
Atrial fibrillation burden and the risk of stroke: A systematic review and dose-response meta-analysis
2022-03-07 13:06YangSYHuangWangALGeMaZhiWangLN
World Journal of Clinical Cases 2022年3期
INTRODUCTION
This meta-analysis demonstrated that AF burden is a significant risk factor for clinical AF and stroke. There is a linear dose-response between AF burden and risk of stroke.Further studies are needed to validate this effect and evaluate the cut-off value for AF burden among patients requiring anticoagulation treatment.
Some studies demonstrated an association between AF burden and stroke risk, but few mentioned the existence of a dose-response effect. The Italian AT 500 registry study showed that patients with device-detected AF episodes of > 24 h had a 3.1-fold increased risk of stroke. In contrast, patients with AF episodes of > 5 min and < 24 h experience no significant increase in stroke risk[7]. Moreover, the ASSERT Clinical Trial reported episodes lasting > 6 min were associated with an increased risk of ischemic stroke or systemic embolism[8]. A recent systematic review demonstrated the AF burden exceeding different thresholds was associated with an increased risk of stroke; however, they did not provide a definite threshold for AF burden at stroke risk[9]. It is a matter of controversy whether an AF burden of > 5 min can increase the risk of stroke, and no studies have reported the potential dose-response effect on stroke.Accordingly, we performed a systematic review and meta-analysis to determine the association between AF burden > 5 min and the increased risk of stroke and explored the dose-response effect between these two factors.
MATERIALS AND METHODS
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines[10].
Search strategy
The literature search was performed by two researchers (YSY and HM) with the help of an experienced medical reference librarian. Studies were retrieved by searching electronic databases (PubMed, EMBASE, Medline, Cochrane, Web of Science) from inception until February 28, 2020. The following search terms were used: AF,physiological monitoring, implantable cardiac monitor, artificial pacemaker, electrocardiograph, burden, stroke, cerebrovascular disorders, brain infarction and thromboembolic event. The language of publication was restricted to English. We also retrieved the reference lists of included articles and previous reviews to identify potential studies as comprehensively as possible. All retrieved references were exported to EndNote X9, and duplicate citations were removed.
理想人格的典范和目标深刻地影响着当代中国人的人格建构[6]。十八大报告提出的社会主义核心价值观中,也十分深刻地体现出在继承和发扬优秀传统文化的基础上,对当代大学生人格发展的要求。基于上述传统文化中理想人格的特征,大学生人格培育需要在吸取中国传统文化的精华中彰显时代发展的特质,符合相应的人格修养标准。
Inclusion criteria and exclusion criteria
Two investigators (YSY, HM) independently assessed the eligibility of the studies identified. The inclusion criteria included: (1) Studies that described AF burden within 1 d or more; (2) Studies that described the method used to quantify AF burden such as a pacemaker, implantable cardioverter-defibrillator and cardiac-resynchronization device; and (3) Studies where clinical outcomes included stroke, ischemic stroke,systematic embolism, transient ischemic attack or other thromboembolic events. The combined endpoint of these outcomes was also included: (1) Studies that directly and/or indirectly provided the relative risk of the outcome, including hazard ratio(HR), risk ratio (RR) and odds ratio (OR) values; (2) Observational studies or randomized controlled trials (RCTs); and (3) Studies where the study design and methods were described in detail.
However, reviews, conference abstracts, editorials, case reports, duplicate publications and cross-sectional studies were excluded.
Data extraction
Two researchers (YSY and HM) independently extracted the following information from the included studies: Study type, significant AF burden definition, adverse outcomes, sample size, follow-up period, the method for AF monitoring and others.The number of cases and HR, RR, OR for the risk of the adverse outcomes for different AF burdens were also recorded. HRs provided by original studies were considered as adjusted RRs. We also contacted the authors for additional data or any clarification if necessary. Disagreements were resolved by a consensus-based discussion.
