
Crohn’s disease-related ‘gastrocnemius myalgia syndrome’ successfully treated with infliximab: A case report
2022-03-15 09:14:36JulienCatherineHazimKadhimFredericLambotClaireLiefferinckxVirginieMeurantLukasOteroSanchez
Julien Catherine, Hazim Kadhim, Frederic Lambot, Claire Liefferinckx, Virginie Meurant, Lukas Otero Sanchez
Abstract
Key Words: Crohn’s disease; Extra-intestinal manifestation; Gastrocnemius myalgia syndrome;Granulomatous myositis; Anti-tumour necrosis factor-α therapy; Case report
INTRODUCTION
The multi-system nature of inflammatory bowel diseases (IBD) is widely known. The extraintestinal manifestations (EIMs) of IBD are diverse and deferred from IBD diagnosis in a quarter of the cases. It has been estimated that 6 % to 47 % of patients with IBD experience at least one EIM[1 ]. The most frequently reported EIMs include peripheral and/or axial arthropathy, cutaneous lesions, ophthalmological immune-inflammatory manifestations and hepatobiliary affections[2 ]. However, EIMs can involve almost any organ or tissue, and some rare manifestations, such as specific muscular involvement can also occur and might even herald an hidden IBD[3 ].
We hereby report the first CD-associated GMS in a Belgian patient that turned out to be “granulomatous myositis”, an exceptionally rare subtype. In addition, we performed a literature review by searching EMBASE, MEDLINE, Scopus, and the Cochrane Library databases for studies published between January 1 , 1970 , and July 7 , 2021 , using the following keywords or MeSH terms: ‘Inflammatory Bowel Diseases’, ‘Crohn’s Disease’, ‘Ulcerative colitis’, ‘Myositis’, ‘Gastrocnemius myalgia syndrome’and ‘Granulomatous Myositis’. Finally, we discuss the role of anti-tumour necrosis factor (TNF)-α therapy in this specific context.
CASE PRESENTATION
Chief complaints
A 33 -year-old woman presented at the emergency department with a 5 -d history of isolated tenderness in both calves leading to walking difficulties.
History of present illness
She denied any traumatism but reported a colitis relapse 30 d before her admission which resolved with a short-course of modified-release beclomethasone therapy.
History of past illness
The patient had a history of allergic asthma,Heliobacter pylorigastritis and unclassified colitis. Previous investigations performed during colitis flares did not discriminate a specific IBD pattern concluding in an unclassified colitis. The patient was not taking any chronic medication. Her familial history was not contributive.
Physical examination
Clinical findings on admission included bilateral swelling of both calves which were warm and painful to palpation. Motricity and sensitive perception were preserved. Examination of other muscles, joints and the spine was unremarkable and her abdomen was soft and non-tender.
Laboratory examinations
Initial laboratory investigations showed a C-reactive protein level at 106 .6 mg/L (normal range, 0 .4 -12 mg/L) with mild neutrophilic leukocytosis (8770 /mm3 , normal range 1900 -8000 /mm3 ). Creatinine kinase (CK), aspartate aminotransferase, lactate dehydrogenase and D-dimer serum levels were within reference values. Hemocultures were negative as well as antinuclear, antineutrophil cytoplasmic and anti-saccharomyces cerevisiaeantibodies.
2.4 miR-145过表达抑制SiHa细胞的迁移和侵袭能力 与NC组比较,miR-145过表达组SiHa细胞迁移、侵袭能力均显著下降,差异有统计学意义(P<0.05),见图4(封二)。
Imaging examinations
Ultrasonography of lower limbs revealed a bilateral 5 -millimeter-thick edema surrounding gastrocnemius muscles in the absence of vascular abnormality while a magnetic resonance imaging showed marked inflammation of muscles and their fascia in both legs, suggested by a high signal on T2 -weighted images and a strong gadolinium enhancement on fat-suppressed T1 -weighted images(Figure 1 ).
Muscular biopsy
A muscular biopsy of the right gastrocnemius revealed a remarkable inflammatory reaction that particularly involved the perimysial compartment. The infiltrate mainly comprised dense lymphoplasmocytic cells with the formation of several granulomatous structures wherein several histiocytes,sometimes multinucleated, were observed (Figure 2 A, C and D). Endomysial inflammatory infiltrate was however less remarkable and rather discrete and focal. There was besides a very mild and discrete perivascular affinity for the inflammatory infiltrate but there was no frank/convincing vasculitis in the examined sections (Figure 2 B). A few muscle fibers showed suspected myofibrillary disintegration.Immunohistochemical analyses showed an outstanding cohort of CD3 positive cells (with a slight predominance of CD8 + over CD4 + cells) (Figure 2 C and D). Electron microscopy was generally unremarkable and showed rare lipofuscin deposits. Moreover, rare mastocytes were observed.
