
Evaluation of right-to-left shunt on contrast-enhanced transcranial Doppler in patent foramen ovale-related cryptogenic stroke:Research based on imaging
2022-02-11 05:28LeiXiaoYanHongYanYaFangDingManLiuLiJuanKongChunHongHuPinJingHui
World Journal of Clinical Cases 2022年1期
INTRODUCTION
Ischemic stroke is more common than hemorrhagic stroke[1]. Cryptogenic stroke (CS), a subtype of ischemic stroke with no determined etiology after an extensive investigation, accounts for 40% of all types of ischemic stroke[2,3]. Seeking the underlying causes of CS can guide treatment and reduce or prevent the reoccurrence of stroke. Previous studies have indicated that patent foramen ovale (PFO) occurs in approximately half of CS patients, particularly among those who are of young age[4-6]; moreover, this percentage is considerably higher than in the normal healthy population. Paradoxical embolism caused by right-to-left shunt (RLS) of a PFO is considered an important pathogenesis for CS[7,8].
So he begged his father to let him have a ship for the voyage, set sail with a favourable9 wind, and after a time landed in the country where Signy lived
CS patients with PFO show characteristic infarction patterns on diffusion-weighted imaging (DWI), as compared to CS patients without PFO. This characteristic becomes more obvious as the grade of shunt increases on contrast-enhanced transcranial Doppler (c-TCD)[9-11]. In latent RLS, microbubbles are detected on c-TCD only after the valsalva maneuver (VM), whereas in permanent RLS, microbubbles are also detected at rest[12]. In this study, we sought to determine the relationship between RLS on c-TCD and the infarction pattern on DWI in PFO-related CS patients when combining the type and grade of RLS. The RLS grade evaluated by c-TCD was compared to the size of PFO determined by transesophageal echocardiography (TEE).
MATERIALS AND METHODS
Study population
We retrospectively evaluated CS patients who attended the stroke center at the First Affiliated Hospital of Soochow University within 72 h from onset of symptoms. The study was carried out from August 2015 to December 2019. According to the TOAST criteria, CS is defined upon determination of no specific cause after an extensive evaluation[2]. The data for study included findings from clinical examinations, standard laboratory tests, brain imaging (computed tomography and magnetic resonance imaging), vascular imaging (color-coded duplex sonography, magnetic resonance or conventional angiography), 12-lead and 24 h electrocardiographic analyses, and echocardiographic analysis.
During the study period, 238 of the ischemic stroke patients admitted to our center had been diagnosed with CS. Of these, 148 underwent examination by c-TCD and TEE; the 16 patients among them who did not complete c-TCD or TEE detection due to poor cardiac or pulmonary function and a poor condition of temporal window or median cubital vein were excluded. Additionally, 12 patients with a negative result for both c-TCD and TEE, 6 patients with pulmonary arteriovenous malformation (detectedcomputed tomography pulmonary angiography[13]) and 3 patients with aortic arch disease and other sources of cardioembolism (detected by transthoracic echocardiography[14]) were excluded. Finally, a total of 111 CS patients with PFO were included in the current study (Figure 1).

For all included patients, findings from DWI of brain magnetic resonance imaging and TEE detection were assessed. A normal control group of 33 patients with simple dizziness who were age-matched to the included CS patients and admitted to hospital in the corresponding period were chosen. The normal control group had no neurological signs, no cerebral infarction, and negative c-TCD. The baseline characteristics and laboratory tests were evaluated to determine differences between PFOrelated CS patients and the normal control group.