Quality assessment and the level of evidence
The quantitative assessment tool ‘QualSyst’[11] and the Oxford Centre for Evidence-Based Medicine 2009 Level of Evidence Tool[12] were used to assess the methodological quality and the evidence levels of the included studies by two researchers (YSY and HMJ). The ‘QualSyst’ scoring system included 14 criteria with three possible answers: Yes, No, and Partial. “Yes” = 2 points, “No” = 0 points and “Partial” = 1 points. Items not applicable to a particular study design were marked ‘NA’ and were excluded from calculating the summary score. A summary score was calculated for each article based on the evaluation criteria. A score greater than 75% of the summary score indicated strong quality, a score ranging from 55% to 75% indicated moderate quality, and a score lower than 55% indicated poor quality. The level of evidence was assessed according to the type of study, and each subgroup level included five levels.
Data synthesis and statistical analysis
Grade A (Excellent): 0
AF burden > 5 min was associated with an increased risk of clinical AF [adjusted risk ratio (RR) = 4.18, 95% confidence interval (CI): 2.26-7.74]. However, no association was found with an increased risk of all-cause mortality (adjusted RR =1.55, 95%CI: 0.87-2.75). Patients with AF burden > 5 min had an increased risk of stroke (adjusted RR = 2.49, 95%CI: 1.79-3.47). Moreover, a dose-response analysis showed that the increased stroke risk was paralleled by an increase in AF burden at a rate of 2.0%hour (= 0.656, RR = 1.02, 95%CI: 1.01-1.03). Trial sequential analysis provided robust evidence of the association between AF burden > 5 min and an increased risk of stroke.
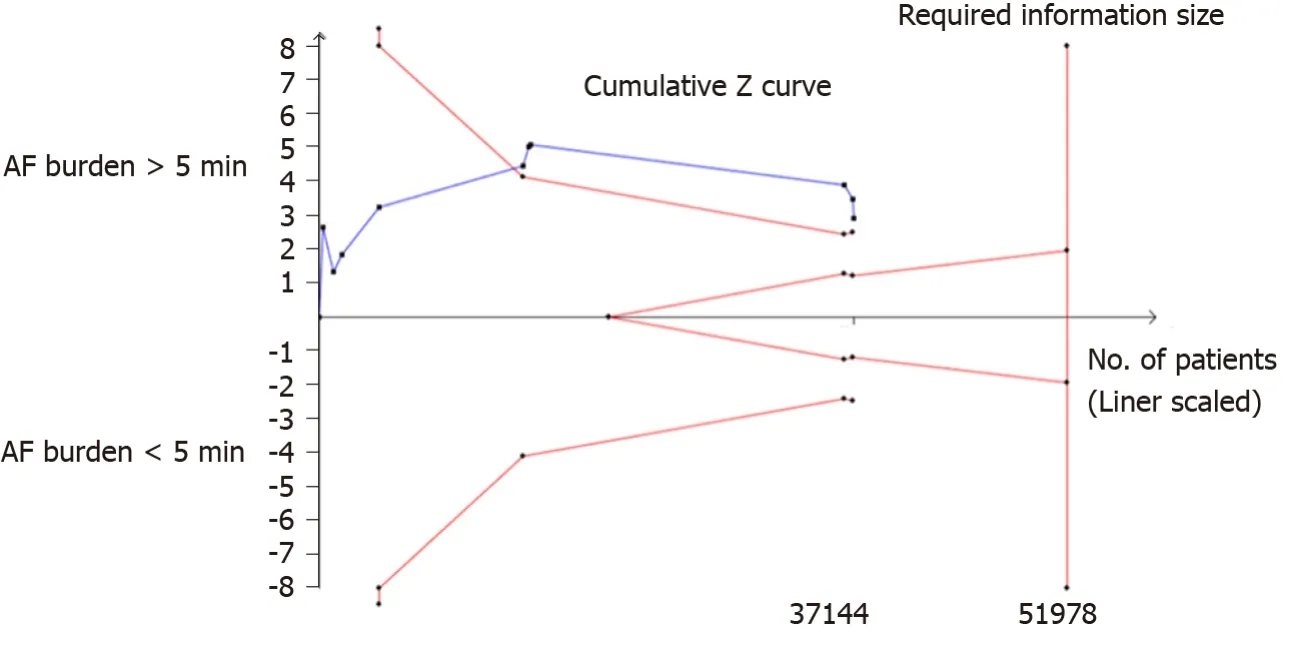
Moreover, when the AF burden was not a definite value, the midpoint between the upper and lower boundaries was considered as the average AF burden; when the lowest level was an open interval, the lowest dose was assumed to be 0; when the highest category was open-ended, a value with 1.5 times of the boundary of the highest dose was considered the dose[16]. Trial sequential analysis (TSA) was used to evaluate the statistical power of the current sample size and provide robust evidence of the effect of AF burden on the stroke risk[17]. Heterogeneity-adjusted required information size was calculated with α = 0.05, β = 0.2 and a relative risk reduction of 30%.
