
Recent advances in the diagnostic evaluation of pancreatic cystic lesions
2022-03-16 06:22:20DevarshiArdeshnaTroyCaoBrandonRodgersChidiebereOnongayaDanJonesWeiChenEugeneJKoaySomashekarKrishna
Devarshi R Ardeshna,Troy Cao, Brandon Rodgers, Chidiebere Onongaya, Dan Jones, Wei Chen, Eugene JKoay, Somashekar G Krishna
Abstract Pancreatic cystic lesions (PCLs) are becoming more prevalent due to more frequent abdominal imaging and the increasing age of the general population. It has become crucial to identify these PCLs and subsequently risk stratify them to guide management. Given the high morbidity associated with pancreatic surgery,only those PCLs at high risk for malignancy should undergo such treatment.However, current diagnostic testing is suboptimal at accurately diagnosing and risk stratifying PCLs. Therefore, research has focused on developing new techniques for differentiating mucinous from non-mucinous PCLs and identifying high risk lesions for malignancy. Cross sectional imaging radiomics can potentially improve the predictive accuracy of primary risk stratification of PCLs at the time of detection to guide invasive testing. While cyst fluid glucose has reemerged as a potential biomarker, cyst fluid molecular markers have improved accuracy for identifying specific types of PCLs. Endoscopic ultrasound guided approaches such as confocal laser endomicroscopy and through the needle microforceps biopsy have shown a good correlation with histopathological findings and are evolving techniques for identifying and risk stratifying PCLs.While most of these recent diagnostics are only practiced at selective tertiary care centers, they hold a promise that management of PCLs will only get better in the future.
Key Words: Pancreatic cystic lesion; Intraductal papillary mucinous neoplasms; Mucinous cystic neoplasm; Microforceps biopsy; Radiomics; Confocal laser endomicroscopy
INTRODUCTION
Pancreatic cystic lesions (PCLs) are increasingly detected, largely due to advances in imaging techniques and the increasing age of the general population[1 ]. With prevalence estimated in the range of 4 %-14 % in the general population and increasing constantly, it has become essential to characterize and risk stratify these cysts to guide management[2 ]. Current guidelines for evaluating PCLs are limited to less than optimal diagnostic techniques, resulting in either missed detection of early cancer or surgical over-treatment (see Figure 1 ). Resection of PCLs should be extremely selective since pancreatic surgery generally has a 20 %-40 % morbidity rate and an approximate 2 % mortality rate[3 -5 ]. Therefore, research and utilization of safe and effective diagnostic modalities with high accuracy are needed to evaluate cysts and introduce properly timed interventions.
Addressing this issue is especially relevant for intraductal papillary mucinous neoplasms (IPMNs), a type of PCL with one of the highest risks for malignancy. Of the two IPMN subtypes, main duct IPMNs are reported to have a risk from 38 % to 68 %and branch duct IPMNs from 12 % to 47 %[6 ]. Substantial research has addressed the use of consensus guidelines for evaluating IPMNs, but all mention that significant areas of improvement is imperative[7 -9 ].
Current standards for the evaluation of cyst morphology include computed tomography (CT) scan, magnetic resonance imaging (MRI), and endoscopic ultrasound (EUS). Fine needle aspiration (FNA) of cyst fluid for carcinoembryonic antigen (CEA) and cytology is performed during EUS. Considerable heterogeneity exists among the five widely used guidelines, which indicate a lack of standardization in diagnostic workups[7 -12 ]. In terms of the target population, American College of Gastroenterology and European guidelines include all PCLs, American College of Radiology guidelines focus on incidental PCLs, Fukuoka guidelines only focuses on IPMNs and American Gastroenterological Association (AGA) includes all PCLs except main-duct IPMNs. Guidelines differ in recommending evaluation with EUS and EUSFNA, and surgical resection. Multiple studies have compared some of these guidelines for identifying high-risk PCLs. Amongst patients who underwent surgery, the current guidelines directed clinical decision with an accuracy, sensitivity and specificity of 49 .6 %, 23 .5 %, 84 .3 % for 2015 AGA guidelines, 41 .2 %, 39 .7 %, 43 .1 % for revised Fukuoka guidelines and 58 %, 67 .7 %, 45 .1 % for 2018 European guidelines[13 ].