c-TCD and RLS assessment
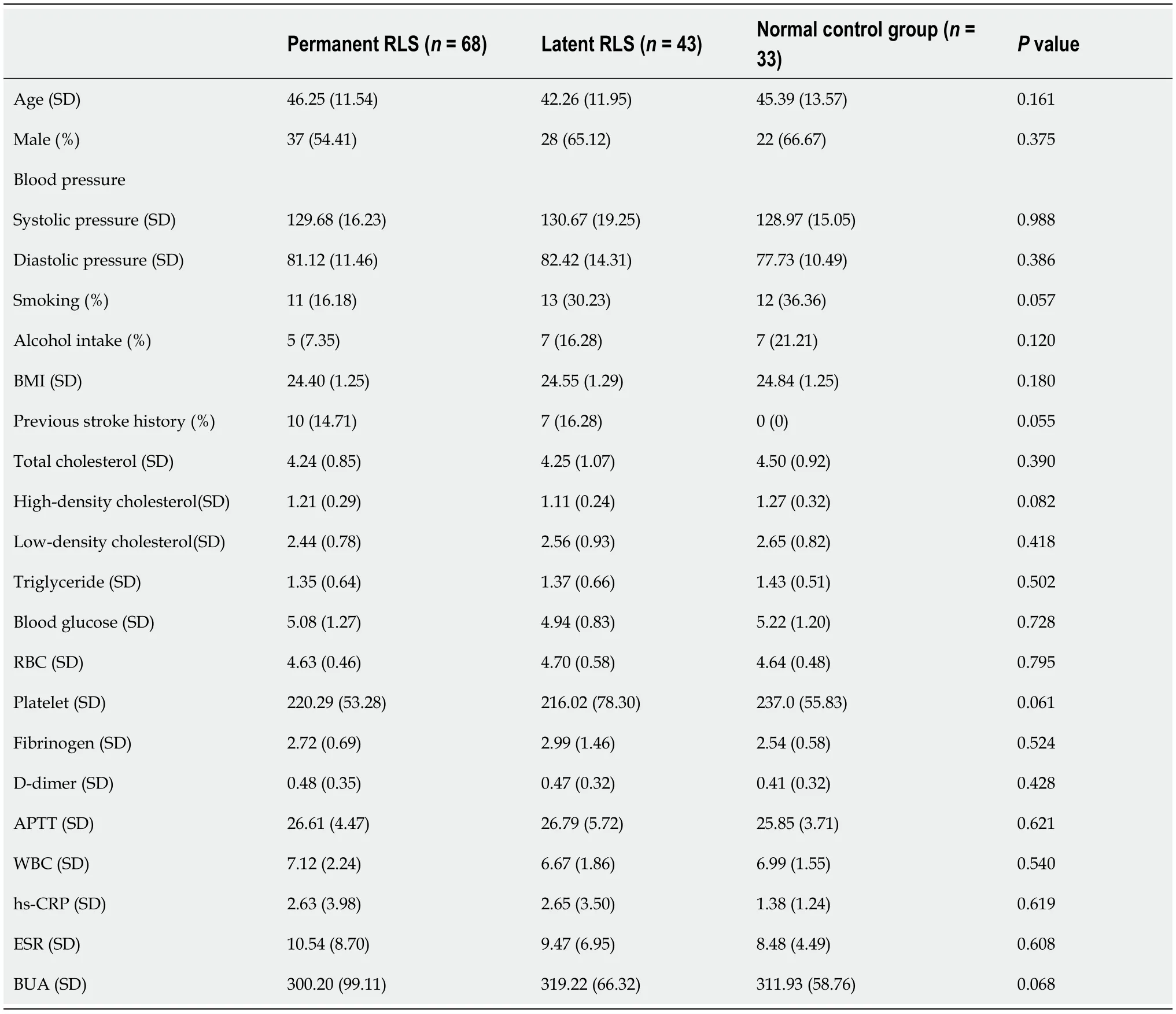
A total of 68 patients (61.26%) were classified as having permanent RLS and 43 patients (38.74%) as having latent RLS based on c-TCD. The differences in age, sex, blood pressure, smoking, alcohol intake, body mass index and history of stroke did not reach statistical significance in comparison between the CS patients with permanent or latent RLS and the normal control group. We then analyzed the findings from laboratory tests and observed no statistically significant differences among the three groups for blood lipid parameters, blood glucose, blood cell count, coagulation indicators, inflammatory biomarkers, and blood uric acid (Table 1).
CS patients with multiple, small and cortical infarcts should be advised to receive c-TCD to determine RLS induced by PFO. Multiple territory infarcts indicate permanent RLS, while posterior circulation infarcts may indicate latent RLS. This infarction pattern suggests that distribution of the infarct may provide clues for c-TCD screening of PFO.
The inspection result in each state was recorded using a five-level categorization system[6] based on the number of MBs observed, as follows: Grade 0, negative; Grade I, 1 ≤ MBs ≤ 10; Grade II, 10 < MBs ≤ 25; Grade III, > 25 MBs and no curtain; and Grade IV, curtain, a single MBs could not be identified. To improve the analysis, we further categorized the CS patients based on the level of the shunt, as follows: small RLS, Grade I; mild RLS: Grade II; large RLS, Grade III and IV.