The meta-analysis was conducted using Review Manager (v5.3). The potential doseresponse association was conducted by STATA software (v15.0, College Station, TX,United States). TSA was conducted with TSA 0.9.5.10 Beta software (http://www.ctu.dk.tsa)[18].
RESULTS
Identification of studies
The search strategy yielded a total of 10479 abstracts from five English databases,while a manual search of the references cited in other available included articles and previous reviews yielded an additional 372 abstracts. After removing duplicates, 7827 studies remained. After abstract screening, 7004 studies were excluded. The remaining 823 full-texts were assessed for eligibility based on the inclusion and exclusion criteria,and 807 studies were excluded for the following reasons: 412 were not original articles,218 lacked detailed data on AF burden and 126 did not provide information on the clinical outcomes, 44 had a history of AF or stroke, and seven were cross-sectional studies. Finally, 16 studies were included in the quantitative synthesis (Figure 1).
Characteristics of the involved studies
Table 1 shows the characteristics of the included 16 studies, all except one were RCT studies[7,8,19-32]. The detected devices for AF burden included one or more of the three following devices: Pacemaker, implantable cardioverter-defibrillator and cardiac-resynchronization device. The 16 studies included 53141 subjects with mean or median ages > 65 years. Except for case-crossover study, subjects in all studies were followed up for at least 1 year to ascertain the clinical outcomes[25]. Four studies were multinational consortium studies; six were conducted in European countries, four in North American countries and two in Asian countries.
仅就融资功能而言,中国金融业一方面尚未建立覆盖一、二、三产业及不同所有制企业的服务体系。此外,因资本市场的长期萎靡不振而使中国的融资体系一直表现得过度偏狭,同时对技术研发创新的融资现尚处摸索阶段;人们在不同地域多元配置资产的愿望也未能得到满足,金融机构自身也主要依靠传统方式去消化自身的经营风险。这就是金融业跟不上社会经济发展的问题。
Table 2 shows the quality evaluation and the evidence level for each study. Twelve studies were associated with scores higher than 21. The levels of evidence ranged from 1b to 3a, and most were considered level 2b evidence.
为进行军民融合,双方作出妥协和改动是不可避免的,而融合标准制定的一个重要原则就是在标准层面上就应考虑融合会带来的影响,并在标准融合时将这种影响降到最低。
The incidence of AF burden > 5 min and stroke
Eleven studies provided data on the incidence of AF burden > 5 min. The detectable rate of AF burden > 5 min ranged from 10.12% to 70.77% among CIED patients, and AF burden > 24 h ranged from 6.70% to 39.26%. Overall, AF burdens > 5 min and > 24 h were detected in 26% (95%CI: 1%-52%) and 15% (95%CI: 6%-35%) of patients within the follow-up period, respectively, and the pooled incidence of stroke was 2.80%(95%CI: 1.56%-4.03%).
Association between AF burden > 5 min and future stroke risks
Sufficient data were obtained to calculate the crude RR for stroke associated with AF burden > 5 min in each study. The average follow-up for the 11 studies ranged from 12 to 67 mo (mean = 36.18 mo). The random-effects pooled analysis revealed that patients with AF burden > 5 min had a 67% increased risk of stroke (RR = 1.67, 95%CI: 1.25-2.25) compared with patients with AF burden < 5min (Figure 2A). Significant heterogeneity was found within the included studies (= 52%,= 0.020). The funnel plot was symmetrical, and Egger’s test showed no significant publication bias (= 1.56,=0.150).


TSA of ten studies showed that 71.5% (37144 out of 51978 patients) of the heterogeneity-adjusted information size required was accrued. We also found that the 1.08,= 0.340) among these studies.cumulative Z curve crossed the trial sequential monitoring boundary, providing robust evidence of the association between the AF burden > 5 min and increased risk of stroke based on the sample size (Figure 3).
