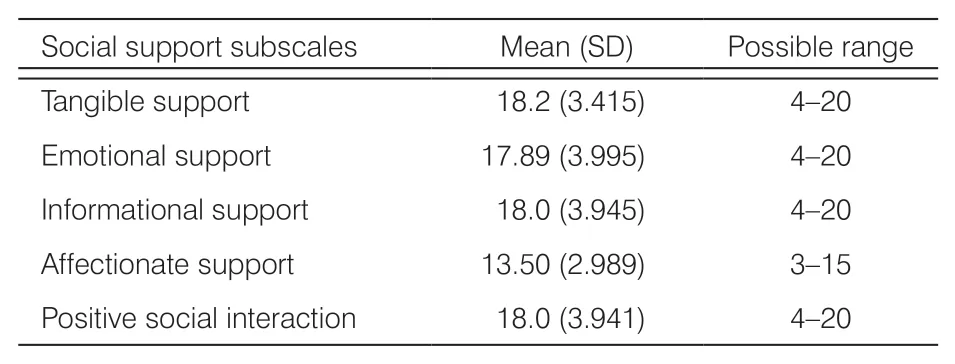
Table 3. Mean (SD) scores of social support subscales.
The relationships between psychological disorders and social support and demographic variables are presented in Table 5 using univariate linear regression. Regarding the assessment of relationship between social support and psychological disorders, a 1-point increase in the social support score results in a reduction in the psychological disorders score by 0.35 point (P< 0.001). Further, social support is inversely related to psychological disorders, which implies that individuals with greater social support possess fewer mental problems. Regarding demographic variables, the score of psychological disorders in females was 0.21 point higher compared to that in males (P< 0.001). Further, the score of psychological disorders in literate and married individuals were obtained, and were ascertained to be 0.067 (P= 0.182) and 0.128 (P= 0.01) point lower than that in non-literate and single individuals, respectively. Furthermore, the individuals earning $270 monthly possessed lower psychological disorders (0.137 point) compared to those having less monthly income (P= 0.006). No significant relationship was observed between psychological disorders and age, smoking, chronic disease, or educational level.
In multivariate linear regression, a 1-point increase in social support resulted in the decrease of psychological disorders by 0.332 point (P< 0.001). Gender and psychological disorders were correlated based on multivariate regression, which is inferred from the fact that psychological disorders were 0.13 point greater in females compared to males. These findings were consistent with the results of univariate regression. Based on multivariate analysis, a significant relationship was not observed between psychological disorders and age, marital status, chronic diseases, education level, or income (Table 6). So, the variables of social support, gender, and smoking were recognized as independent and potent predicting variables of psychological disorders.
4. Discussion