FINAL DIAGNOSIS
This histomyopathological affection in this clinical context was concordant with the GMS, a rare disorder classically associated with CD[6 ]. Moreover, a new ileocolonoscopy was performed during the hospital stay and revealed endoscopic pattern in favor of CD diagnosis, despite the absence of intestinal granuloma on histopathologic examination.
TREATMENT
Considering these results, the patient was started on a prednisone equivalent dose of 1 mg/kg, resulting in a rapid clinical and biochemical remission.
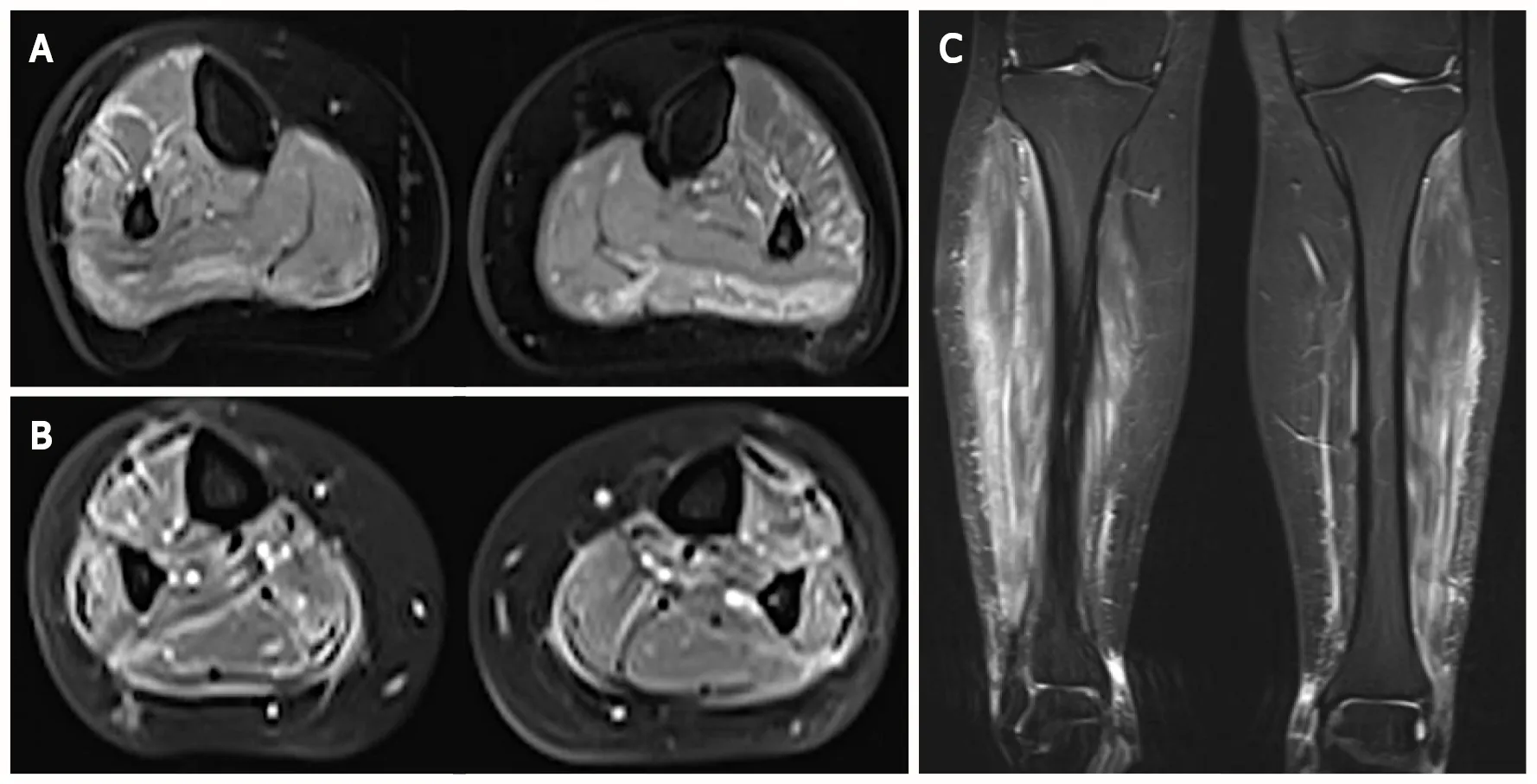
Figure 1 Magnetic resonance imaging of the calves in axial and frontal views. A and C: Demonstration of high signal on T2 -weighted images in muscles from posterior and lateral compartments of the legs as well as in their surrounding fascia; B: This finding was accentuated on gadolinium-enhanced fatsuppressed T1 -weighted images, suggestive of myositis and fasciitis.