Subgroup analyses of association between AF burden > 5 min and the future stroke risk
The fixed-effect pooled analysis performed with adjusted RRs revealed that patients with AF burden > 5 min had a 1.23-fold increase in risk of stroke (RR = 2.23, 95%CI:1.48-3.35), compared to AF burden < 5 min among patients with no history of AF.Moreover, patients with AF burden > 5 min had a 2.14-fold increase in the risk of stroke (adjusted RR = 2.14, 95%CI: 1.23-3.72) compared to AF burden < 5 min among patients not on anticoagulation therapy. The detailed results of subgroup analyseswith different populations are shown in Supplementary Table 1.


Does-response relationship between AF burden and the future stroke risk
Seven studies were included in the dose-response meta-analysis on the association between AF burden and stroke. The potential linear or nonlinear dose-response association was evaluated using a restricted cubic splines regression model. A linear dose-response relationship(= 0.656) was found (Figure 4),and AF burden was associated with 2.0% and3.0% increased risksofstroke for every 1h (RR =1.02,95%CI: 1.01-1.03) and 2 h (RR = 1.03, 95%CI: 1.02-1.05), respectively.
AF burden and risk of clinical AF
Three of the included studies, including 3286 patients, provided adjusted RRs values of the AF burden > 5 min on the risk of clinical AF. The random-effect pooled analysis reveal that patients with AF burden > 5 min had a 3.18 fold increased risk of clinical AF (adjusted RR = 4.18, 95%CI: 2.26-7.74) compared with the patient suffering AF burden < 5 min (Figure 5). The heterogeneity was significant among the different study designs (= 77%,= 0.010), RCT[19] and two retrospective observational studies[8,26]. The funnel plot was symmetrical and no significant publication bias was found in the Egger’s test (= 0.80,= 0.570).
AF burden and the risk of all-cause mortality
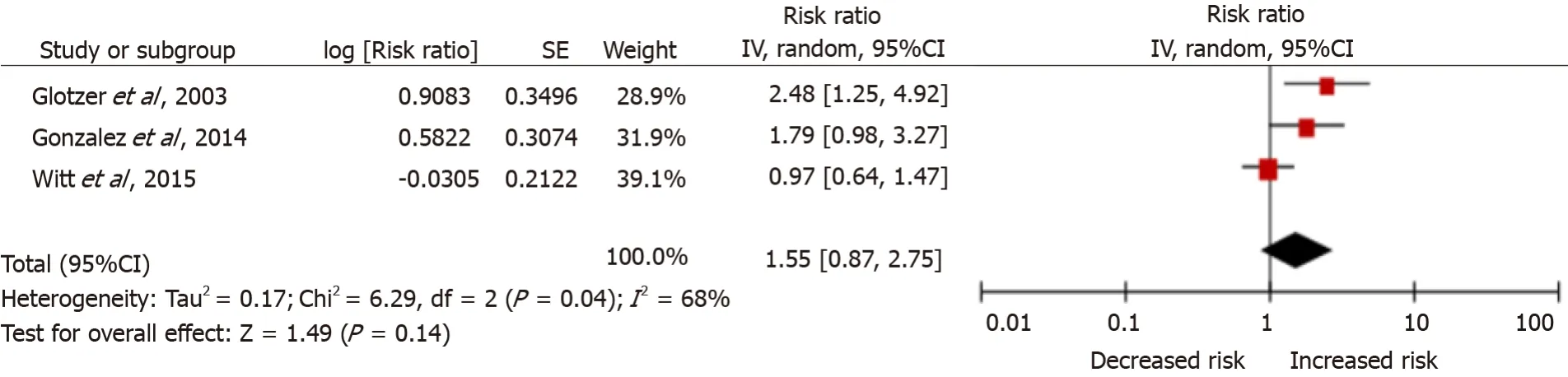
The reported adjusted RRs for the strength of association between AF burden > 5 min and risk of all-cause mortality in three studies differed. An ancillary study of the Mode Selection Trial trial[19] included patients with sinus node disease who were in sinus rhythm at the time of pacemaker implantation and aged > 21 years. Two studies[23,26]included patients with no history of AF. The random-effects pooled analysis found that patients with AF burden > 5 min had a 55% increased risk of all-cause mortality(adjusted RR = 1.55, 95%CI: 0.87-2.75) (Figure 6); however, significant heterogeneity (= 68%,= 0.040) and publication bias (= -21.13,= 0.030) were present in this analysis.