TEE and PFO assessment
TEE was performed using a cardiac ultrasound machine (Vivid E9; GE Healthcare, Chicago, IL, United States) with a 6VT-D transesophageal probe at a frequency range of 3.0-8.0 MHz. All patients were examined in a fasting state. For each, after local pharyngeal anesthesia was applied (10% topical lidocaine spray), the probe was quickly inserted into the esophagus through the mouth until it reached the pharynx. The width of the fissure between the primary septum and secondary septum was measured as the size of PFO in all confirmed PFO patients.
Brain imaging assessment
Brain magnetic resonance imaging was conducted within 24 h of admission for all patients by use of a MAGNETOM Skyra 3T system (Siemens, Munich, Germany). The obtained DWI images were reviewed by experienced neuroradiologists (including Chief Physician) who were blinded to the study groups.
The ischemic lesions were classified based on the amount (single or multiple) and size (small: < 1 cm diameter; large: > 1 cm diameter)[11]. According to the vascular territory involved, the lesions were divided into anterior circulation, posterior circulation and multiple territories[11]. The lesions were also classified based on cortical involvement (only-cortical, cortical-subcortical, and only-subcortical). We further synthesized and divided the infarction patterns into single territory single lesion, single territory multiple lesions, multiple territories small scattered lesions, and multiple territories large and small lesions, in accordance with a previous study[17].
Statistical analysis
As previously reported, RLS is regarded as a common cause of CS in young and middle-aged adults[18,19]. In the current study, we observed that the average age of CS patients was < 55 years. Krassen[20] indicated that PFO was more prevalent in men with CS than in women with CS. However, the same was not observed in the current study. Furthermore, the vascular risk factors of CS patients were evaluated. We found no significant difference between CS patients with permanent RLS and latent RLS and the normal control group. The results indicated that other mechanisms of stroke, such as paradoxical embolism, may exist in these patients, which was similar to findings of previous studies[11,21].
For future research, we will continue to study the mechanism of stroke in patent foramen ovale (PFO)-related cryptogenic stroke (CS) patients, and we plan to cooperate with other stroke centers to expand the range of sample selection and sample size. This will allow more accurate and clinically consistent research results.
What I hadn’t counted on were the people with enormous orders who chose to use the drive-thru window, or the women who felt that the coffee was much too creamy, or the men who wanted their iced coffees remade again and again until they reached a certain level of perfection. There were moments when I was exasperated4 with the human race as a whole, simply because I couldn’t seem to please anyone. There was always too much sugar, too little ice, and not enough skim milk. Nevertheless, I kept at it.
RESULTS
Clinical characteristics and laboratory tests
All examinations performed by TCD detector (EMS-9PB; Shenzhen Delica Medical Equipment, Shenzhen, China) were conducted by an experienced neuroscientist (> 300 case experience). In practice, with the patient lying in the supine position, a handheld 1.6 MHz probe was placed at the left temporal window to monitor the middle cerebral artery. The single-channel dual-depth mode was selected, with two depths (48-52 mm and 60-64 mm) having a depth difference of 12 mm. The detector was set to a sample volume of 10 mm (of note, the depth difference should be greater than the sample volume) and a low gain for embolus to distinguish from the background spectrum.
