
Increased levels of lactate dehydrogenase and hypertension are associated with severe illness of COVID-19
2022-02-11 05:28ZhenMuJinJiChanShiMoZhengQueLuChenYueYingZhouFangChengJingCaiXianGaoJiang
World Journal of Clinical Cases 2022年1期
INTRODUCTION
Coronavirus disease 2019 (COVID-19) has rapidly evolved into a pandemic since its first outbreak in Wuhan, China in December 2019. However, there is still no effective drugs for this disease[1,2]. In addition, the symptoms and signs and pathological mechanisms of COVID-19 are very complex, posing great challenges in treating patients. Our hospital is a dedicated hospital for treating patients with COVID-19 in Wenzhou, China, which is 680 km from Wuhan. There is strong economic connectivity and mass migrations between the two cities. The present study aimed to analyze the clinical characteristics of COVID-19 patients from a hospital in Wenzhou, China.
MATERIALS AND METHODS
Patients
The clinical data of COVID-19 patients treated from January 22, 2020 to March 3, 2020 at our hospital were retrospectively collected. The diagnostic criteria for COVID-19 at our hospital were: (1) Potential exposure to COVID-19; (2) Had fever, respiratory symptoms, radiological abnormalities in the lungs, or leukocytopenia/lymphocytopenia; and (3) Presence of viral RNA in nasopharyngeal specimens. The inclusion criteria were: (1) With laboratory-confirmed COVID-19; (2) With specific outcomes of discharge or death; and (3) Had been examined by chest computed tomography (CT) during hospitalization. Our study was approved by the ethics committee of our hospital.
But the young man told her all his sad tale, and how he possessed5 a wonderful snuff-box, and how it had been stolen from him, and how he had nothing left, now that he was parted from his wife and was in need of everything
Data collection
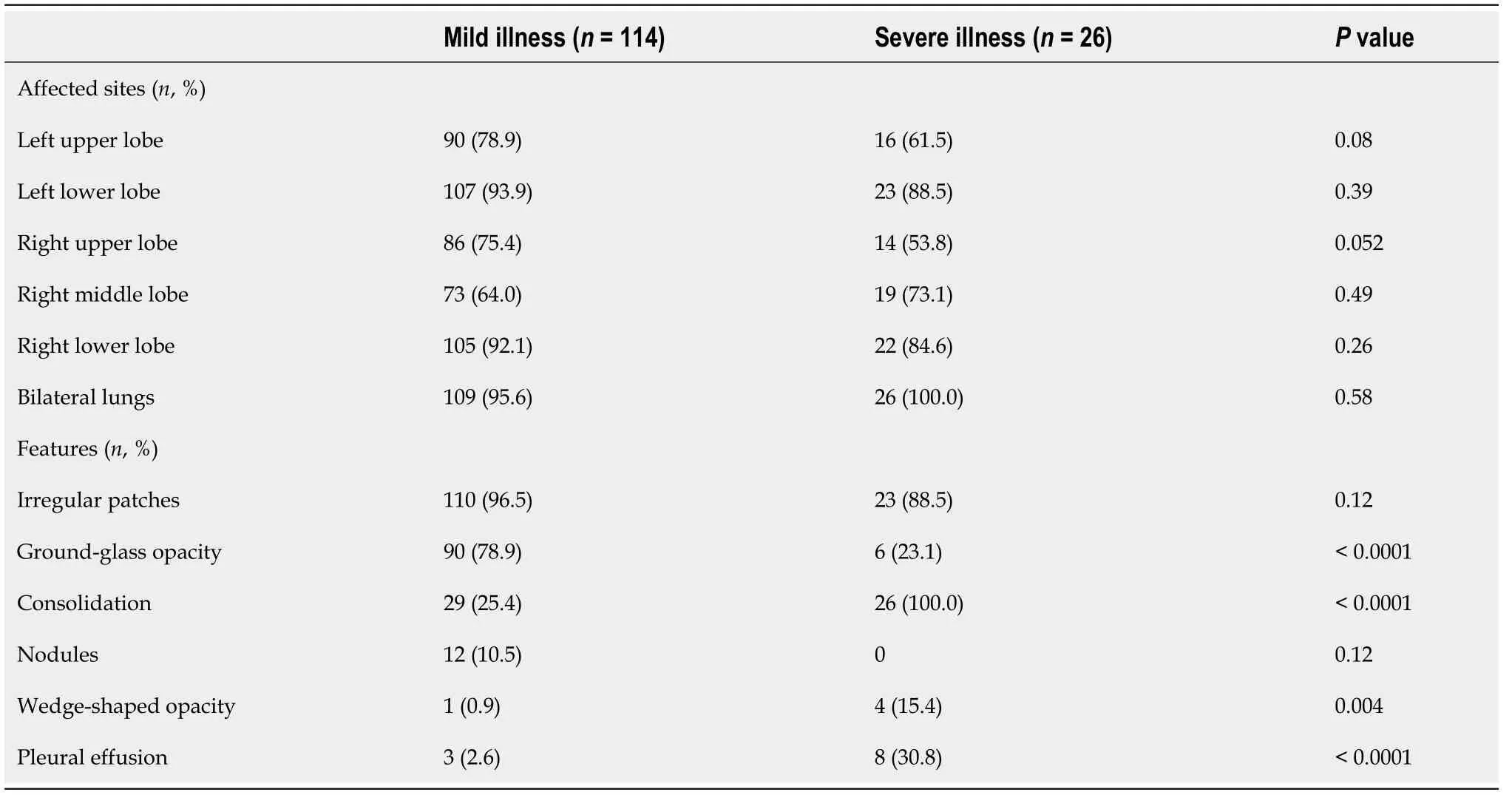
Only 3 three patients showed no significant radiologic findings (3/140, 2.1%). The radiologic characteristics are shown in Table 3. There was no significant difference in the frequency of affected lung sites between patients with mild illness and those with severe illness. However, significantly more patients with mild illness had ground-glass opacity than those with severe illness (78.9%23.1%,< 0.0001). On the contrary, there were significantly more patients with consolidation (100%25.4,< 0.0001) and pleural effusion (30.8%2.6%,< 0.0001) in the severe illness group than in the mild illness group.
