
Superior mesenteric venous thrombosis: Endovascular management and outcomes
2022-02-11 05:29KhaledAlnahhalBeauToskichSamuelNussbaumZhuoLiYoungErbenAlbertHakaimHoussamFarres
World Journal of Clinical Cases 2022年1期
INTRODUCTION
Acute mesenteric venous thrombosis accounts for 6% to 9% of mesenteric ischemia cases and 1 in 5000 to 15000 hospital admissions[1-3]. Superior mesenteric venous thrombosis (SMVT) is a rare condition but portends a mortality rate of up to 23%[4]. Risk factors for SMVT include hypercoagulable states, intra-abdominal surgery, infection, inflammation, and malignancy.
After checking all the exits, I found just enough room to squeeze under a gate in the rear of the school. I pushed my purse through first, lay on my back and slowly edged through.
Systemic anticoagulation in addition to laparotomy for presentations with peritonitis represent conventional approaches to treating SMVT[3,5,6]. Endovascular therapy, such as thrombolysis and/or thrombectomy, is typically used as adjunctive treatment when medical management has failed. To date, most studies that explore endovascular treatment of SMVT have been case reports and small case series. More information regarding this treatment is needed.
This study aims to report on this rare condition to expand the literature base and evaluate the endovascular therapies effects on technical and clinical outcomes on 24 patients diagnosed with SMVT from a large tri-center institution.
MATERIALS AND METHODS
Study design
A retrospective search of the Mayo Clinic Health System electronic medical record and imaging report archive was performed. All patients age 18 years and older who were diagnosed with isolated SMVT or SMVT combined with portal vein thrombosis as an inpatient and underwent both medical and endovascular treatment between January 2000 and December 2019 were included for analysis. Patients were excluded if they did not have sufficient follow-up data of at least 1 mo. Patients with peritonitis were not included in this study as these patients are taken to an operating room and would not undergo endovascular treatment. Twenty-four patients were identified and met our criteria. Patient demographics, presenting symptoms, date of symptom onset, risk factors for SMVT admission and endovascular intervention, endovascular modality(s), technical and clinical outcomes, patency rates, and length of stay. The adverse events were evaluated and reported per Clavien-Dindo classification. The follow-up was until last clinical note recorded in the patients’ medical record.
Interventional procedures
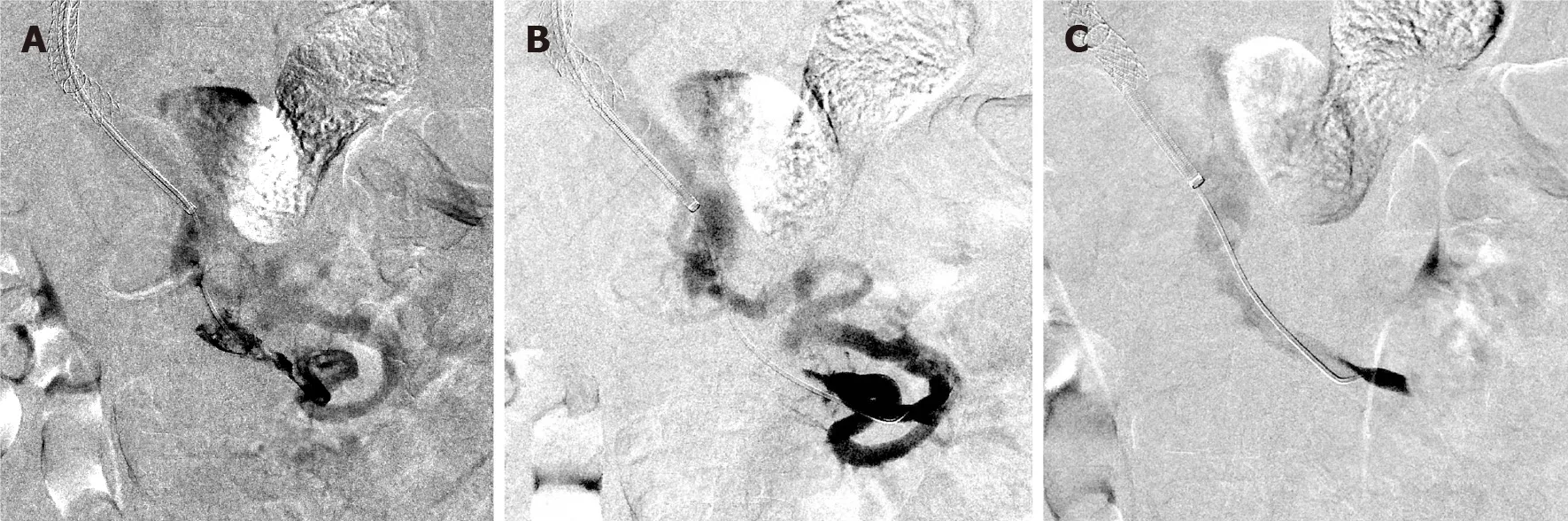
Endovascular therapy was initiated after failure of systemic anticoagulation, determined by a lack of clinical improvement (Figure 1). The anticoagulation management was unfractionated heparin or low-molecular-weight heparin started at the time of diagnosis. Percutaneous transhepatic and/or transjugular approaches were used for all interventions. The selection between approaches was operator dependent.