供给情况:国产钾方面,盐湖装置正常运作,日产1.4万吨,日发运200-300车,青海小厂开工率维持低位;青海盐湖库存略降,基准产品60%晶粉到站价维持2350元/吨,各地经销商到站参考报价维持2200元/吨。进口钾方面,到船量仍较少,港口钾库存180万吨,市场可售现货紧俏;贸易商看涨预期仍强,62%俄白钾主流报价维持2350元/吨。边贸钾方面,到货量较少,库存偏低,货源供应持续偏紧,62%俄白钾报价涨至2150元/吨。

DISCUSSION
In this systematic review and dose-response meta-analysis on the association between AF burden and the risk of stroke, 16 original studies were included, including 53141 CIED patients. First of all, we found that patients with an AF burden > 5 min had an increased risk of stroke. Moreover, a linear dose-response relationship was found; the risk of stroke was increased by 2.0%hour among subjects with AF burden > 5 min.Last but not least, we found AF burden > 5 min was associated with a significantly increased risk of clinical AF but not associated with an increase in all-cause mortality.
AF burden: A significant risk factor for stroke
Data from each study were extracted to calculate the crude RRs without considering the time-to-event endpoints. The pooled results indicated that patients with AF burden> 5 min had a higher stroke risk. That significant heterogeneity was detected for the pooled analysis of the relationship between AF burden and stroke risk (= 52%,=0.02). The heterogeneity might be associated with the variations in patient populations,hypertension, prior AF and antithrombotic therapy,.[33]. The population included in our study had different comorbidities, including patients with symptomatic atrial tachyarrhythmias[7,20], sinus node disease[19] and heart failure[22]. Moreover, some studies provided no information on patient history of AF[8,23,26-28]. Besides, in the study by Chu[29], patients with oral anticoagulants for any reason were excluded.However, even though anticoagulants were used in different proportions of patients at baseline, we found that the heterogeneity was not significant. With the pooled data of HRs adjusted for one or more known embolism predictors [including age, sex, heart failure, prior stroke diabetes, congestive heart failure, hypertension, age 75 years,diabetes mellitus, stroke or transient ischemic attack, vascular disease, age 65 to 74 years, sex category (CHA2DS2-VASc) score], we found that an AF burden > 5 min was associated with an increased risk of stroke (= 0,= 0.62).
We found that subjects with AF burden of > 5 min had a 67% increased risk of stroke. Recently, a meta-analysis also found that subclinical AF (pooled with highest AF duration cut-off values from the original studies) was associated with a 2.4-fold increased risk of stroke[9]. These results indicated that the risk of stroke was higher among the subjects with the serious AF burden. This finding provides novel insights that can be used to develop stroke prophylaxis approaches for AF patients.

Consistently, Shanmugam[22] found that a higher AF burden (AF burden > 3.8 h) was associated with a 9.4-fold risk of stroke among CIED patients. Two studies[28,30] also reported that patients with AF burden > 24 h had an increased risk of stroke.However, these results were inconsistent with a study by Healey[8], which could be accounted for by the fact that patients who experienced long periods of sinus rhythm and the better treatment of stroke had no history of AF[8].


The European and American[34] guidelines recommend estimating stroke risk in AF patients based on the CHA2DS2-VASc score. Moreover, an oral anticoagulant is recommended to reduce thromboembolic stroke risk in patients with AF, especially male patients with a CHA2DS2-VASc score of 1 and female patients with a CHA2DS2-VASc score of 2. Interestingly, some studies explored the association between AF burden and CHA2DS2-VASc scores. Botto[20] indicated that patients with a CHADS2 score of 1 or 2 had either a high or low stroke risk consistent with a high or low detected AF duration, respectively. Kaplan[30] also found an interaction between AF duration and CHA2DS2-VASc score. The risk of systemic embolism in patients with intermediate CHA2DS2-VASc scores was variable and correlated with the maximum AF burden. Accordingly, the stroke risk among AF patients should be evaluated based on the CHA2DS2-VASc score and AF burden to provide better personalized anticoagulation decisions.