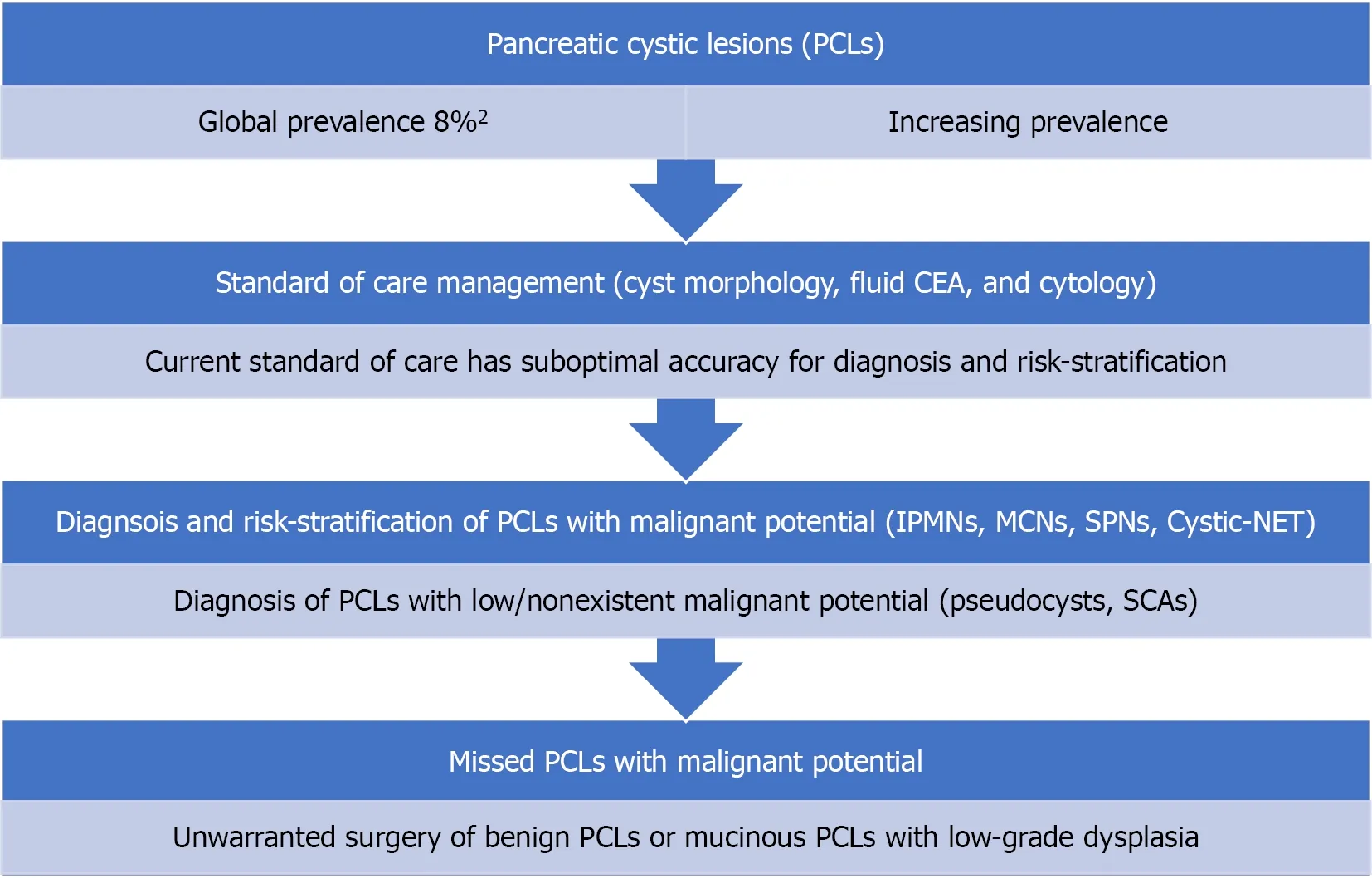
Figure 1 Current standard of care diagnostic methods are suboptimal in the diagnosis of specific types of pancreatic cystic lesions and risk-stratification of mucinous cysts. PCL: Pancreatic cystic lesion, CEA: Carcinoembryonic antigen, IPMN: Intraductal papillary mucinous neoplasms, MCN:Mucinous cystic neoplasm, SPN: Solid pseudopapillary neoplasm, Cystic-NET: Cystic neuroendocrine tumors, SCA: Serous cystadenoma.