Pharmacomechanical thrombectomy was performed in most patients who underwent thrombectomy using either rheolysis (AngioJet, Boston Scientific Corporation) or aspiration thrombectomy (Penumbra CAT 8 device, Penumbra Inc.). Catheter-directed thrombolysis (CDT) was performed using a multiple side-hole infusion catheter that extended into the thrombosed SMV. Tissue plasminogen activator was used as thrombolytic agent that initiated at an infusion rate of 0.5-1 mg/h in most patients who underwent thrombolysis for a duration ranging from 24 to 72 h with a low-dose heparin infusion at a standard rate of 500 units/h. Other endovascular techniques were employed when lysis and thrombectomy alone were insufficient including transjugular intrahepatic portosystemic shunt creation (TIPS), which was used if there was significant residual underlying portal hypertension after thrombectomy (portal pressure gradient > 12 mmHg) or if there was evidence of rethrombosis related to poor intrahepatic portal perfusion; balloon angioplasty, and self-expanding or balloon-expandable stents were deployed when a persistent flowlimiting lesion (> 50% stenosis) was present after angioplasty.
Study end points and definitions
In our study, percutaneous thrombectomy was used to treat 14 patients, most commonly using pharmacomechanical thrombectomy through rheolysis and less commonly using aspiration thrombectomy, either in combination with other modalities, especially CDT, or alone, in case CDT was contraindicated