Regarding the period of old age, multiple stressful issues such as various diseases, lack of spouse, and loss of job can endanger the mental health of the elderly. Based on our findings, in the Iranian elderly, the prevalence of various psychological disorders differs from 32.4% to 74.9%.25Researchers believe that social support influences positively on preventing a reduction of the individual’s quality of life, which is regarded as being more important in the period of old age.9,26
Tajvir et al.,9in a study among 644 elderlies in Tehran, discovered that the health of the elderly receiving moderate and high social support were 3.8 times higher compared to that of individuals failing to receive adequate social support. Based on the results of the present study, on average, a 1-point increase in the score of social support decreases the score of psychological disorders by 0.2 point. Wedgeworth et al.26conducted a study among rural elderly with the inclusion criterion of attaining at least 45 scores in the SCL-90 test, and the psychological disorders of the elderly were related to social support (β = 0.09). Further, they found that demographic variables such as marital status and educational level could anticipate psychological disorders.26According to Harandi et al.,27receipt of higher social support by the elderly led to an increase in their mental health. In fact, the addition of social support resulted in increasing mental health and physical performance simultaneously.28However, social support differs from social participation, which plays a supporting role in the mental health of the elderly.29Moatamedy et al.30found that social support increased mental welfare due to better stress management. Wedgeworth et al.26mentioned the moderating role of social support on the relationship between the psychological disorders in, and the life quality of, the elderly. Researchers believed that the network of friends and family members were to be regarded as the most important protective factor for mental and personality disorders.31
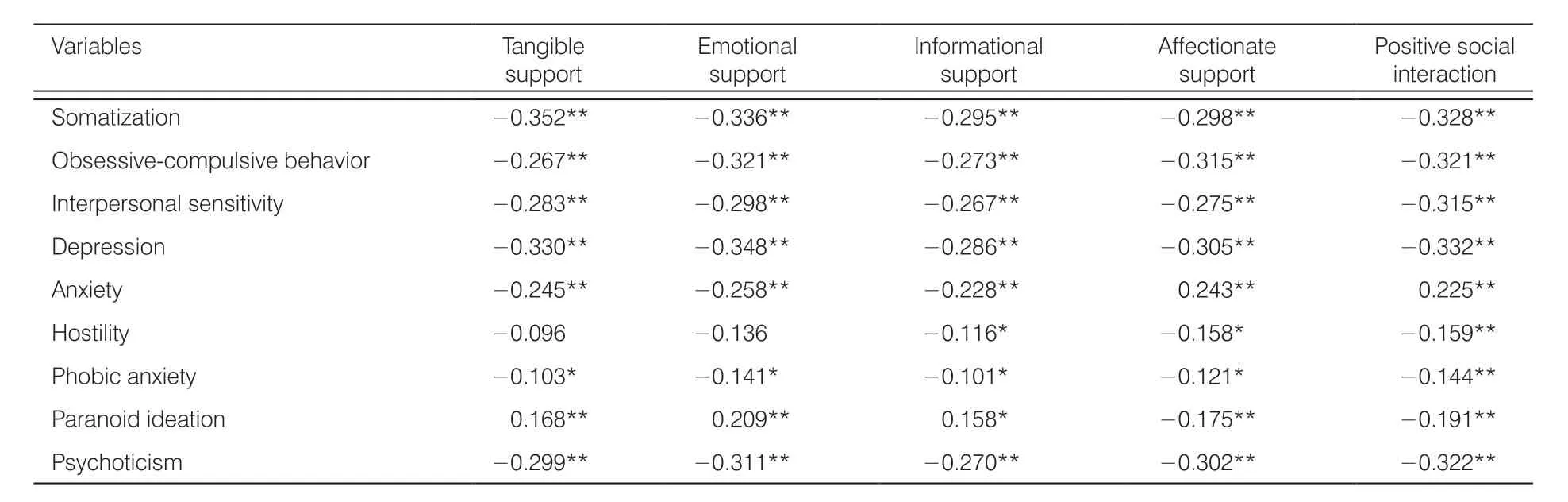
Table 4. Correlation coefficients of SCL-90 domains and social support subscales.
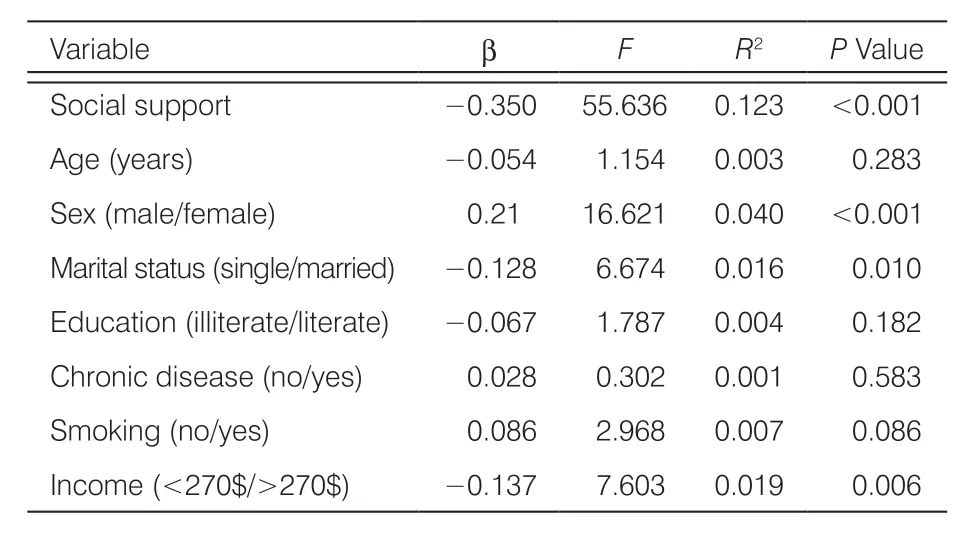
Table 5. Associations between SCL-90 total score and social support and demographic variables in univariate linear regression.