Infarction pattern of PFO-related CS
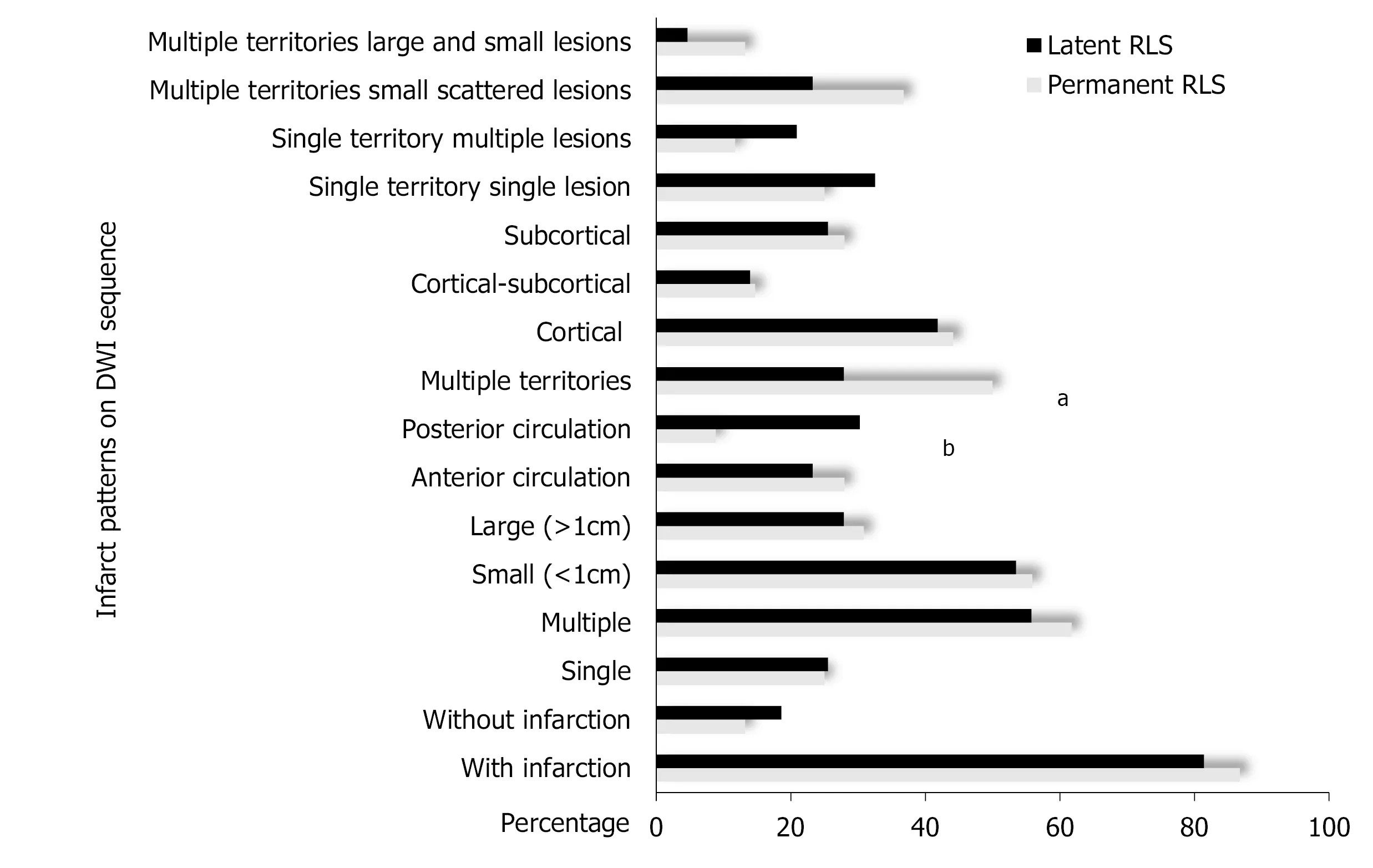
The DWI lesions of CS patients with different types and grades of RLS were compared and analyzed. First, the DWI lesions were compared between the permanent RLS group and the latent RLS group. In the permanent RLS group, 86.76% of the patients showed DWI lesions; in the latent RLS group, 81.40% of the patients showed DWI lesions. These rates were not significantly different between the two groups. We also found no significant differences in the number, size and cortical involvement of DWI lesions between the permanent RLS group and the latent RLS group. The proportion of patients with multiple territory lesions in the permanent RLS group (50.00%) was significantly greater than that in the latent RLS group (27.91%;= 0.021). However, the latent RLS group was more likely to show an effect on posterior circulation (= 0.004) (Figures 2 and 3).
We then subcategorized the permanent RLS and latent RLS groups into small RLS, mild RLS and large RLS according to the grade of shunt on c-TCD. In the permanent RLS group, 18 patients had small RLS, 13 patients had mild RLS, and 37 patients had large RLS. The proportion of patients with DWI lesions was 72.22% in the small RLS subgroup, 84.61% in the mild RLS subgroup, and 94.59% in the large RLS subgroup (t= 0.022). The proportion of multiple lesions was 44.44% in the small RLS subgroup, 53.85% in the mild RLS subgroup, and 72.97% in the large RLS subgroup (= 0.035). The proportion of small lesions was 33.33% in the small RLS subgroup, 53.85% in the mild RLS subgroup, and 67.57% in the large RLS subgroup (= 0.017). The proportion of multiple territory lesions was 27.78% in the small RLS subgroup, 46.15% in the mild RLS subgroup, and 62.16% in the large RLS subgroup (= 0.017). Cortical involvement varied from 22.22% in the small RLS subgroup to 46.15% in the mild RLS subgroup and 54.05% in the large RLS subgroup (= 0.031). The grade of RLS also showed a positive tendency with multiple territories and small scattered lesions, varying from 16.67% in the small RLS subgroup to 38.46% in the mild RLS subgroup and 45.95% in the large RLS subgroup (= 0.041) (Figure 4A).