or not indicated. Rabuffi[10] evaluated the outcomes of 8 patients who were treated by a pharmacomechanical thrombectomy, and showed survival rate of 87.5% and a 12.5% major complication rate at mean follow up of 37 mo, compared to 78.6% and 7.1% in our study at median follow-up of 23 mo.
Statistical analysis
Continuous variables were summarized as median (range) and quartiles while categorical variables were reported as frequency (percentage). The Kaplan-Meier method was used to estimate primary patency and overall survival using R version 3.6.2 (https://www.r-project.org).values were considered statistically significant if< 0.05. The statistical methods of this study were reviewed by Li Z, MS from Mayo Clinic.
RESULTS
Clinical presentation and baseline characteristics
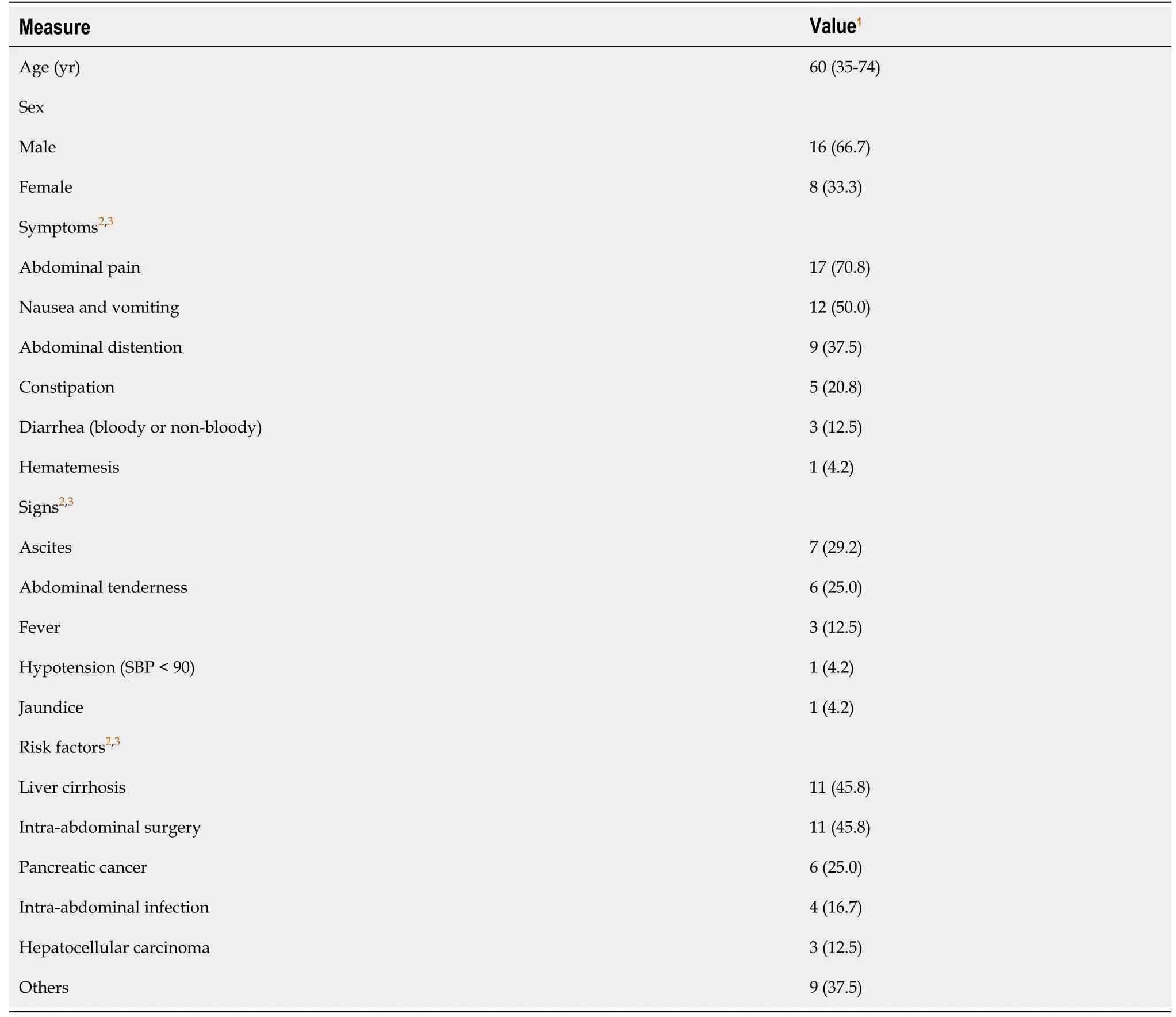
The study population consisted of 24 patients (Table 1). The median age at intervention was 60 years (35-74 years) and 67% (= 16) were men. The median time between presentation to hospital and intervention was 3 d (0-15 d), while the median time from symptom onset to intervention was 8 d (2-35 d). Of 79.2% (= 19) patients presented with acute symptoms while acute on top of chronic symptoms occurred in 20.8% (= 5) of the patients. The most common SMVT risk factors were history of intra-abdominal surgery (= 11, 45.8%), liver cirrhosis (= 11, 45.8%), and malignancy (= 11, 45.8%). Patients presented primarily with abdominal pain 70.8% (= 17), and nausea and vomiting 50% (= 12).