A better understanding of investigational characteristics that lead to malignancy is necessary to improve existing criteria and accurately determine associated risks(Figure 1 ). While cyst fluid glucose has reemerged as a potential biomarker, novel techniques such as cyst fluid molecular analysis, EUS-guided needle-based confocal laser endomicroscopy (EUS-nCLE) and microforceps biopsy (EUS-MFB) have been introduced. The aim of this review is to provide an update of the recent literature in the management of PCLs with an emphasis on novel diagnostic methods.
RADIOMICS
Increasing prevalence of incidental PCLs has placed significant pressure on the necessity of discerning low-risk and high-risk lesions identified in radiological images.Radiomics is the analysis of mathematically derived textural features from crosssectional imaging studies. The features are generally beyond human visual perception.Using radiometric feature extraction tool, radiomics can quantify individual pixels and their associated gray-scale value from cross-sectional imaging in a temporal and spatial plane to create a cyst impression. While studies have varied in the extraction of radiometric data, these features can potentially risk stratify PCLs. Hence, radiomics can guide downstream invasive diagnostics.
Studies in radiomics can be classified into two broad categories: (1 ) Differentiating types of PCLs, and (2 ) Risk stratification of IPMNs. Investigators have applied machine learning algorithms to radiomic features for automatic classification of PCLs.Some recent studies have evaluated nomograms and algorithms combining radiomics,cyst morphology, and clinical features. For differentiating PCLs, several investigations have demonstrated promising results. One of the first studies by Dmitrievet al[14 ],achieved a reasonable accuracy of 83 .6 % in discriminating PCL types into IPMNs,mucinous cystic neoplasms (MCNs), serous cystadenoma (SCAs) and solid neoplasms[14 ]. Their model had 93 .2 %-95 .9 % accuracy at predicting IPMNs. Subsequently, three investigations utilized CT-Scan radiomics to differentiate serous cystadenomas from other PCLs (area under the curve (AUC) 0 .77 -0 .99 , sensitivity 69 %-95 %, specificity 71 %-96 %)[15 -17 ]. In one of these studies, radiomics outperformed radiologic characteristics in differentiating MCNs and macrocystic SCAs; comparative diagnostic parameters included sensitivity (93 .6 % vs 74 .2 %), specificity (96 .2 % vs 80 .8 %) and accuracy (94 .7 % vs 77 .2 %), respectively[16 ]. Combining radiomics with radiological findings or clinical parameters significantly improved the accuracy to distinguish cyst types in comparison to radiomics alone (P< 0 .05 ) [16 ,18 ].
Only a few studies have evaluated the role of radiomics in differentiating IPMNs with advanced neoplasia, from indolent lesions with low-grade dysplasia (Table 1 )[19 -23 ]. Most of the studies evaluating radiomics in IPMNs have used CT scans, and included patients with confirmed surgical histopathology as ground truth. A recent study by Cuiet al[24 ], presents the first publication where a radiomic signature incorporating 9 features was combined with clinical variables to predict high-grade dysplasia or adenocarcinoma (advanced neoplasia) in branch duct-IPMNs. Their predictive nomogram diagnosed advanced neoplasia with AUC values of 0 .903 (training cohort; sensitivity 95 %, specificity 73 %), and 0 .884 (one of two external validation cohorts; sensitivity 79 %, specificity 90 %)[24 ].