The existence of comorbidities can increase the risk of more severe illness and mortality in COVID-19 patients[7,8]. The most common comorbidity in our patients was hypertension (22.9%), and patients with severe illness were significantly more likely to be hypertensive than those with mild illness (38.4%19.3%). A previous study with 1099 COVID-19 patients also found that hypertension was associated with severe disease[3]. In addition, we found that the levels of lactate dehydrogenase were significantly elevated in patients with severe illness compared to those with mild illness. Lactate dehydrogenase is a biomarker for myocardial injury[9,10]. All these findings suggest that hypertension and the resulting myocardial injury may lead to a poor prognosis in COVID-19. There have been concerns and debates on the roles of the renin-angiotensin system, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers in COVID-19 and poor prognosis[11-15]. However, there is no con
Statistical analysis
Older people are at increased risk of cardiovascular diseases and COVID-19. The relationship between COVID-19 and cardiovascular diseases is poorly understood.
RESULTS
Patient general information
A total of 140 laboratory-confirmed COVID-19 patients were included in our study (Table 1). There were 75 male patients and 65 female patients (53.6%46.4%). The mean age was 45.4 ± 14.6 years (range, 2-85 years). Most of the patients had potential exposure to COVID-19 (= 92, 65.7%).
Clinical characteristics
The most common symptom was fever (= 110, 78.6%), followed by cough (= 82, 58.6%), expectoration (= 51, 36.4%), fatigue (= 20, 14.3%), shortness of breath (= 15, 10.7%), diarrhea (= 14, 10%), and headache (= 4.3%) (Table 1). Eight patients (5.6%) were asymptomatic but were positive for SARS-CoV-2 RNA. These patients were family members or neighbors of other symptomatic patients and thus were tested for COVID-19.