Laboratory tests, imaging, and treatment modalities
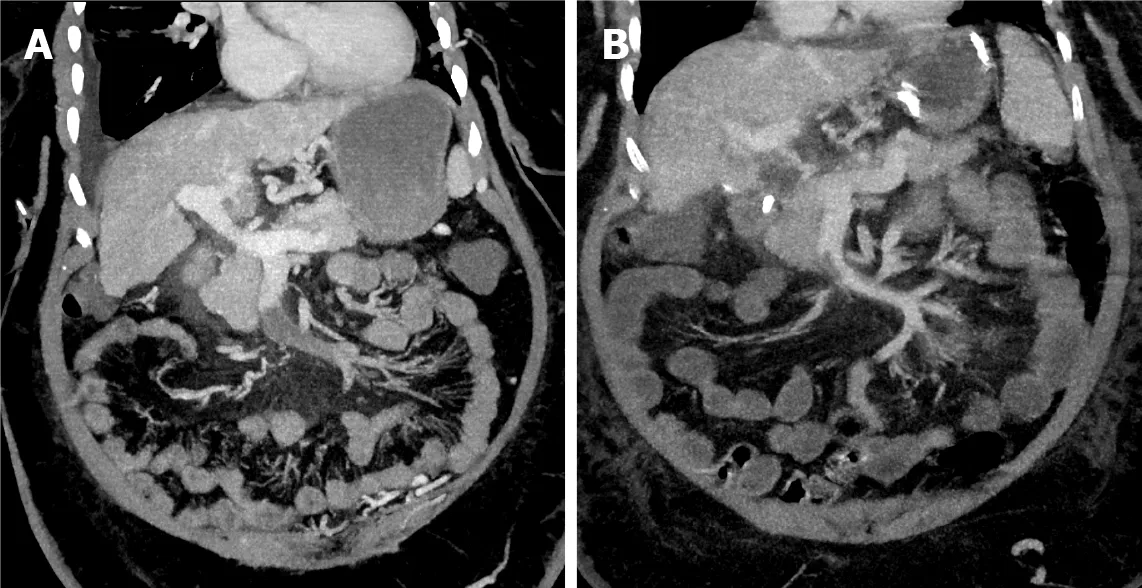
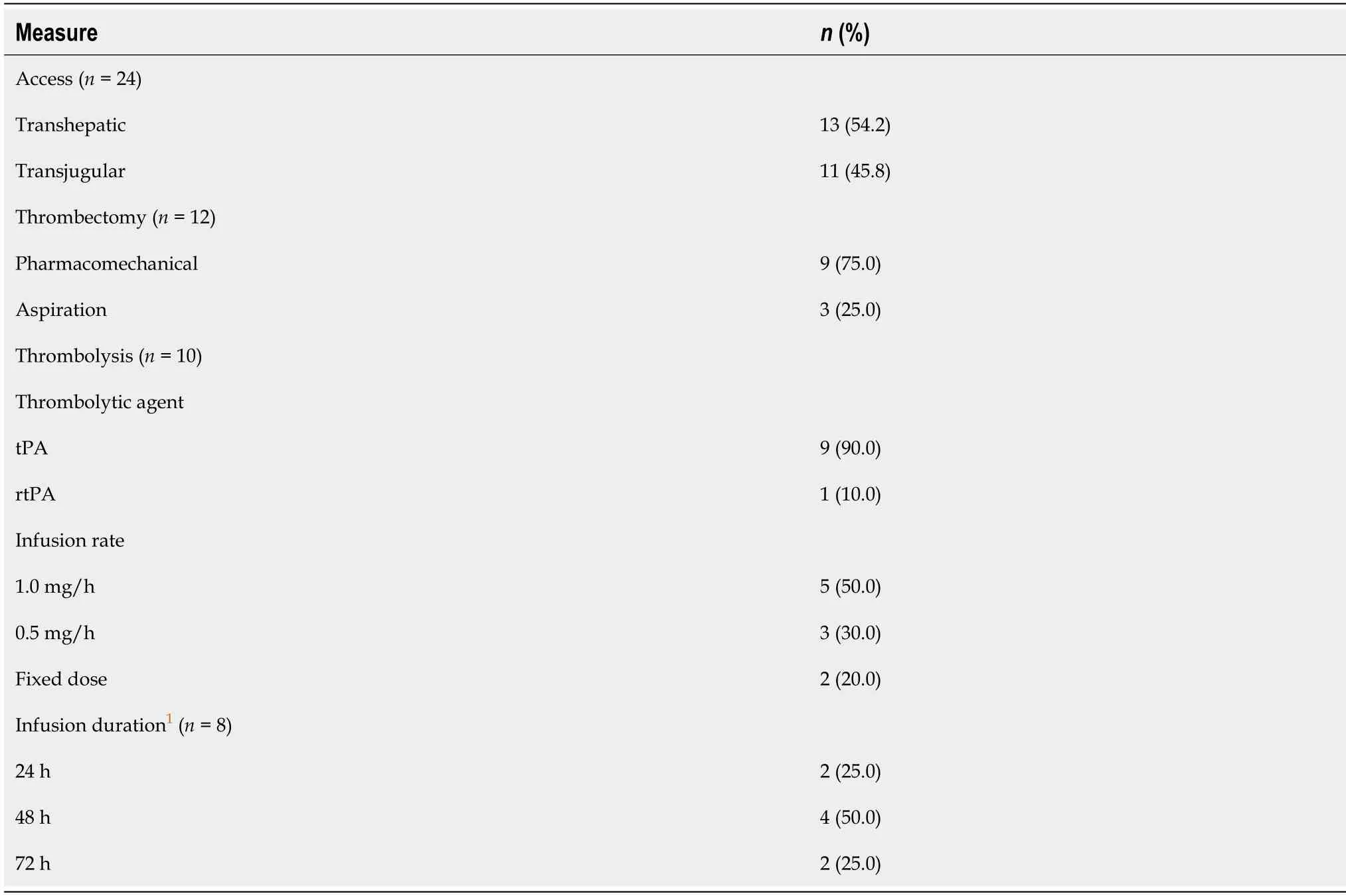
All 24 patients received at least one endovascular modality, while 13 (54.2%) received a combination of treatments (Table 2). Thrombectomy was the most commonly used, which was attempted in 50% (= 12), Out of 12 patients, a pharmacomechanical system (AngioJet device; Boston Scientific Corporation) was performed in 75% (= 9) and aspiration thrombectomy was employed in 25% (= 3) (Figure 2). CDT was attempted in 41.7% (= 10) of the patients, where CDT alone was in 4 patients and in combination with other modalities in 6 patients. In patients who received CDT, eight were treated with tissue plasminogen activator with an infusion rate of 0.5 to 1.0 mg/h over 24 to 72 h and 2 patients received fixed doses of recombinant tissue plasminogen activator (Table 3).
Only 54.2% (= 13) patients had a reported lactate level at presentation, of them, 23.1% (= 3) have hyperlactatemia with a median level of 1.4 mmol/L (range, 0.8-4.8 mg/dL). While 91.7% (= 22) had a reported white blood cell count, where 13.6% (= 3) have leukocytosis with a median count of 9.2 (× 10/L; range, 3.5-21.9 × 10/L). Computed tomography was the most frequently used imaging modality [62.5% (= 15)] followed by the magnetic resonance angiography used in 37.5% (= 9). Among 24 patients, only 2 had isolated SMVT while the portal vein was involved in the other 91.7% (= 22). The distal part of the SMV (defined as the part