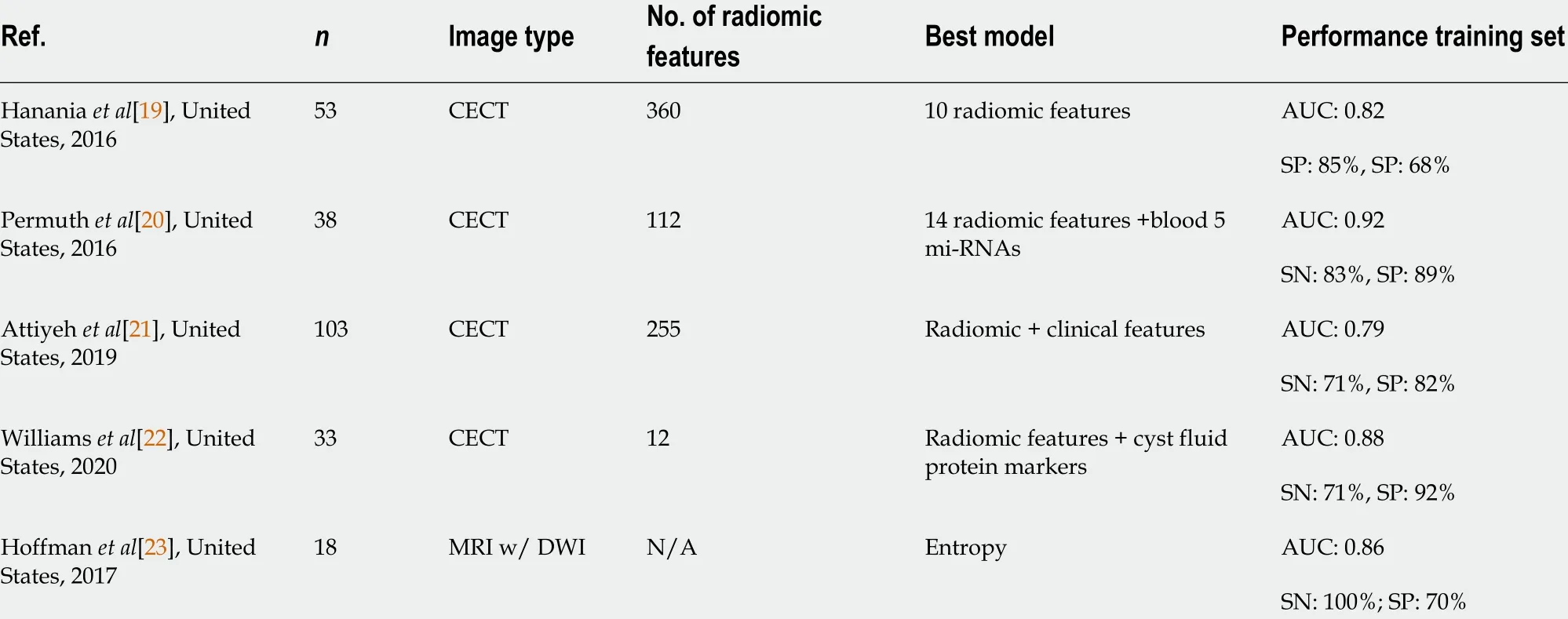
Table 1 Summary of studies evaluating the role of radiomics in differentiating intraductal papillary mucinous neoplasms with advanced neoplasia
HGD: High-grade dysplasia; LGD: Low-grade dysplasia; CECT: Contrast-enhanced computed tomography; MRI: Magnetic resonance imaging; mi-RNA:micro-RNA; DWI: Diffusion weighted imaging; AUC: Area under curve; SN: Sensitivity; SP: Specificity; NA: Not application.
Thus, radiomics represents a promising non-invasive approach for the classification and risk stratification of PCLs and will favorably impact patient management.However, radiomics continues to be a novel concept and has been largely used to date in clinical trials at academic centers. While radiomics has demonstrated an immense potential for diagnosis, prognosis, and risk assessment in PCLs; there is a need for standardized protocols for image acquisition, segmentation, feature extraction, and analysis.
TRADITIONAL DIAGNOSTIC APPROACHES USING BIOMARKERS
Cyst fluid analysis
CEA and amylase: Traditionally pancreatic cyst fluid is aspirated using EUS-FNA for biomarker and cytologic analysis. In early studies, cyst fluid CEA levels above 192 ng/mL was shown to correlate with mucinous PCL with 79 % (88 /111 ) accuracy (P<0 .0001 )[25 ]. However more recent studies, have estimated CEA sensitivity and specificity at 63 % and 88 %, respectively in differentiating mucinous from nonmucinous cysts[26 ]. This level of accuracy would result in misdiagnosis of 35 %-39 % of mucinous cysts. Additionally, CEA levels across sites are difficult to compare and levels have not been shown to correlate with PCL malignant potential[25 ,27 -29 ].Regarding amylase levels, a low cyst fluid amylase level has very high specificity for excluding pseudocyst. However, high amylase levels have been shown to have no diagnostic utility[26 ,30 ]. As a result, measuring amylase has fallen out of favor for the diagnosis of PCLs.