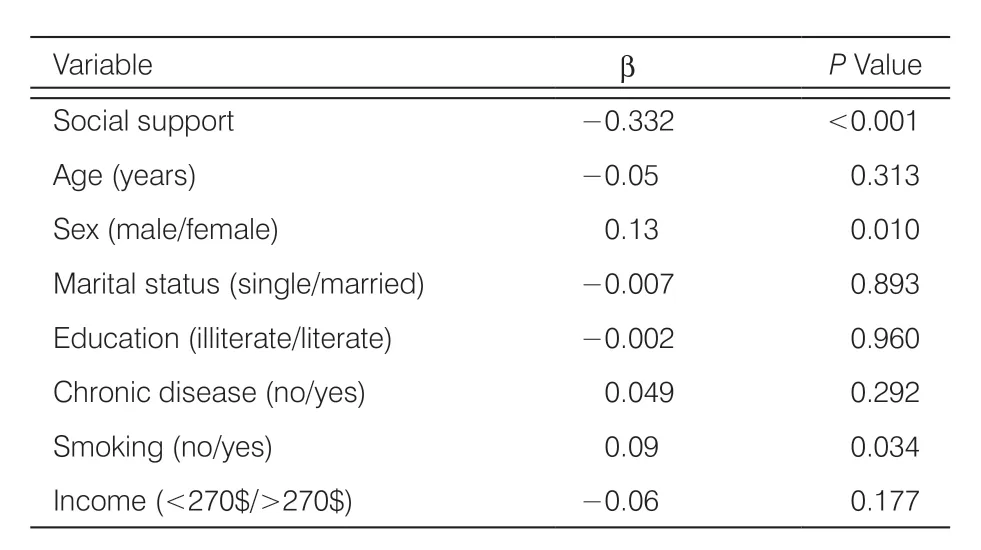
Table 6. Associations between SCL-90 total score and social support and demographic variables in multivariate linear regression.
Although the present study was conducted among elderlies living in the community, other studies espoused the view that the importance of social support is not limited to the elderly living in the community, and it was considered as important for those living in a nursing house and having less social relationships as well.32,33According to Nickbakht et al.,33among older adults living in a nursing house, the minimum life satisfaction was related to the shortage of social relationship. In another study, social support (emotional, informational, instrumental, and financial support) significantly affected the mental and social health of the elderly living in a nursing house.34Social support played an important role during disease. In addition, the individuals who had a stroke and received lower social support were more depressed in comparison with others.35
Thus, the results of the present study, conducted among Iranian elderly with Islamic culture, are consistent with those of previous studies and emphasizes the relationship between the social support received by, and the mental health of, the elderly. Assessing the prevalence of different psychological disorders in the elderly and their relationship with the amount and various dimensions of social support is considered as one of the advantages of the present study, an aspect which was less discussed in previous studies.
5. Conclusions
The prevalence of psychological disorders is becoming more obvious in the increasing elderly population in Iran. Since social support as a preventive factor results in reduction in mental disorders, it is essential to increase the amount of social support in the elderly and improve their spirit and quality of life through various methods such as enhancing participation in religious activities and regularly practicing physical exercises in the period of old age. Based on the results of the present study, it is suggested that future studies can focus on females and smokers among older adults, who are at higher risk of psychological disorders.
Limitations
The results are limited to Iran’s urban area and cannot be generalized to rural areas. Further, the elderly living in the community were the ones primarily taken into consideration in the present study. Thus, it is suggested that further assessments be conducted among elderly with special conditions, such as those living in a nursing house.
Acknowledgments
The study was approved by Shiraz University of Medical Sciences Ethics Committee. The authors would like to thank all elderlies who participated in the study, and the health deputy of Shiraz University of Medical Sciences, for their cooperation in this study.
Ethical approval
Ethical issues are not involved in this paper.
Conflicts of interest
None of the authors disclose any potential conflict of interest.

- Frontiers of Nursing的其它文章
- Application of a perioperative nursing strategy in the surgical treatment of elderly patients: a narrative review†
- Relationship between effort-reward imbalance, job satisfaction, and intention to leave the profession among the medical staff of Qom University of Medical Sciences†
- Inter-Professional-Compassionate pain management during endotracheal suctioning: a valuable lesson from a Chinese surgical intensive care unit
- Evidence-based practice profiles of nurses: a transcultural study†
- Identifying the core competencies of backup nurses in the acute care hospital through a modified Delphi process†
- Undergraduate nursing students’ experiences of online learning: gaining access in resource-limited circumstances†