of the SMV near the tributaries) was involved in 66.7% (= 16), the proximal end (defined as the portion of the SMV proper without tributaries) was involved in 12.5% (= 3), and 20.8% (= 5) had both proximal and distal involvement.
20. That is my house and yours, where we shall live together: A house can represent the family line (Biedermann 179). According to Jung, What happens inside it, happens within ourselves (Biedermann 179). Freud associates the house with the woman, the mother, in a sexual or childbearing sense (Biedermann 179).
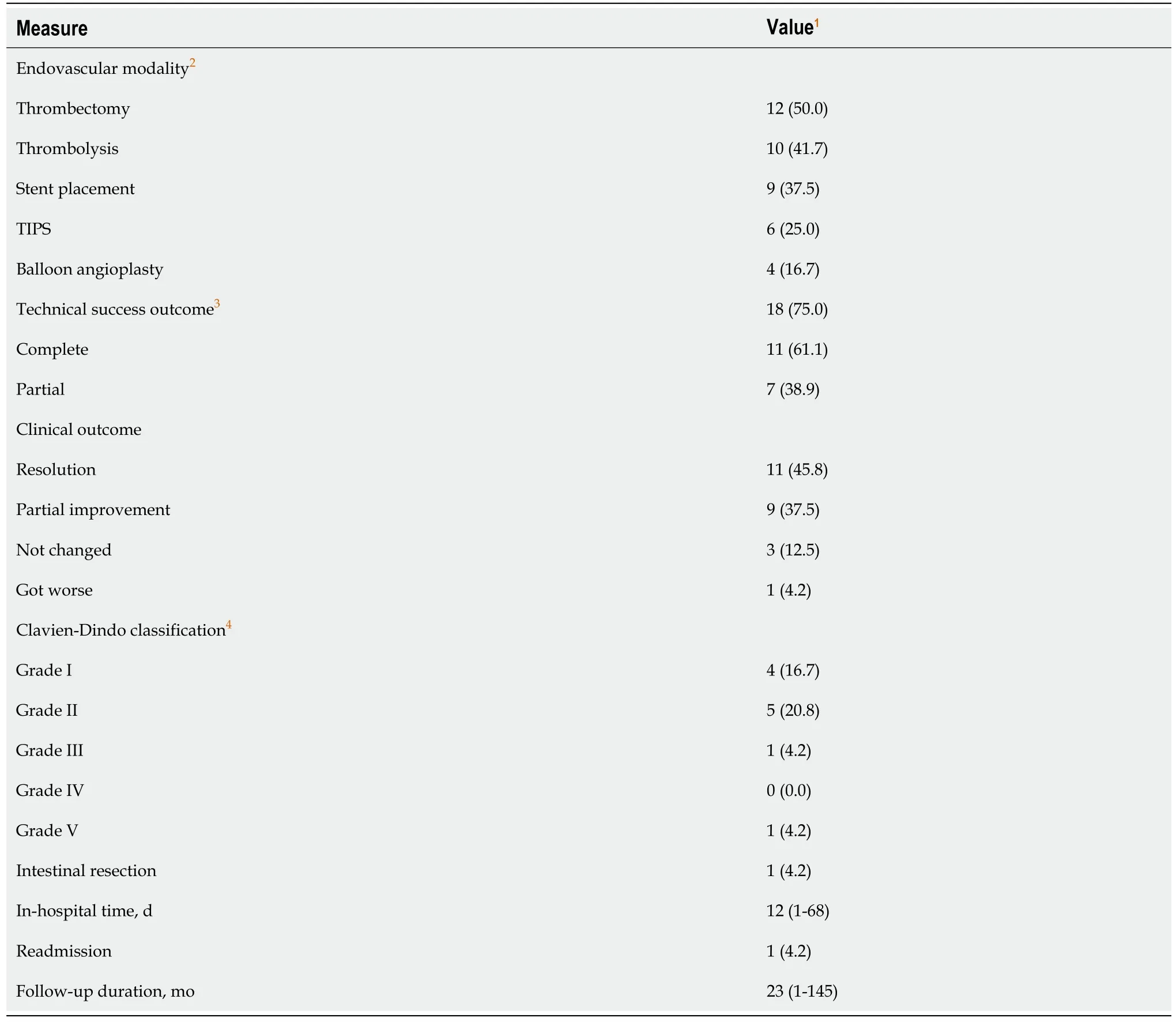
Other treatment modalities were also employed, including stents placed in 37.5% (= 9), TIPS created in 25.0% (= 6), and balloon angioplasty alone performed in 16.7% (= 4). All patients that had a TIPS creation received an intrahepatic stent.
Success rates and follow-up data
Since the presenting symptoms of SMVT are not specific (, abdominal pain and nausea and/or vomiting), early detection and diagnosis of the condition is challenging, leading to a delay in initiating management; thus, more dangerous consequences can emerge, such as intestinal and bowel infarction. The delay of management in these patients is also due to the failure of anticoagulation which is always the first line of treatment before moving to endovascular therapy and explains the 3-d median time of presentation-to-intervention that was found. Endovascular therapies are becoming increasingly used, however, the data available regarding their use in literature is insufficient[9-12].