Cytology: Cyst fluid analysis by cytology has been shown to lack sensitivity for the diagnosis of PCLs. A meta-analysis with 937 patients demonstrated cyst fluid cytology to have 63 % sensitivity and 88 % specificity for the diagnosis of PCL[31 ]. Another metaanalysis calculated cytology to have 51 % and 94 % sensitivity and specificity,respectively[32 ]. This lack of sensitivity results from cytology evaluations usually detecting only intact exfoliated cells that are typically few in number[25 ,33 ].Glucose:Intracystic glucose has good accuracy at differentiating mucinous and nonmucinous cysts but this economical diagnostic tool has not been used in routine clinical practice. However, recent prospective studies have provided improved and sustained evidence that cyst fluid glucose should be considered for standard of care evaluation of PCLs. Low intra-cystic glucose concentration is predictive of a mucinous cyst while high concentrations are consistent with non-mucinous cysts. In 2020 ,Ribaldoneet al[34 ] reported from 56 patients that intra-cystic glucose concentration <50 mg/dL had significantly better sensitivity than a CEA level > 192 ng/mL for diagnosing mucinous cysts (93 .6 % vs 54 .8 %; P = 0 .003 ). Both CEA and intra-cystic glucose had high specificity for diagnosing mucinous cysts (96 % vs 100 %; P = 1 ). They reported that intra-cystic glucose concentration of more than 50 mg/dL had higher sensitivity than CEA values of less than 5 ng/mL for diagnosing non-mucinous cysts(96 % vs 72 %, P = 0 .07 ).
A meta-analysis of 7 studies encompassing 566 patients reported that lower (cut-off< 50 mg/dL) intra-cystic glucose concentration had a pooled sensitivity of 90 .1 %(95 %CI: 87 .2 -92 .5 ) and pooled specificity of 85 .3 % (95 %CI: 76 .8 -91 .1 ) when differentiating mucinous from non-mucinous cysts[35 ]. In a subset analysis, point-of-care glucometer measurements for intra-cystic glucose (3 studies) also revealed comparable pooled sensitivity of 89 .5 % (95 %CI: 85 .5 -92 .5 ; I2 = 0 ) and pooled specificity of 83 .9 %(95 %CI: 68 .5 -92 .6 ; I2 = 43 ) for the differentiation of PCLs[35 ]. A more recent (2021 )meta-analysis that included 8 studies with 609 PCLs showed pooled sensitivities for glucosevsCEA of 91 % (95 %CI: 88 -94 ) vs 56 % (95 %CI 46 -66 ) (comparativePvalue <0 .001 ), pooled specificities were 86 % (95 %CI: 81 -90 ) vs 96 % (95 %CI: 90 -99 ), P > 0 .05 ,respectively[36 ].
Estimation of glucose levels is a low-cost diagnostic test that has repeatedly demonstrated better accuracy at differentiating mucinous and non-mucinous cyst.While not being definitive, cyst fluid glucose is a practical and economical diagnostic tool that can help in the differentiation of PCLs.
Molecular markers: With the introduction of next-generation sequencing (NGS),diagnosis of PCLs with either small gene panels and whole exome NGS have been employed. This method allows assessment of intact cell and cell-free nucleic acid that has been shed into the cyst fluid. DNA mutations that are commonly associated with pancreatic adenocarcinoma (KRAS, CDKN2A, SMAD4 , PTEN, PIK3 CA, and TP53 ) may also be present in precursor PCLs, with the latter five associated with advanced neoplasia.
