
Successful response to camrelizumab in metastatic bladder cancer:A case report
2022-02-11 05:29ChenXieXiaYuanShuHuiChenZhiYongLiuDiLaLuFengXuZhiQiuChenXiaoMingZhong
World Journal of Clinical Cases 2022年1期
INTRODUCTION
Multiple studies have demonstrated that blocking of programmed death 1 (PD-1) or its ligand programmed death-ligand 1 (PD-L1) improved anti-tumor activity in metastatic urothelial cancer patients with disease progression after standard chemotherapy[1-3]. However, only a subset of patients is sensitive to immunotherapy. In addition to microsatellite instability (MSI) status and PD-L1 expression, tumor mutational burden (TMB), the third approved biomarker for immunosuppressant, could be used to predict the efficacy of immunosuppressive agents. Recently, increasing studies have indicated that there were no overlapping effects of PD-L1 expression and TMB on the response rate to PD-1/PD-L1 inhibitors across distinct tumor types, therefore they can be broadly used to categorize the immunologic subtypes of cancer[4].
Camrelizumab, as an anti-PD-1 inhibitor, provided an improved objective response rate (ORR) and disease control rate (DCR) in pre-treated patients with dMMR/MSIhigh (MSI-H) and advanced or metastatic solid tumor. Several clinical trials of camrelizumab for advanced urinary system tumors such as NCT03827837 have been launched. It brings more treatment options to patients with an advanced or metastatic solid tumor, including bladder cancer. Herein, we report the case of a recurrent bladder cancer patient with positive PD-L1 expression and high TMB. The patient received camrelizumab in combination with chemotherapy and achieved a partial response (PR).
CASE PRESENTATION
Chief complaints
A patient presented with recurrent metastatic bladder cancer (metastatic urothelial carcinoma, mUC), which demonstrated positive PD-L1 expression and high TMB.
History of present illness
A 74-year-old male patient, with a history of high-grade urothelial carcinoma of the bladder, was initially presented to our hospital in August 2017 due to gross hematuria and dysuria. Recurrence of bladder cancer was declared by computed tomography (CT) imaging. The patient was subjected to radical cystectomy and lysis of pelvic adhesions. The pathological evaluation of the tumor sample indicated infiltrating highgrade urothelial carcinoma of the bladder which invaded the entire layer and surrounding adipose tissue (Figure 1). Two months after surgery, the patient had pain in the right pubic bone while magnetic resonance imaging (MRI) revealed recurrence of stage IV bladder cancer with bone metastases.

History of past illness
The patient had a free previous medical history.
Physical examination
Vital signs and general inspection included the head, neck, anterior torso, posterior torso, anterior chest, abdomen, male genitalia, gait, station, coordination. Our clinical consideration was the recurrence of bladder cancer.
Laboratory examinations
Palliative radiotherapy in the metastatic site was given to the patient. In May 2018, the patient had pain of the right ilium and the symphysis pubis and received palliative radiotherapy followed by four cycles of chemotherapy with paclitaxel liposome (210 mg Q3W) from July 10, 2018 to September 12, 2018. Based on the high TMB level and positive PD-L1 expression, the patient was administered with immunotherapy of camrelizumab (200 mg, D0, q3w) in combination with chemotherapy including gemcitabine (1 g, D1 and D8, q3w) and cisplatin (40 mg, D1-D3, q3w) since October 2019.
High tumor mutation may lead to high neoantigen load and increased immunogenicity, which could promote recognition and killing abilities of the immune system. Multiple studies have shown that TMB is associated with the efficacy of mUC immunotherapy. A study indicated that tumor mutational load predicts survival after immunotherapy in mUC by the TMB cutoff of 17.6% or the cutoff of 25% by quartering[9]. The updated result of the PURE-01 study revealed that TMB may predict the pathological response to pembrolizumab in patients with muscle-invasive bladder cancer while a pretreatment TMB of 15 mutations/Mb was predictive of pathological complete response[10]. Another study showed that higher TMB levels revealed improved overall survival (OS) and lowered tumor recurrence[11]. Based on many relevant clinical studies, On June 16, 2020, the Food and Drug Administration approved pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastatic TMB-high [≥ 10 mutations/megabase (mut/Mb)] solid tumors.