In a study that included 43 patients who were treated for their ASMVT using multidisciplinary stepwise management, endovascular CDT was performed in 83% (= 36) patients with or without adjunctive procedures, 20 as an initial procedure and 16 were postoperatively, their recanalization rate was 94.44% (75% in this study). Bowel resection was required in 18 patients, with 30-d mortality and overall inhospital mortality rates of 11.63% and 16.28%, respectively. The overall 1-year survival was 83.72% (82% 5-year survival rate in our study)[16].
Some modern interpretations95 of the tale, such as Shannon Hale s excellent novel, explain that the Goose Girl doesn t reveal her true identity because she fears no one will believe her. She awaits the best opportunity to reveal her identity with the least amount of blood shed available.
A total of 6 patients (25%) died at some point during the study, four of which (16.7%) died before the median follow up time of 23 mo. Five-year overall survival rate was 82% (58%-100%).
DISCUSSION
SMVT is associated with high rates of morbidity and mortality[1]. Our study described and evaluated the outcomes of endovascular treatment of SMVT in 24 patients, with either acute thrombosis or chronic thrombosis with acute symptoms. The acute onset usually presents with crampy upper, middle, or lower-middle abdominal pain in addition to nausea, anorexia, vomiting, diarrhea, and/or bloody stool. Features of portal hypertension are usually reported in the chronic onset[7,8].