Similar to radiomics, molecular analysis of cyst fluid can contribute to the classification of PCLs, and risk stratification of IPMNs. In a meta-analysis (6 studies, 785 PCLs), McCartyet al[37 ] reported that the dual presence ofKRASandGNASmutations detected mucinous PCLs with a sensitivity of 75 % (95 %CI: 58 -87 %), specificity of 99 %(95 %CI: 67 -100 %), and diagnostic accuracy of 97 % (95 %CI: 95 -98 %), respectively. For specifically diagnosing IPMNs, dualKRAS/GNASmutation had 94 % (95 %CI: 72 -99 %)sensitivity, 91 % (95 %CI: 72 -98 ; I2 = 89 .83 %) specificity and 97 % (95 %CI: 95 -98 %)accuracy, respectively. Recently, our group identified, for the first time, that uncommonBRAFmutations (and occasionalMAP2K1mutations) characterize a significant subset of IPMNs that lackKRASmutations, indicating that RAS-MAPK dysregulation is ubiquitous in these tumors[12 ]. In the same study, we showed 88 .5 %sensitivity, 100 % specificity, and 90 .3 % accuracy for NGS differentiation of PCLs[12 ].
For the risk stratification of IPMNs, Singhiet al[38 ] used next-generation sequencing to evaluate DNA mutations associated with advanced neoplasia. In a subgroup analysis of 102 patients with histopathologic diagnosis, they reported that the presence of TP53 , PIK3 CA and/or PTEN mutation had 88 % (95 %CI: 62 -98 %) sensitivity and 95 % (95 %CI: 88 -98 %) specificity, respectively for diagnosing IPMNs with advanced neoplasia.
Cyst fluid molecular analysis by next generation sequencing is superior to measuring cyst CEA levels with superior accuracy and the ability to provide risk stratification for IPMNs. However, it is selectively available and represents a logistical and financial barrier for universal adaptation.
ADVANCED INTERVENTIONAL DIAGNOSTIC APPROACHES
EUS-guided needle confocal laser endomicroscopy
EUS-guided needle confocal laser endomicroscopy (nCLE) permits real-time microscopic imaging of intra-cystic epithelium within a single plane. It allows forinvivopathological analysis of PCLs. Early studies have established the characteristic features for IPMNs. Investigations by Napoleonet al[40 ] in the CONTACT study established defining criteria for MCNs, SCAs, and cystic neuroendocrine tumors[39 ,40 ]. In 2020 , the INDEX study provided further support for nCLE as a viable diagnostic tool by demonstrating high performance in differentiating PCLs amongst the highest number (n= 65 ) of patients with surgical histopathology[41 ]. For the differentiation of PCLs into mucinous and non-mucinous lesions, a recent meta-analysis with 7 studies and 324 patients reported a pooled sensitivity, specificity and accuracy of 85 % (95 %CI: 71 -93 %), 99 % (95 %CI: 90 -100 %) and 99 % (95 %CI: 98 -100 %),respectively. The pooled risk of post-procedure acute pancreatitis was 1 % (95 %CI: 0 -3 %)[42 ]. Another recent meta-analysis (10 studies, 536 patients) reported a pooled sensitivity, specificity, and accuracy of 82 .4 % (95 %CI: 74 .7 -90 .1 %), 96 .6 % (95 %CI: 94 .3 -99 %), and 88 .6 % (95 %CI: 83 .7 -93 .4 %), respectively, for the differentiation of mucinous from non-mucinous PCLs[43 ].
In addition to the high accuracy of diagnosing IPMNs and other cysts, nCLE can potentially determine the risk for advanced neoplasia in PCLs. To detect advanced neoplasia in IPMNs, multiple nCLE imaging variables were identified in a post-hoc analysis of the INDEX study[44 ], Figure 2 . This study identified that the variables with the highest interobserver agreement were papillary epithelial thickness and darkness.Specifically, nCLE visualized papillary epithelial thickness (width ≥ 50 μm) had a sensitivity, specificity, and AUC of 87 .5 % (95 %CI: 62 %-99 %), 100 % (95 %CI: 69 %-100 %),and 0 .95 , respectively for the detection of advanced neoplasia. Also, estimation of the papillary epithelial darkness (cut-off ≤ 90 pixel intensity) revealed a sensitivity,specificity, and AUC of 87 .5 % (95 %CI: 62 %-99 %), 100 % (95 %CI: 69 %-100 %), and 0 .90 ,respectively[44 ]. Analogously for mucinous cysts, Feng et al[45 ] reported that nCLE pattern of “dark aggregates of neoplastic cells” correlated with the morphologic features of "irregular branching and budding" and was diagnostic of malignancy, with 75 % sensitivity, 100 % specificity and 94 % accuracy, respectively.