The princess, his wife, although she had got her husband by a trick, found that she could not trick him, and so she never tried, but busied herself in teaching her children and scolding her maids
Imaging examinations
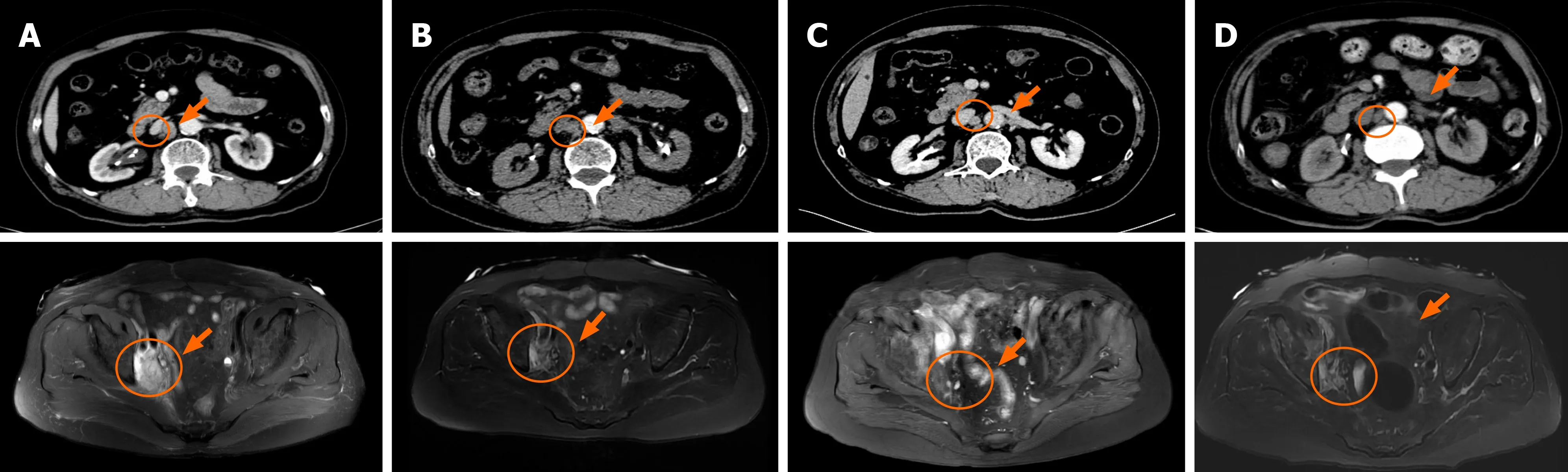
CT imaging and MRI were performed. In September 2019, the reexamination of abdominal CT identified multiple newly appeared swollen retroperitoneal lymph nodes in which the largest node had a diameter of about 1.7 cm (Figure 2A). After three treatment cycles, the patient achieved a PR as the repeated CT scan on December 20, 2019 showed a 53% decrease in the target lesion (Figure 2B). Then, the patient continued camrelizumab (200 mg, D0, q3w) and gemcitabine (1 g, D1, D8, q3w) and maintained the PR (Figure 2C and D).
FINAL DIAGNOSIS
Since the patient had pain in the right pubic bone with bone metastases, palliative radiotherapy in the metastatic site was given to the patient, followed by four cycles of chemotherapy with paclitaxel liposome (210 mg Q3W). Mild gastrointestinal reactions developed during paclitaxel liposome and immunotherapy of camrelizumab (200 mg, D0, q3w) in combination with chemotherapy with gemcitabine (1 g, D1, D8, q3w) and cisplatin (40 mg, D1-D3, q3w). Oppression in the chest, grade 1 myeloid suppression, and abnormal liver and kidney function occurred during the first gemcitabine and cisplatin chemotherapy, and gemcitabine dose was therefore reduced. In addition, abnormal liver function, moderate anemia, and mild gastrointestinal reactions occurred during the immunotherapy with camrelizumab and chemotherapy with gemcitabine and cisplatin. The patient maintained PR. The latest follow-up in October 2020 showed the progression of the tumor. The total progression-free survival (PFS) of the patient since camrelizumab therapy was 11 mo.
TREATMENT
Routine blood tests, routine urine tests and urinary sediment examination, routine fecal tests and occult blood tests, blood biochemistry, immune indexes, infection indexes immunohistochemistry (IHC) test, routine blood test genetic mutation profiling, and TMB evaluation were performed.
The plasma sample of the patient was subjected to genetic mutation profiling and TMB evaluation through next-generation sequencing (NGS) with a panel consisting of 520 cancer-related genes (Burning Rock Biotech, Guangzhou, China). The sequencing identified a total of 19 somatic mutations, including PIK3CA (p.Glu545Lys) andARID1A (p.Ser1948fs) mutations, and RAF1 amplification (CN = 3.6). The TMB level was 19.8 mutations per Mb. Furthermore, IHC on tissue samples indicated positive PD-L1 protein expression with a tumor proportion score (TPS) of 20%.