OUTCOME AND FOLLOW-UP
Two months later, the patient experienced intestinal symptoms associated with a recurrence of pain in both legs during corticosteroids (CS) tapering. The ileocolonoscopy performed at that time showed a very severe ileocolitis [CD Endoscopic Index of Severity (CDEIS) scored at 31 ] with no histopathologic evidence of granuloma for which intravenous methylprednisolone (1 mg/kg for 5 d) and infliximab (5 mg/kg at week 0 , 1 and 4 ) therapies were started to target both muscular and intestinal disease leading to clinical remission of both ileocolitis- and myositis-related symptoms. Oral corticotherapy was then prescribed and slowly tapered while infliximab was continued (5 mg/kg, every 8 wk). Twenty months later, both ileocolitis and myositis were quiescent.
DISCUSSION
Inflammatory myopathies (IM) occurring in the setting of IBD are considered as rare EIMs and have been roughly described in the literature to date[6 ]. We report the first CD-associated GMS in a Belgian patient that besides turned out to be “granulomatous”. This represents a very exceptional subtype as there has been only two such reported cases. To the best of our knowledge, only 15 cases of GMS are described in the international literature and always occurred in patients with CD (Table 1 ). Apart from GMS, orbital myositis, which is currently considered as a subtype of idiopathic orbital inflammation,has also been reported in patients with IBD, mainly CD[5 ]. Few cases of dermatomyositis (DM) and polymyositis have also been described during the course of IBDs and a recent study showed that DM was more frequent in ulcerative colitis patients than CD patients and control subjects[7 ]. Nevertheless,the true incidence of IM occurring in this context is probably underestimated as myalgia can be confused with joint manifestations or with non-inflammatory muscle disorders (e.g., secondary to hypokalemia or medications) and by the fact that clinicians may rule out myositis’ diagnosis in the absence of CK elevation in serum.
The first case of myositis affecting gastrocnemius muscles in CD was reported in 1979 by Ménardet al[8 ] who described a 44 -year-old man with granulomatous myositis localized to the calf occurring two months before CD diagnosis[8 ]. Since then, several cases have been reported, sharing the classically following features: (1 ) Calf-limited myalgia revealing localized myositis; (2 ) Normal serum CK levels;and (3 ) A high early-response rate to CS therapy[9 ]. In 2003 , this entity was denominated as “GMS” by Christopouloset al[3 ], a term adopted in the literature ever since[10 ]. Most patients developed GMS months or years after the onset of CD but myositis could precede gastrointestinal manifestations by up to 10 years[11 ]. When CD had been diagnosed before GMS, the intestinal disease was active in most cases at myositis’ diagnosis (Table 1 ). Other EIMs were associated with GMS in 50 % of patients which is in accordance with previous observations that patients who presented an EIM are at higher risk to develop another one[1 ].

Table 1 Case descriptions of gastrocnemius myalgia syndrome reported in Crohn’s disease
While clinical and biological features in patients with GMS are generally characteristics, histomyopathological findings are rather heterogeneous. In fact, our case is only the third in which granulomatous lesions were observed while all remaining reported cases were characterized by non-granulomatous inflammation (4 cases) or localized vasculitis (5 cases) (Table 1 ). However, whatever the histopathologic image observed, the inflammatory infiltrate was more often localized in the perimysium and more discrete in the endomysium, probably explaining why most patients with GMS have normal CK values. GMS could therefore represent a form of localized “perimyositis” with no or limited myofiber injury. This observation also suggests that the immune response is directed against connective tissue components or vessels rather than against the myofibers themselves.
Finally, while GMS was initially controlled in this case by oral CS therapy, it ultimately relapsed during tapering. In this context, the presence of a concomitant severe active ileocolitis prompted us to start an anti-TNF-α agent. While CS were the first-line treatment prescribed in almost all cases of GMS,their efficacy, however, was not enduring as 6 /16 patients (including ours) relapsed during dose deescalation (Table 1 ). Moreover, two other patients were initially refractory to CS[12 ,13 ]. Various drugs were used in these corticosteroid-dependent or refractory cases. Anti-TNF-α agents were constantly associated with GMS remission in the six cases where they were introduced, suggesting that the muscular and intestinal affections in this context could share a common pathophysiological mechanism.Importantly, our case represents the first GMS with granulomatous inflammation treated with an anti-TNF-α agent. Further case descriptions and/or case series will be required to ascertain the role of such therapy in this specific context.