However, potential limitations of nCLE include differences in interobserver interpretation of images and the tedious nature of manually determining papillary epithelial thickness and darkness. Both of these issues were addressed with the development of a machine learning artificial intelligence model that identified advanced neoplasia in IPMNs with a sensitivity (83 %) and specificity (88 %) well above the Fukuoka or AGA guidelines[46 ].
Despite the growing evidence of nCLE as a viable diagnostic technique, its incorporation into standard clinical evaluation is lacking. The primary challenges include equipment costs, optimal training in image acquisition and interpretation, and prevention of adverse events higher than the standard EUS-FNA process.
EUS guided MFB or EUS-through-the-needle biopsy
This technique utilizes an EUS guided approach to pass a specialized device, the Moray micro forceps (Moray micro forceps, US Endoscopy, Mentor, Ohio, United States) through the 19 -gauge EUS needle to collect tissue sample from PCLs. Multiple recent studies have demonstrated an improved diagnostic yield and accuracy in the diagnosis of specific types of PCLs[47 ,48 ].
Multiple meta-analyses have been published and the most recent studies include the following. Tacelliet al[49 ] (2020 ) included 9 studies with 454 patients and pooled technical success, histological accuracy and diagnostic yield for specific types of PCLs were 98 .5 % (95 %CI: 97 .3 %-99 .6 %), 86 .7 % (95 %CI: 80 .1 -93 .4 ) and 69 .5 % (95 %CI: 59 .2 -79 .7 %), respectively. Additionally sensitivity and specificity for diagnosis of mucinous PCLs were 88 .6 % and 94 .7 %, respectively. However, the overall complication rate was 8 .6 % (95 %CI: 4 .0 -13 .1 %) with studies reporting rates ranging from 1 %-23 %. Of the reported complications, 57 .1 % had self-limiting bleedings (most commonly intra-cystic bleeding), 24 .5 % had mild pancreatitis, 6 .1 % had infections and 14 .3 % had abdominal pain. Westerveldet al[50 ] analyzed 8 studies with 426 patients reporting similar results. The MFB approach had significantly higher diagnostic yield for specific cyst type compared to cytology (72 .5 %, 95 %CI: 60 .6 -83 .0 % vs 38 .1 %, 95 %CI: 18 .0 -60 .5 %).Additionally, MFB had significantly higher diagnostic yield for mucinous cyst compared to cytology (OR: 3 .86 ; 95 %CI: 2 .0 -7 .44 , I2 = 72 %). Overall MFB procedures had a 7 % complication rate with 5 % incidence of intra-cystic hemorrhage and 2 .3 % risk of acute pancreatitis. More importantly, in a subgroup analysis of 92 patients who had surgical resection of their PCLs, MFB findings had concordance of 82 .3 % (95 %CI: 71 .9 -90 .7 %) for specific cyst diagnosis. MFB findings for mucinous cysts had a sensitivity of 90 .1 % (95 %CI: 78 .4 -97 .6 %) and specificity of 94 % (95 %CI: 81 .5 -99 .7 %). Additionally,the concordance rate for histological grade of dysplasia was 75 .6 % (95 %CI: 62 .3 -86 .8 ).
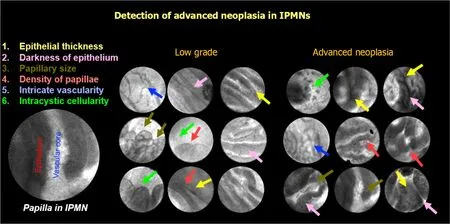
Figure 2 Features identified on endoscopic ultrasound guided needle confocal laser endomicroscopy. IPMN: Intraductal papillary mucinous neoplasms.