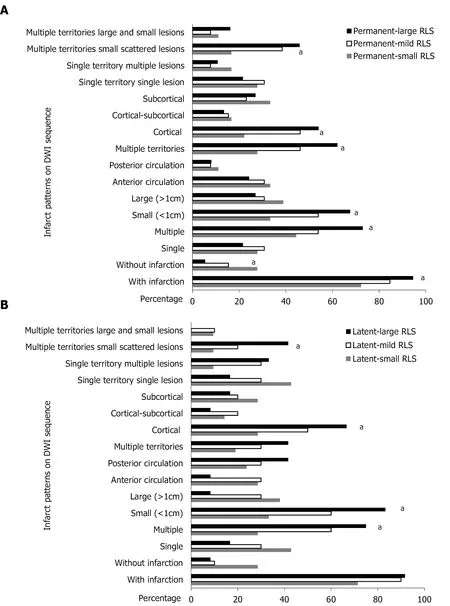
In the latent RLS group, 21 patients had small RLS, 10 patients had mild RLS, and 12 patients had large RLS. No statistically significant difference was found for the proportion of patients with DWI lesions and the distribution of lesions according to the different grades of RLS. The proportion of multiple lesions varied from 28.57% in the small RLS subgroup to 60.00% in the mild RLS subgroup and 75.00% in the large RLS subgroup (= 0.009). The proportion of small lesions varied from 33.33% in the small RLS subgroup to 60% in the mild RLS subgroup and 83.33% in the large RLS subgroup (= 0.006). The proportion of cortical involvement varied from 28.57% in the small RLS subgroup to 50.00% in the mild RLS subgroup and 66.67% in the large RLS subgroup (= 0.033). Multiple territory and small scattered lesions varied from 9.52% in the small RLS subgroup to 20.00% in the mild RLS subgroup and 41.67% in the large RLS subgroup (= 0.033) (Figure 4B).
Finally, the DWI lesions of CS patients with an equivalent grade of RLS between the permanent RLS group and the latent RLS group were compared. A statistically significant difference was found only in the proportions of posterior circulation lesions of the large RLS subgroup for the permanent RLS group (8.11%) and the latent RLS group (41.67%;= 0.007). No statistically significant difference was found in mild or small RLS between the permanent RLS group and the latent RLS group.
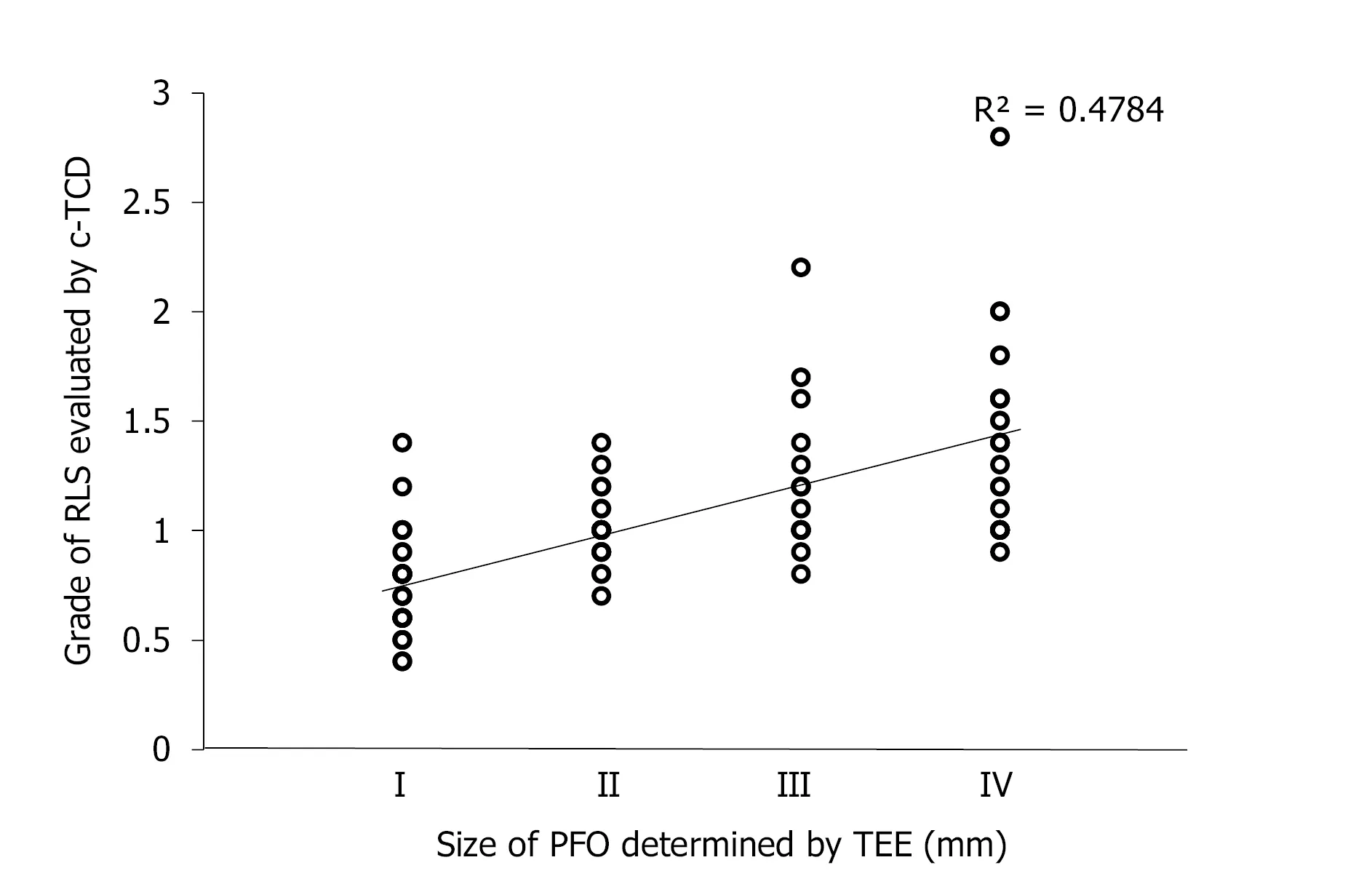
Size of PFO as determined by TEE
The width of fissure between the primary septum and secondary septum was measured as the size of PFO in all PFO-related CS patients. The grade of RLS evaluated by c-TCD was found to correlate statistically with the size of PFO determined by TEE (= 0.758,< 0.001) (Figure 5).
DISCUSSION
Baseline characteristics and laboratory tests