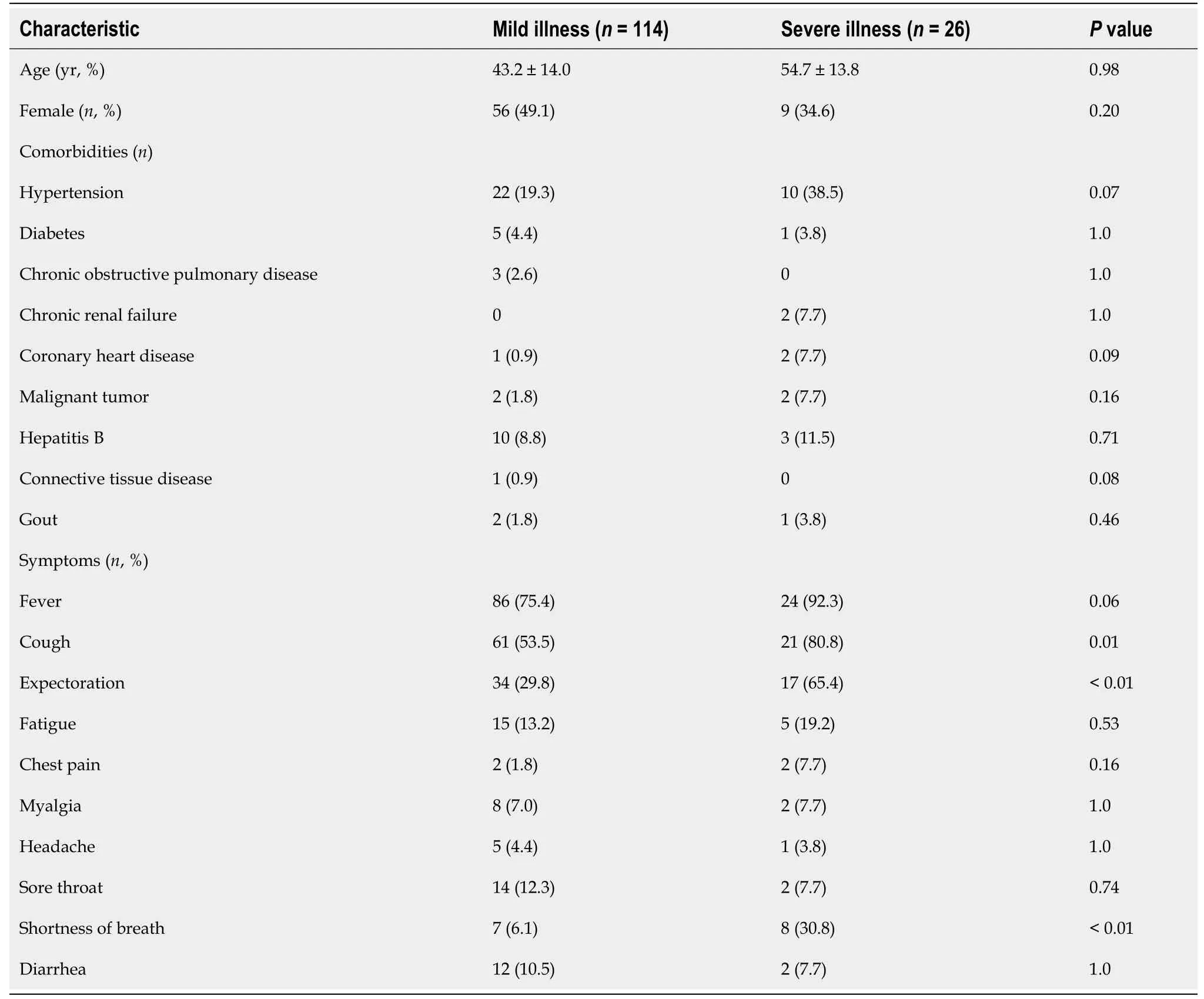
The most common comorbidity was hypertension (= 32, 22.9%). Other comorbidities included diabetes (= 6), coronary heart disease (= 3), and malignant tumor (= 4). Most of the patients had mild illness (= 114, 81.4%) and 26 had severe illness (18.6%) (Table 1). Patients with severe illness were significantly more likely to be hypertensive than those with mild illness [(10/26, 38.5%)(22/114, 19.3%),= 0.036].