Association between AF burden and risk of clinical AF or all-cause mortality
Clinical AF is a chaotic heart rhythm characterized by an irregular and often rapid heart rate documented with a 12-lead electrocardiogram. Electrocardiogramdocumented AF was confirmed in 38.9% of patients with AF burden and 2.1% without AF burden[19]. Our study found that AF burden > 5 min was associated with an increased risk of clinical AF. Furthermore, progression from paroxysmal to persistent or permanent AF might be faster in patients with subclinical AF who did not receive treatment. Consequently, more emphasis should be placed on screening patients with AF burden > 5 min and providing timely therapy.
Our study demonstrated that AF burden was not associated with all-cause mortality. However, there was significant heterogeneity in this meta-analysis. Indeed,further research is required to explore the role of AF burden on all-cause mortality.
Limitations
Even though this meta-analysis was performed utilizing crude RRs and adjusted RRs,there are still some limitations. Owing to the lack of adjusted RRs corresponding to three or more groups of AF burden, this meta-analysis was conducted without considering the time-to-event points and adjusting for confounding factors.Furthermore, patients with CIEDs might have diabetes, hypertension and other stroke risk factors, which might lead to an overestimation of the effect of AF on stroke.Underreporting of stroke and prescribing an oral anticoagulant to patients with higher AF burden might also lead to underestimating the impact of AF burden on the stroke risk. However, anticoagulation was used in the different subgroups of patients who had comorbidities at the baseline. Finally, publication bias was present in this study.Our results might have been influenced by non-published studies or language bias as we only included studies published in English.
黄国滋等[22]对普洱茶晒青毛茶和陈香茶中可溶性糖在储存过程中的变化进行研究,在3种不同的储存环境下储存540 d,2类茶可溶性糖的保留量与储存时间成反比,即随着储存时间的延长,其可溶性糖的保留量逐渐减少。
CONCLUSION
Atrial fibrillation (AF) is one of the most frequent cardiac arrhythmias. Reports suggest that an estimated 12.1 million people will suffer from this condition in the United States by 2030 and 17.9 million people in Europe by 2060[1,2]. It has been established that patients with AF have a 3 to 5-fold increased risk of stroke, and subjects with AF-related embolic stroke have a worse progression than those who experience stroke not related to AF[3-5]. With the widespread use of cardiac implantable electronic devices (CIEDs) and wearable devices, it is now possible to monitor the time and frequency of AF episodes. The American Heart Association recommends that the AF burden should be defined as the duration of the longest AF episode during a defined monitoring period[6].
利用研制的晶体管直流增益在线测试系统,以BCX41和3CK3B两种晶体管器件作为试验样品,在CFBR-II堆上开展了不同中子辐照注量效应试验,分别获得了辐照功率为2,20,200 W下晶体管的直流增益变化趋势,结果如图8—图10所示。


AF burden is a significant risk factor for clinical AF and stroke. A significant linear association is present between increased AF burden and the risk of stroke.
More emphasis should be laid on patients with AF burden to minimize the stroke risks.
ACKNOWLEDGEMENTS
We are grateful to Meng-Jiao He and Fei-Hong Chen for their helpful advice of methodology and statistics and to Mr. Satyajit Kundu for language polishing.
猜你喜欢
心理学报(2022年10期)2022-10-12
科学导报(2022年17期)2022-04-02
农业工程学报(2022年1期)2022-03-25
河南科技(2022年1期)2022-03-11
大自然探索(2021年7期)2021-09-26
湖北大学学报(自然科学版)(2021年5期)2021-08-20
北京航空航天大学学报(2021年6期)2021-07-20
江苏农业科学(2017年19期)2017-11-22
西江文艺(2017年15期)2017-09-10
信息化建设(2016年12期)2017-05-02
 World Journal of Clinical Cases2022年3期
World Journal of Clinical Cases2022年3期
- World Journal of Clinical Cases的其它文章
- Lung injury after cardiopulmonary bypass: Alternative treatment prospects
- Acute myocardial injury in patients with COVID-19: Possible mechanisms and clinical implications
- Anemia in cirrhosis: An underestimated entity
- High tumor mutation burden indicates a poor prognosis in patients with intrahepatic cholangiocarcinoma
- Does delaying ureteral stent placement lead to higher rates of preoperative acute pyelonephritis during pregnancy?
- Management of retroperitoneal sarcoma involving the iliac artery: Single-center surgical experience