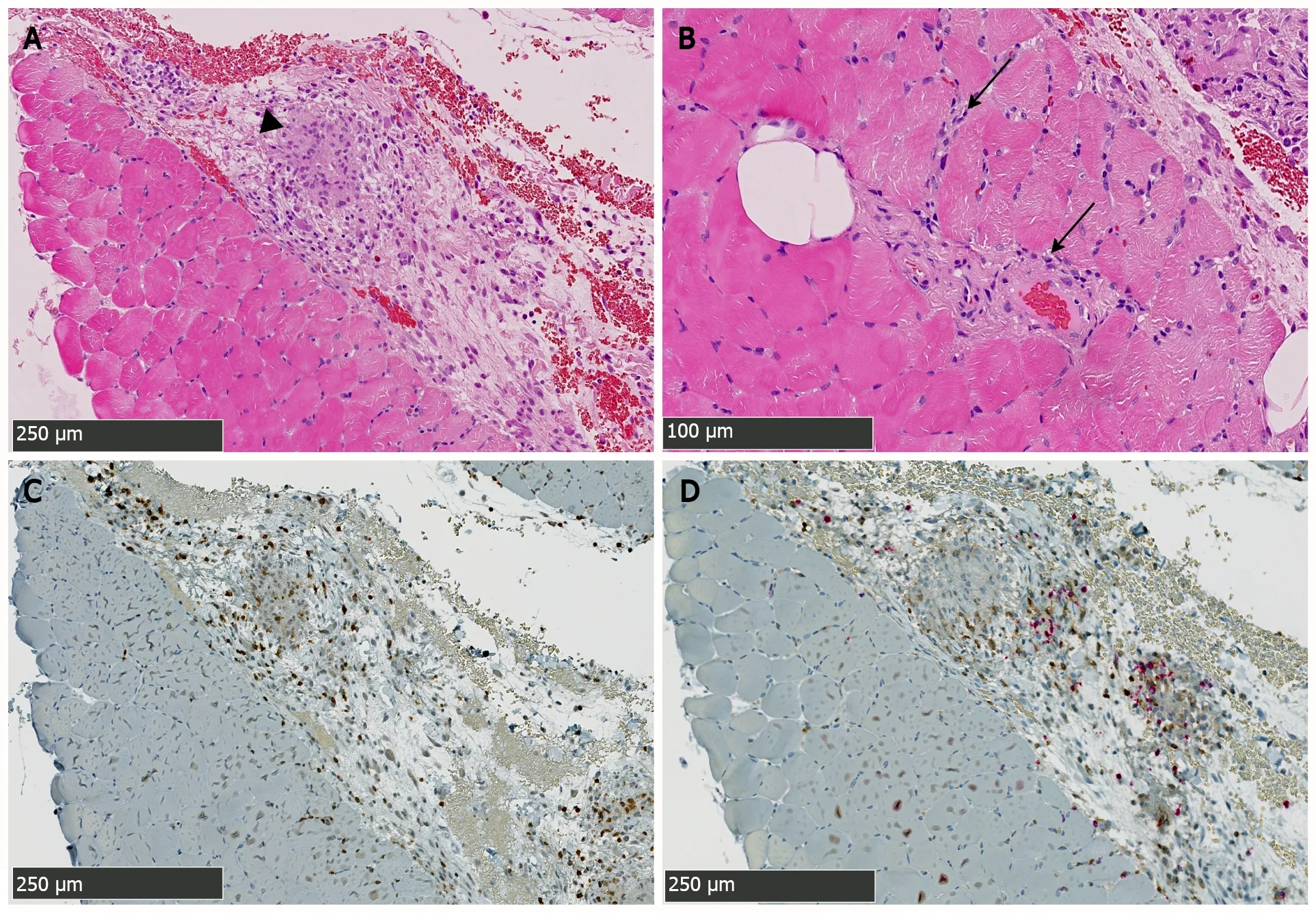
Figure 2 Biopsy specimen from the right gastrocnemius muscle showing the intense immune-inflammatory reaction. A: This hematoxylin and eosin-stained section shows the granulomatous nature (arrowhead) of this Crohn’s disease-associated skeletal myositis, predominating in the perimysial compartment; B: Discrete and focal immune infiltrates are found in the endomysium and around vascular structures (arrows); C and D: Immunohistochemical staining characterize immune cell-types involved therein: Co-staining for CD3 (brown staining) and CD20 lymphocytes (red staining) shown in C reveals predominance of CD3 + lymphocytes over CD20 + cells. CD4 and CD8 T cells subtyping shown in D (brown and red staining respectively) further reveals a slight predominance of CD8 +over CD4 + cells.