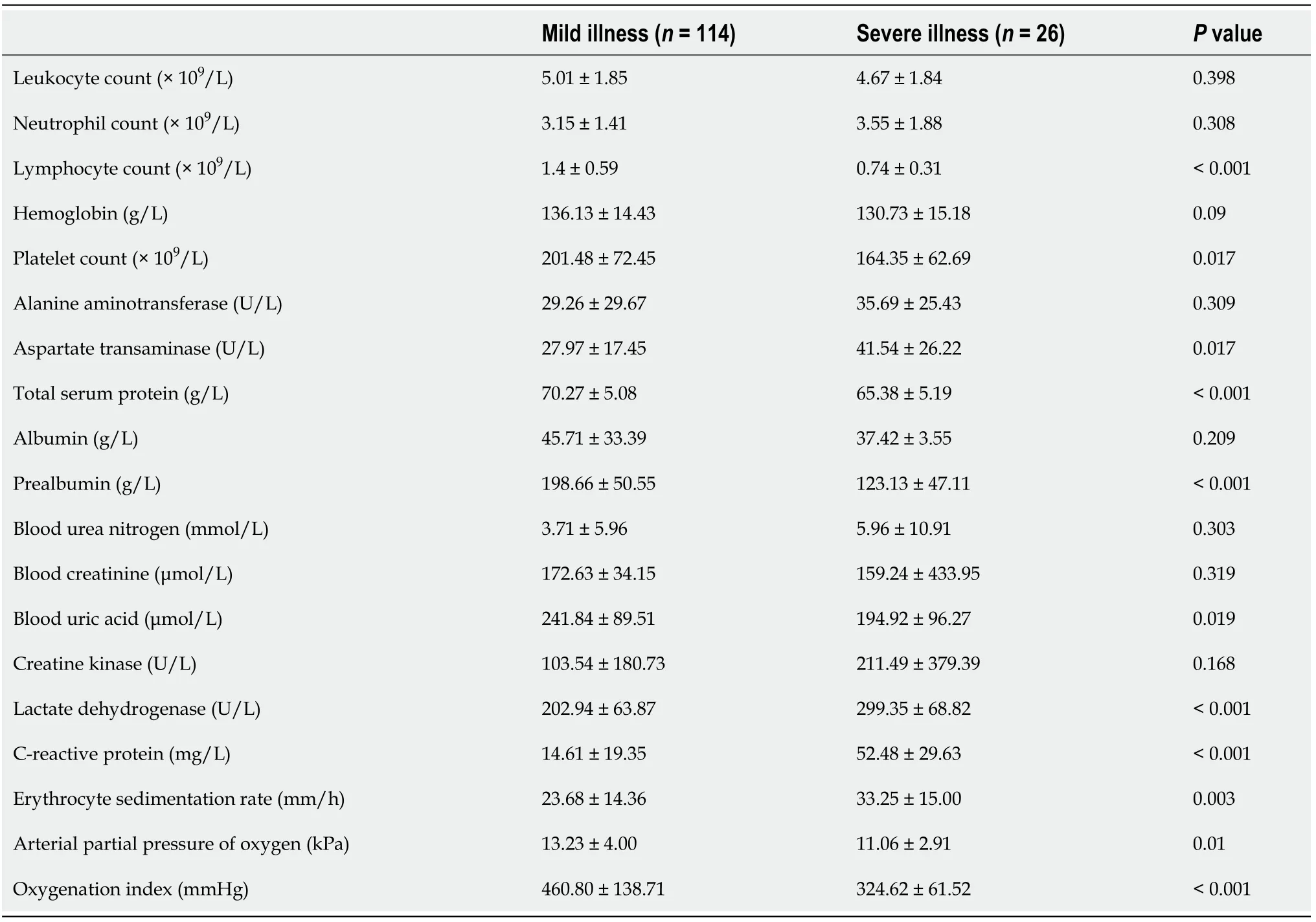
The results of laboratory tests are shown in Table 2. The leukocyte count was lower than 3.5 × 10/L in 26 patients (18.6%). The lymphocyte count was lower than 1.1 × 10/L in 54 patients (38.6%). Low levels of hemoglobin were present in 16 patients (11.4%). Thrombocytopenia (< 100 × 10/L) was present in three patients. Elevated serum levels of creatinine > 94 μmol/L were noticed in 18 patients. Elevated serum levels of creatine kinase > 200 U/L were noticed in 12 patients, and > 500 U/L in three patients. Elevated serum levels of lactate dehydrogenase were noticed in 37 patients. The level of lactate dehydrogenase was significantly higher in the severe illness group than in the mild illness group (299.35 ± 68.82202.94 ± 63.87,< 0.001). There were significant differences in lymphocyte count, platelet count, levels of total serum protein, prealbumin, blood uric acid, lactate dehydrogenase, C-reactive protein, erythrocyte sedimentation rate, arterial partial pressure of oxygen, and oxygenation index between patients with mild illness and those with severe illness (Table 2).
Radiologic characteristics in computed tomography
All data were retrospectively collected from electronic records of the patients, including sex, age, symptoms, radiological findings, laboratory test results, treatment methods, and patient outcomes. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA was tested using quantitative real-time polymerase chain reaction. Blood samples were collected at 7 am after fasting overnight. Disease severity was classified as mild illness (respiratory symptoms and/or radiological findings of pneumonia) and severe illness (respiratory distress and/or need of mechanical ventilation).
Treatment outcomes