OUTCOME AND FOLLOW-UP
Recurrence of high-grade urothelial carcinoma of the bladder with bone metastases and multiple newly appearing swollen retroperitoneal lymph nodes.
DISCUSSION
Joyce Thomas comments on the trickery and imagery of the bone. The bone provides the imagery of deprivation112 and starvation, one of the primary themes of the tale. Also, the bone Hansel uses imitates the fate awaiting his flesh (the bone could well be the gnawed113 remains114 of the cage s previous occupant) (Thomas 1989).Return to place in story.
The application of immunotherapy has thoroughly promoted the progress of cancer treatment in recent years. However, 80% of patients with positive PD-L1 are unable to benefit from immunotherapy. Hitherto FDA has approved five drugs as immunotherapies for bladder cancer, but the ORRs of these drugs in bladder cancer are 13.4%-21.1%[5]. In clinical trials of camrelizumab in advanced solid tumors, some bladder carcinoma patients got a complete response[6]. Camrelizumab provided improved ORR and DCR in pre-treated patients with dMMR/MSI-H and advanced or metastatic solid tumor[7,8]. With the increase of approved immune checkpoint inhibitors, it is urgent to define patient subgroups that are more likely to have treatment benefits. PDL1, as the only effective biomarker for prediction, is far from being enough.
My day began on a decidedly sour(,) note when I saw my six-year-old wrestling with a limb of my azalea() bush. By the time I got outside, he d broken it. Can I take this to school today? he asked. With a wave of my hand, I sent him off. I turned my back so he wouldn t see the tears gathering1 in my eyes. I loved that azalea bush. I touched the broken limb as if to say silently, I m sorry.
School was finally out for the holidays and we were going Christmas shopping. Not for us, not even for friends, but for a little girl named Lauren. Lauren is a poverty-stricken five-year-old, and my family and our friends were buying Christmas presents for her that her family could not afford.
In addition, the NGS results of the patient revealed an inactivated nonsense mutation in ARID1A (p.Ser1948fs) which results in the loss of ARID1A protein expression and indicates potential treatment response to immunotherapy. ARID1A mutation has a high incidence in tumors, and it can increase the efficacy of tumor immunotherapy through multiple mechanisms of action, including MSI-H phenotype, high TMB, upregulation of PD-L1 expression, and immune activated tumor microenvironment. The largest study of 17486 patients with gastrointestinal tumors has demonstrated selective DNA damage repair (DDR) defects and ARID1A defects were associated with high TMB. In general, ARID1A was inactivated with increased TMB and low gene copy number, suggesting that it may be an indicator of immunotherapy[12]. Studies of immunotherapy for advanced urothelial carcinoma have shown that mutations in thegene are associated with improved PFS and OS[13]. Thegene is an independent factor associated with the efficacy of immunosuppressive therapy in mUC. In addition to high TMB (19.8 mutations per Mb) and positive PD-L1 expression (TPS 20%), the treatment benefit of camrelizumab observed in our case may also be explained by the change of thegene. Hence, the patient received immunotherapy in combination with chemotherapy and achieved a PR with a PFS of 11 mo.
In 1945, a 12-year-old boy saw something in a shop window that set his heart racing1. But the price—five dollars—was far beyond Reuben Earle s means. Five dollars would buy almost a week s groceries for his family.
More effective predictors of bladder cancer immunotherapy have yet to be explored, and the combination of multiple factors may be more predictive than a single factor.
CONCLUSION
Here, we report a Chinese patient with advanced bladder cancer showing effective treatment response to camrelizumab in combination with chemotherapy. This is the first case report on the treatment effect of camrelizumab for advanced bladder cancer with positive PD-L1 expression and high TMB. Our study suggested that TMB, PD-L1 expression, and DDR gene mutation can be used in combination to predict treatment effects of immunotherapy. More studies are needed to develop effective biomarkers and identify appropriate patient subgroups that are more likely to benefit from cancer immunotherapies.
World Journal of Clinical Cases2022年1期
- World Journal of Clinical Cases的其它文章
- Hepatitis B virus reactivation in rheumatoid arthritis
- Paradoxical role of interleukin-33/suppressor of tumorigenicity 2 in colorectal carcinogenesis: Progress and therapeutic potential
- Changes in rheumatoid arthritis under ultrasound before and after sinomenine injection
- Benefits of multidisciplinary collaborative care team-based nursing services in treating pressure injury wounds in cerebral infarction patients
- Outcomes and complications of open, laparoscopic, and hybrid giant ventral hernia repair
- Surgical resection of intradural extramedullary tumors in the atlantoaxial spine via a posterior approach