Data were statistically analyzed using SPSS statistical software, version 25.0 (IBM Corp., Armonk, NY, United States). For continuous variables, one-way analysis of variance or the Kruskal-Wallis test were used to compare between-group differences. The least significant difference test or the adjusted Mann-Whitneyrank sum test were chosen as the method for intragroup multiple comparisons. For nominal variables, intragroup and intergroup differences were analyzed using the Pearsontest,test for trends, Fisher’s exact test or partitioningtest. Spearman rank correlation was used to analyze the correlation between the grade of RLS evaluated by c-TCD and the size of PFO determined by TEE. The level of significance was set at< 0.05.
One of the main determinants of success in life is our attitude towards adversity. From time to time we all face hardships, problems, accidents, afflictions and difficulties. Some are of our making but many confront us through no fault of our own. Whilst we cannot choose the adversity we can choose our attitude towards it.
Infarction pattern
In the present study, we demonstrated characteristic infarction patterns on DWI depending on the different types and grades of RLS in PFO-related CS patients. Patients with permanent RLS were more likely to involve multiple territories, and patients with latent RLS were more likely to involve posterior circulation. We also observed this tendency in latent-large RLS patients. The high prevalence of posterior circulatory infarction in latent RLS patients can be attributed to the reduced innervation of the sympathetic nervous system and the increased blood flow to the posterior circulatory area after the provocation maneuver[22,23]. Meanwhile, infarction in permanent RLS patients exhibited the tendency to involve multiple vascular territories because of the existence of microemboli, both at a resting state and after the provocation maneuver[13].