CONCLUSION
In conclusion, we report a rare extra-intestinal manifestation of CD, namely a GMS, characterized by a very rarely reported granulomatous perimyositis. The rapid relapse of GMS during CS tapering and the emergence of a severe active ileocolitis prompted the introduction of an anti-TNF-α agent that resulted in persistent clinical remission of both disorders. This might further suggest the effectiveness of such agents in CS-dependent or refractory cases. Finally, physicians should remain aware of the eventual emergence of a such complicating myositis when musculo-skeletal symptoms arise in IBD patients even in the absence of CK elevation.
ACKNOWLEDGEMENTS
We thank Anaïs Boisson (Laboratory of Molecular Immunology, Jules Bordet Institute, Brussels, 1000 ,Belgium) who performed immunohistochemistry stainings.
FOOTNOTES
Author contributions:Lambot F, Catherine J and Otero Sanchez L managed the patient; Kadhim H did myopathology diagnosis and analyses; Catherine J, Otero Sanchez L and Meurant V designed the study and collected data;Catherine J and Otero Sanchez L drafted and wrote the manuscript; Liefferinckx C, Lambot F and Kadhim H provided their expertise throughout the course of the work by revising and editing the manuscript; all authors approved the final version of the manuscript to be published.
Supported byNational Fund for Scientific Research (F.R.S-FNRS) as research fellows to Catherine J and Otero Sanchez L; Fonds Erasme to Otero Sanchez L; and F.R.S-FNRS as postdoctoral fellow to Liefferinckx C.
Informed consent statement:The study was performed in accordance with the ethical standards of the Helsinki Declaration and was approved by the institutional review board of CHU Tivoli (approval number #1396 ). Patient’s informed consent was obtained by Meurant V.
Conflict-of-interest statement:Liefferinckx C received consultancy fees from Takeda and Galapagos; speaker fees from Sandoz, Janssen and AbbVie.
CARE Checklist (2016 ) statement: The authors have read the CARE Checklist (2016 ), and the manuscript was prepared and revised according to the CARE Checklist (2016 ).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4 .0 ) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4 .0 /
Country/Territory of origin:Belgium
ORCID number:Julien Catherine 0000 -0001 -8825 -8126 ; Hazim Kadhim 0000 -0003 -4943 -9172 ; Frédéric Lambot 0000 -0003 -3585 -3444 ; Claire Liefferinckx 0000 -0002 -2046 -4051 ; Virginie Meurant 0000 -0002 -7626 -8543 ; Lukas Otero Sanchez 0000 -0002 -8013 -1371 .
S-Editor:Fan JR
L-Editor:A
P-Editor:Fan JR
猜你喜欢
作品(2022年10期)2022-10-18 10:24:18
新少年(2022年9期)2022-09-17 07:10:54
作品(2022年6期)2022-06-30 09:45:38
音乐探索(2022年2期)2022-05-30 21:01:37
孙子研究(2021年1期)2021-05-12 01:01:36
小天使·一年级语数英综合(2020年6期)2020-12-16 02:56:41
小天使·一年级语数英综合(2019年8期)2019-08-27 02:23:00
小学科学(学生版)(2018年7期)2018-08-13 09:33:04
北极光(2014年8期)2015-03-30 02:50:51
郑州大学学报(医学版)(2015年2期)2015-02-27 14:50:46
 World Journal of Gastroenterology2022年7期
World Journal of Gastroenterology2022年7期
- World Journal of Gastroenterology的其它文章
- Gallbladder biliary lithotripsy: A new rationale applied to old treatment
- Stereotactic radiotherapy and the potential role of magnetic resonance-guided adaptive techniques for pancreatic cancer
- Will the collaboration of surgery and external radiotherapy open new avenues for hepatocellular carcinoma with portal vein thrombosis?
- Early gastric cancer: A challenge in Western countries
- Effect of Bifidobacterium longum 35624 on disease severity and quality of life in patients with irritable bowel syndrome
- Clinical online nomogram for predicting prognosis in recurrent hepatolithiasis after biliary surgery: A multicenter, retrospective study