High-flow nasal oxygen therapy was used in 22 patients with mild illness (22/114, 19.3%), while all the 26 patients with severe illness used this treatment. Non-invasive mechanical ventilation was used in 4/26 (15.4%) patients with severe illness, while none of the patients with mild illness used this treatment. No tracheal intubation was required in our patients. All patients were cured and discharged as of March 3, 2020.
Fever (78.6%) and cough (58.6%) were the most common symptoms in our patients. This finding is consistent with previous reports[3,4]. However, these symptoms are not specific and many of the patients had early on-set symptoms of fatigue, diarrhea, and myalgia. In addition, eight patients (5.6%) were asymptomatic but were positive for SARS-CoV-2 RNA. Most recent research showed that the rate of asymptomatic infection in the general population may be as high as 80.9%[5,6]. Due to the criteria for diagnosis and patient admission for COVID-19 at our hospital, asymptomatic patients were not tested for viral RNA and thus were not confirmed with the diagnosis of COVID-19.
DISCUSSION
Our study retrospectively analyzed 140 patients with laboratory-confirmed COVID-19 and found that patients with severe illness were more likely to have hypertension than those with mild illness. In addition, the level of lactate dehydrogenase was significantly higher in the severe illness group than in the mild illness group.
Every day when she got up she meant to say it at night, and when night came she put it off again, until at last she had a dismal dream which helped her to make up her mind
In short, Bingo turned exceptionally nasty. When he saw our heads pop up in the window frame, instead of the reassuring features of his owners, he had an expression of bewilderment(,) . His eyes, if ever a dog could do this - became wide with shock and incomprehension, which, as he was approached, festered() into vicious disappointment, bile and acrid() resentment.
crete evidence at present suggesting that these anti-hypertensive drugs should be discontinued in hypertensive COVID-19 patients[16,17].