When the grey women heard that laugh they began to weep, for now they knew that a stranger had robbed them, and that they could not help themselves, and their tears froze as they fell from the hollows where no eyes were, and rattled20 on the icy ground of the cave
Technical success was achieved in 18 of 24 patients. In these patients, 61.1% (= 11) achieved complete recanalization, and 38.9% (= 7) were established partial recanalization. Three patients underwent more than 1 endovascular intervention: 2 of them with technical success. Out of the 11 patients that had liver cirrhosis, 9 achieved technical success; with only one patient having primary patency failure, and three patients died by the end of the study. An 83.3% (= 20) of the patients demonstrated clinical improvement 48 h following the procedure (Table 2). A single patient experienced symptom progression after intervention.
The end points of the study were to determine both the short- and long-term technical success, and the clinical outcomes of using the endovascular therapeutic options in treating patients diagnosed with SMVT. Short-term technical success was measured as any improvement in SMV flow per completion angiography at the time of intervention. The long-term technical success was represented by the primary and secondary patency rates. Primary patency was defined as the interval from reestablishing initial mesenteric venous flow until the first thrombotic event, seen through ultrasound imaging follow up, or additional intervention. Secondary patency was defined as successful restoration of flow after thrombosis post reintervention until rethrombosis or last follow-up. Portal involvement defined as any thrombus extension into the main portal vein. The clinical outcomes were assessed by reporting the clinical status of the patient at 1 to 2 d following the procedure, reporting the adverse eventsClavien-Dindo classification, and showing the 5-year survival rate.
Endovascular intervention with anticoagulation appears to be effective at managing SMVT and may be considered as first-line therapy along with systemic anticoagulation in select patients.
Many studies investigating the endovascular thrombolytic therapies have been reported. Andraska[13] exhibited that thrombolysis achieved a rate of complete or partial recanalization of 91.6% in patients who received this treatment modality alone. Another study[14] evaluated outcomes of performing CDT in 20 patients, demonstrated a complication rate of 60%, and 1 death during hospitalization due to gastro-intestinal hemorrhage and septic shock. In our study, the primary patency was established in 5 of the 6 patients who were treated with CDT combined with other modalities. On the other hand, 3 out of 4 patients who were treated with CDT alone did not reestablish flow. Of those patients, two developed complications, 1 underwent surgical bowel resection after the procedure and the other patient developed a large subcapsular hematoma and subhepatic intraperitoneal hemorrhage. The latter patient had an emergent endovascular embolization where 14 units of packed red blood cells were given, and the patient was transferred to the intensive care unit where he died 6 d later. Their lactate level was 4.8 mmol/L, supporting the evidence that lactic acidosis can be associated with higher likelihood of requiring bowel resection[13]. The 13 patients, who received one or more endovascular treatment modality other than the CDT, had a technical success of 92% and none of them underwent bowel resection after the endovascular procedure.
Yang[14] found among 13 cases who are treated with transcatheter thrombolysis, 4 cases required small bowel resection due to localized bowel infarction and secondary stricture. In our study, only 1 patient, who was still symptomatic for abdominal pain despite the thrombolysis for 72 h, underwent resection of proximal one-third of the jejunum and an ostomy placement after the thrombolysis therapy, which denotes the early detection and diagnosis of the condition and the rapid intervention as well.
TIPS was performed in 9 patients, can be helpful through creating a low-pressure system that assists in the removal of the clots in combination with other treatment modalities such as CDT[10]. Neither hepatic encephalopathy nor pulmonary embolism developed in any of these patients, although TIPS can increase the risk of these complications[10,15].
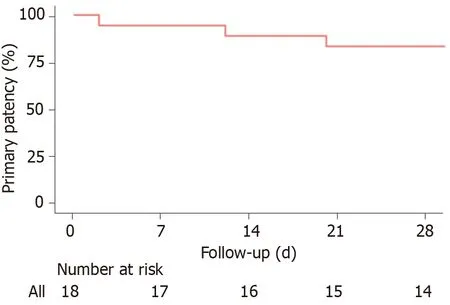
Median follow-up of the patients was 23 mo (range of 1-145). The median length of stay was 12 d (range of 1-68 d). Primary patency at 14 and 30 d were 88.9% (95%CI: 76%-100%) and 83.3% (95%CI: 68%-100%), respectively (Figure 3). Adverse events were identified in 8.3% (= 2) of patients, one marked as grade IIIB, and 1 death marked as grade V. One patient underwent partial small bowel resection, and the second patient had a subcapsular hematoma and intraperitoneal bleeding and died after 6 d.