We also found that the DWI lesions exhibited certain characteristics as the grade of shunt increased, for both the permanent RLS group and the latent RLS group. These lesions were more likely to be multiple, small and cortical lesions. This infarction pattern was consistent with the main characteristic of PFO-related stroke reported in previous studies[24,25]. PFO is an imbricate structure and a potential fissure, which usually only allows for passage of smaller microemboli[26]. If the grade of RLS increases, the number of microemboli that can pass through the PFO will increase relative to the blood flow to the peripheral vessels of the brain. This provides an anatomical basis for multiple, small and cortical lesion patterns.
Size of PFO as determined by TEE
In accordance with the five-level categorization system based on the number of MBs[6], we conducted semiquantitative grading by c-TCD. Although the semiquantitative grading could not diagnose the presence of PFO in our study, we discovered that once PFO was confirmed by TEE, the grade of RLS evaluated by c-TCD was related to the size of PFO as determined by TEE. However, the specific relationship was not very clear and may be explained by several reasons. One is that the number of MBs appearing in the left atrium detected by contrast TEE is not uniformly evaluated in the literature. Thus, the grade of RLS could not be compared with the size of PFO in the same inspection. Another reason is that the size of PFO measured by TEE could be larger than the real value because of the increased pressure in the right atrium[27]. Moreover, a previous study demonstrated that the size of PFO increases with age[28].
TEE is currently regarded as the gold standard for diagnosis of PFO. However, TEE is a semi-invasive detection method, and some patients refuse the procedure due to intolerance. Also, because PFO represents a potential fissure, TEE may miss small PFOs, suggesting that use of TEE may not provide the highest sensitivity for RLS detection[30]. At present, c-TCD is the most commonly used method for detecting RLS clinically, including intracardiac and extracardiac RLS[14]. According to the time when microbubbles appear and whether the signal changed after VM, we could identify intracardiac and extracardiac RLS[31]. The sensitivity and specificity of c-TCD for diagnosis of PFO were reported to be 96.1% and 92.4% respectively[32]. In our study, patients were trained to blow into the connecting tube of a VM quantitative device so that the pressure gauge reached 40 mmHg. Previous studies have reported that the use of quantitative VM significantly improved the positive rate of c-TCD detection of RLS[15]. Indeed, as a noninvasive, effective and repeatable technique, c-TCD has been used to screen PFO through recognition of RLS.
In the current study, 38% of the PFO-CS patients had latent RLS. We found that several patients with latent RLS (detected by c-TCD) were initially negative on TEE. Once we increased the intrathoracic pressure in these patients by appropriately pressurizing their abdomen, the RLS fascicles at the atrial level were observed. This problem could be attributed to difficulty in performing the VM effectively during TEE probe intubation or after sedation; consequently, an inadequate pressure gradient occurs between the right and left atria[29]. This may have led to underestimation or even misdiagnosis of latent RLS induced by PFO on TEE.
She had called her mother that morning to wish her a happy Mother s Day, and her mother had mentioned how colorful the yard was now that spring had arrived. As they talked, the younger woman could almost smell the tantalizing2() aroma3 of purple lilacs() hanging on the big bush outside her parents back door.
Thought I d find you here, first weekend in September. Do you want these? He held out a handful of berries, then tipped them into her bag. Perfect day - are there any bilberries?
There are two major strengths of this study. The first is the application of quantitative VM in c-TCD ensured effectiveness of the detection. The second is the analysis of DWI lesions of PFO-related CS patients by combining different types and grades of RLS detected by c-TCD and the comparison of the multiple features of the infarct. However, our study also included several limitations. First, the study was retrospective and conducted in a single center; Second, to ensure the integrity of data, all cases selected were inpatients, hence presenting a potential for selection bias; and third, the sample size of this study was not adequately large. Therefore, expanding the sample size and sample selection range as well as conducting in-depth and comprehensive studies are necessary to fully elucidate the mechanism of stroke in PFOrelated CS patients.