All our patients were examined by CT and only three showed no significant radiologic findings in the lungs. Most patients had signs of involvement of bilateral lungs, especially the lower lobes. Patients with severe illness of COVID-19 had features of involvement of multiple lobes, irregular patches, and consolidations. Significant radiological progression was seen in 32 patients (22.9%) even after 3 to 7 d. Consistent with previous studies[18,19], our findings suggest that COVID-19 patients with mild or no symptoms may be negative in chest CT examinations. Although CT should not be relied on as a method for screening or diagnosing COVID-19, we recommend repeated chest CT for suspected patients in case of symptoms onset or disease progression.
Our study found that most of the laboratory-confirmed COVID-19 patients in Wenzhou, China had mild illness and generally good outcomes. Hypertension and elevated levels of lactate dehydrogenase may be associated with severe illness of COVID-19. Targeting hypertension-associated myocardial injury may be a potential option in the treatment of COVID-19.
CONCLUSION
Our study has limitations. First, most of our patients were only diagnosed with COVID-19 and admitted to the hospital when they showed symptoms. This criterion for diagnosis may underestimate the true population of COVID-19 patients. Second, patients with mild symptoms may not visit the clinics and just stay at home. This may potentially increase the proportion of patients with severe illness in our study. Third, the relationship between hypertension and elevated levels of lactate dehydrogenase in COVID-19 patients was not addressed due to the retrospective nature of our study.
ARTICLE HIGHLIGHTS
Research background
The coronavirus disease 2019 (COVID-19) pandemic is still evolving.
Research motivation
Continuous data are presented as the mean and standard deviation and were compared using the independent student’s-test. Categorical data are presented as counts or percentages and were compared using the Chi-square test. All statistical analyses were performed using SPSS 24.0 (IBM, United States). Avalue less than 0.05 was considered statistical significance.
Research objectives
Our study aimed to find out the relationship between COVID-19 and cardiovascular diseases.
Research methods
The clinical data of 140 COVID-19 patients were retrospectively analyzed. The clinical characteristics were compared between patients with mild illness and those with severe illness.
Research results
Patients with severe illness of COVID-19 were more likely to be hypertensive and had significantly higher levels of lactate dehydrogenase than those with mild illness.
Clark stayed. For the season and time, the Virginia night was warm. Most leaves had been blown away already, and the trees stood unbothered. The moon was round above them.
Research conclusions
The coexistence of hypertension and higher levels of lactate dehydrogenase in patients with severe illness of COVID-19 suggests a close relationship between COVID-19 and cardiovascular diseases.
Now when the boy had come to his full strength the King of that country fell in love with his mother, and wanted to marry her, but he knew that she would never part from her boy
When the young man saw the maiden12 weeping bitterly he said to her, What is the matter, my poor girl? Oh! she answered, I am chained here till a horrible serpent with seven heads comes to eat me
Research perspectives
The relationship between hypertension and elevated levels of lactate dehydrogenase in COVID-19 patients should be addressed in future investigations.
World Journal of Clinical Cases2022年1期
- World Journal of Clinical Cases的其它文章
- Hepatitis B virus reactivation in rheumatoid arthritis
- Paradoxical role of interleukin-33/suppressor of tumorigenicity 2 in colorectal carcinogenesis: Progress and therapeutic potential
- Changes in rheumatoid arthritis under ultrasound before and after sinomenine injection
- Benefits of multidisciplinary collaborative care team-based nursing services in treating pressure injury wounds in cerebral infarction patients
- Outcomes and complications of open, laparoscopic, and hybrid giant ventral hernia repair
- Surgical resection of intradural extramedullary tumors in the atlantoaxial spine via a posterior approach