In another meta-analysis that included patients with surgical histopathology as reference diagnosis, the pooled sensitivity and specificity for diagnosing mucinous PCL was 86 % (95 %CI: 62 -96 %) and specificity 95 % (95 %CI: 79 -99 %) respectively[51 ].For diagnosis of specific cyst type, the pooled sensitivity and specificity were 69 %(95 %CI: 50 -83 %) and specificity 47 % (95 %CI: 28 -68 %), respectively. The authors also grouped IPMNs and MCNs with advanced neoplasia, SPNs, and cystic neuroendocrine tumors as high-risk cysts. MFB demonstrated a pooled sensitivity and specificity of 78 % (95 %CI: 61 -89 %) and 99 % (95 %CI: 90 -99 %) respectively for diagnosis of a high-risk cyst.
While MFB represents an excellent technique for acquisition of tissue and accurately diagnosing PCLs, the high rates of adverse events including acute pancreatitis and intra-cystic bleeding may deter clinicians from using this technique.
Contrast-enhanced EUS
EUS when combined with contrast enhancers allows detection of vascularity within PCLs. This allowed contrast-enhanced EUS (CE-EUS) to differentiate pseudocysts from true PCLs and identify mural nodules within PCLs. Despite early studies reporting no improvement over traditional EUS at differentiating PCLs[52 ], recent studies have reported higher diagnostic yield for PCLs using CE-EUS (96 % compared to 71 % for traditional EUS)[53 ]. CE-EUS detected small lesions initially missed on contrast-enhanced CT or EUS-FNA[54 ]. Recent literature on CE-EUS has reported higher accuracy at diagnosing PCLs compared to CT, MRI and traditional EUS[55 ].Despite these encouraging results, CE-EUS has not gained traction in clinical management of PCLs.
CONCLUSION
Future directions in the diagnosis of pancreatic cysts
Reliable and accurate diagnosis of PCLs is a bottleneck for appropriate management of these lesions. Although, novel diagnostics have improved the diagnostic accuracy,there is still a dearth of prospective multicenter studies and a need to understand the complementary role of these tests. Radiomics, as a non-invasive tool has the potential for preliminary risk stratification of PCLs into low-and-high risk lesions (Figure 3 ). The technique holds a potential to allow clinicians to skip expensive and invasive diagnostic techniques on certain low risk PCLs.
For low-risk PCLs, and when EUS-FNA is indicated, low-cost cyst fluid analysis with glucose, CEA, and cytology can guide management (Figure 3 ). If radiomics and EUS cyst morphology are indicative of a high-risk PCL, advanced diagnostics with cyst fluid molecular analysis, nCLE, or microforceps biopsy can be considered based on the center and endoscopists’ expertise. The rate of adverse events with microforceps biopsy needs to be considered when considering this test.

Figure 3 Future directions of detection and risk stratification of pancreatic cystic lesion to guide clinical management. PCL: Pancreatic cystic lesion, CEA: Carcinoembryonic antigen, IPMN: Intraductal papillary mucinous neoplasms.
Despite the availability of multiple diagnostic methods, the diagnosis and management of PCLs continues to be challenging. The more recent diagnostic modalities lack supportive larger multicenter data and there is need to demonstrate cost-effectiveness when compared to using suboptimal techniques and resultant unwarranted resection of otherwise benign or indolent PCLs. Apart from diagnosis,surveillance methods for low-risk lesions needs innovation as current tools are resource-consumptive.
 World Journal of Gastroenterology2022年6期
World Journal of Gastroenterology2022年6期
- World Journal of Gastroenterology的其它文章
- Comments on validation of conventional non-invasive fibrosis scoring systems in patients with metabolic associated fatty liver disease
- COVID-19 , liver dysfunction and pathophysiology: A conceptual discussion
- Gallbladder Burkitt’s lymphoma mimicking gallbladder cancer: A case report
- Validation of the PAGE-B score to predict hepatocellular carcinoma risk in caucasian chronic hepatitis B patients on treatment
- Atrophic gastritis and gastric cancer tissue miRNome analysis reveals hsa-miR-129 -1 and hsa-miR-196 a as potential early diagnostic biomarkers
- Effects of viremia and CD4 recovery on gut “microbiome-immunity” axis in treatment-naïve HIV-1 -infected patients undergoing antiretroviral therapy