In our study, primary and secondary patencies were reported and those outcomes are not measured in other studies as far as we know. The high rates of the 30-d primary and secondary patencies of 83.3% and 88.9%, respectively, signify the safety and efficacy of using the endovascular interventions in treating those patients; however, the scale used in showing the patency rates and drawing the Kaplan-Meier curve for the primary patency was in days due to rapid occurrence of the rethrombosis events of those 3 patients.
Without a doubt, it was the best wedding gift I received. One I would never forget. My father showered me with his gifts every day of his life. How did I get so lucky?
Limitations of our study included its retrospective design. Conducting a large scale randomized controlled trial is not feasible because SMVT is a rare condition and the mechanism for SMVT is variable along with the ethics of trial design in withholding therapy to patients not responding to anticoagulation. Indeed, a study of 24 patients who were diagnosed with an uncommon condition is not considered a small study compared to the studies found in the literature, which are mostly case reports and very small case series. However, with this number of patients (= 24), conducting a statistical analysis was not possible. Overall, despite the aforementioned limitations, our study’s findings show that endovascular management for SMVT was associated with high thrombus resolution rates and improvement in patients’ clinical outcomes. Further large prospective study is still warranted to provide more significant data about the outcomes of endovascular therapies.
CONCLUSION
Late in the autumn, when the weather was rough, windy, and wet,and the cold penetrated through the thickest clothing, especially atsea, a wretched boat went out to sea with only two men on board, or,more correctly, a man and a half, for it was the skipper and hisboy
But dinner does not take very long when you are all by yourself, and very soon she sat down cosily56 in the corner of a sofa, and began to think about the charming Prince she had seen in her dream
ARTICLE HIGHLIGHTS
Research background
Superior mesenteric venous thrombosis (SMVT) is a rare but deadly condition with mortality rates of up to 23% that is typically treated with anticoagulation therapy and endovascular treatment if this fails.
Gretel is not the only fairy tale sister to rescue her brother. Also read Brother and Sister and The Six Swans on SurLaLune to read tales in which sisters rescue their brothers from spells or death.
Research motivation
Most existing studies looking into endovascular of SMVT are small case series and case reports, and as such more information is needed on treatments for this rare condition.
Research objectives
This study aimed to evaluate patients diagnosed with SMVT who received endovascular therapy in addition to anticoagulation and report technical and clinical outcomes.
Research methods
A retrospective analysis of the patients who underwent endovascular treatment for SMVT at Mayo Clinic from 2000-2019 was performed. We explored the success of these endovascular treatments by determining technical success in each case, defined as any improvement in SMV flow following recanalization, and by assessing the primary/secondary patency rates.
Research results
Twenty-four patients were included for analysis. Of these patients, 19 presented with acute thrombosis, while 5 presented with chronic thrombosis with acute manifestations.The most commonly used endovascular modalities were thrombectomy in 12 patients and catheter-directed thrombolysis in 10 patients. Technical success was achieved in 75% of patients, and the 14-d and 30-d patency rates were 88.9% and 83.3%respectively. The 5-year overall survival rate was 83%.
She sprang to the door and would have run away, but on the stairs a man caught her and brought her back; and when she looked at him it was King Thrushbeard again
Research conclusions
Endovascular interventions in addition to anticoagulation therapy appears to be effective in treating SMVT and may be considered a first-line therapy in select patients.
Research perspectives
Our research helps build the base of literature on the rare condition of SMVT by providing an evaluation of the technical and clinical endovascular management outcomes. Larger prospective studies looking into the long-term outcomes of these endovascular interventions and anticoagulation therapy may be a future research direction.
World Journal of Clinical Cases2022年1期
- World Journal of Clinical Cases的其它文章
- Hepatitis B virus reactivation in rheumatoid arthritis
- Paradoxical role of interleukin-33/suppressor of tumorigenicity 2 in colorectal carcinogenesis: Progress and therapeutic potential
- Changes in rheumatoid arthritis under ultrasound before and after sinomenine injection
- Benefits of multidisciplinary collaborative care team-based nursing services in treating pressure injury wounds in cerebral infarction patients
- Outcomes and complications of open, laparoscopic, and hybrid giant ventral hernia repair
- Surgical resection of intradural extramedullary tumors in the atlantoaxial spine via a posterior approach