CONCLUSION
Before the test, an 18-gauge needle was aseptically inserted into the left median cubital vein of the patient. The contrast agent was prepared in a saline bag using a mixture of 9 mL of saline, 1 mL of sterile air, and a single drop of blood from the patient. Microbubbles were then created by rapid mechanical mixing (20 times) by means of two 10 mL syringes connected by a three-way stopcock. Immediately after, the contrast agent was injected into the prepared median cubital vein as a bolus. The procedure was performed during: (1) resting state; (2) conventional VM, for which the patients had been trained prior to inhale deeply and hold their breath; and (3) quantitative VM, for which the patients had been trained prior to inhale deeply and blow into the connecting tube of a VM quantitative device. A middle cerebral artery flow velocity with a 25% decrease was used to indicate that the conventional VM was effective[15]. For the quantitative VM specifically, the participants had been trained to blow into the connecting tube so that the pressure gauge reached 40 mmHg[16]. The conventional VM and quantitative VM were monitored over a period of 10 s, starting 5 s after the time the contrast agent injection had been initiated. Each maneuver had an interval of at least 2 min from the last observed microbubble signal (MBs) to ensure that the microbubbles were completely metabolized. The MBs was detected as a series of high-intensity transient signal, defined by the typical chirping sound within the doppler flow spectrum. The spike-like appearance on the spectrogram produced by reprocessing analysis was distinguishable from the noise.
ARTICLE HIGHLIGHTS
Research perspectives
She didn t know if Eric felt the same until they left work together one evening and took a stroll out on a pier above the Pacific Ocean. He signed to her that he was in love and wanted to marry. Marianne s heart danced with joy.
Research conclusions
In this study, we propose that multiple territory infarctions may indicate permanent right-to-left shunt (RLS), while posterior circulation infarction may indicate latent RLS,which suggests that the distribution of infarct may provide clues for contrast-enhanced transcranial Doppler (c-TCD) screening for PFO. This study proposed a new method of analyzing the characteristics of infarction lesions by combining the type and grade of RLS detected on c-TCD.
Research results
The distribution of infarcts indicated a trend for the type of RLS. This observation could contribute to c-TCD screening for PFO. However, this study did have a potential selection bias, and the sample size was not large enough.
Share $20.00 worth of time with someone you love...just a short reminder4 to all of us working so hard for our living. However, let us not let time slip through our fingers without having spent some quality time with those who really matter to us.
Research methods
This was a retrospective study. The normal group (non-CS patients) was selected for control study, and the CS patient group was divided into specific groups for intragroup and intergroup analyses. Patients in the CS patient group received both c-TCD and transesophageal echocardiography, which allowed us to observe patterns in the infarct lesions.
Knowing the death could have been avoided if he had only realized the seriousness of the situation, he always felt he was guilty. To make matters worse, his wife left him a short time later, leaving him alone with his six-year-old younger son. The hurt and pain of the two situations were more than Al could stand, and he turned to alcohol4 for help. In time Al became an alcoholic5.
Research objectives
To find the association between the characteristics of infarction lesions and the type and grade of RLS in PFO-related CS patients. This information will provide a basis for future mechanism research of stroke in PFO-related CS patients.
Research motivation
We aimed to find an association between the characteristics of infarction lesions and the type and grade of RLS in PFO-related CS patients. We hypothesized that we could predict the type and grade of shunt detected during c-TCD examination by the characteristics of the infarction lesions, which would guide the effectiveness of c-TCD.
2. The youngest of whom was called Dummling: Sometimes the translations of the tale call the youngest son Simpleton . Bruno Bettelheim sees the number three as representing the ego14, super-ego, and id (102). Bettelheim sees the simpleton character as the fairy tale s rendering15 of the original debilitated16 state of the ego as it begins its struggle to cope with inner world of drives and with the difficult problems which the outer world presents (75).Return to place in story.
Research background
CS is relatively common in young people. RLS caused by PFO is an important risk factor for CS. Determining the characteristics of infarction lesions in PFO-related CS patients and the type and grade of RLS is of great value in the search for the etiology of CS.
ACKNOWLEDGEMENTS
The authors would like to extend their gratitude to the patients who consented to the use of their clinical and image data.
World Journal of Clinical Cases2022年1期
- World Journal of Clinical Cases的其它文章
- Hepatitis B virus reactivation in rheumatoid arthritis
- Paradoxical role of interleukin-33/suppressor of tumorigenicity 2 in colorectal carcinogenesis: Progress and therapeutic potential
- Changes in rheumatoid arthritis under ultrasound before and after sinomenine injection
- Benefits of multidisciplinary collaborative care team-based nursing services in treating pressure injury wounds in cerebral infarction patients
- Outcomes and complications of open, laparoscopic, and hybrid giant ventral hernia repair
- Surgical resection of intradural extramedullary tumors in the atlantoaxial spine via a posterior approach