
Symptom trajectories in patients with breast cancer: An integrative review
2022-02-08 03:24TingtingCiYueshiHungQingmeiHungHozhiXiChngrongYun
Tingting Ci , Yueshi Hung , Qingmei Hung , Hozhi Xi ,b, Chngrong Yun ,*
a School of Nursing, Fudan University, Shanghai, China
b School of Nursing, Nanjing University of Chinese Medicine, Nanjing, China
Keywords:Breast neoplasms Nursing care Patients Signs and symptoms Trajectories
ABSTRACT Objective: This study aimed to synthesize the available knowledge of symptom trajectories in patients with breast cancer and identify predictors associated with these trajectories.Methods: Whittemore and Knafl’s integrative review method was employed to guide a systematic search for literature in four databases (PubMed, Embase, Web of Science, and CINAHL).The retrieved articles’publication time was limited to 2010 to 2020, and only peer-reviewed English articles were included.Results: Twenty-seven articles were included.The findings of the relevant studies were analyzed using thematic analysis.They were grouped into two themes: symptom trajectories of patients with breast cancer (symptom trajectories in patients with breast cancer, in patients who underwent surgery, and in patients who received cancer-related treatment) and associated factors (socioeconomic factors, health characteristics,cancer-related treatment characteristics).Newly diagnosed patients tended to report high trajectories of depression and persistent sleep disturbance.Most patients who underwent surgery reported significant sleep disturbance and anxiety shortly after surgery.For patients who received cancerrelated treatment, only a small proportion had a high level of physical activity after cancer-related therapy over time.A high body mass index, a low relationship quality, parental responsibilities, insufficient social support, a low educational background, and an unhealthy lifestyle may increase the risk of negative symptom trajectories in patients with breast cancer.Additionally,old patients were more likely to report cognitive impairment after chemotherapy,while young patients tended to report trajectories of persistent sexual dysfunction.Concurring symptoms and poor health status also contributed to adverse symptom trajectories.Conclusion: The findings of this review add to the body of knowledge of the interindividual variability of symptom trajectories in patients with breast cancer.Despite the overall similarity in appraisal at baseline, the patients reported varied symptom trajectories over time.It is recommended that nurses consider sociodemographic, clinical and cancer-related treatment characteristics and perform targeted early preventive interventions for patients with breast cancer.
What is known?
· Cancer-related symptoms are dynamic and change over time,affecting patients at diagnosis and during treatment and can be persistent or increase during cancer progression.
· It is vital for nurses to identify the interrelatedness and change in symptoms to guide timely care.
What is new?
· This review provides insights into the interindividual variability of symptom trajectories in patients with breast cancer.
· The findings demonstrate the need to consider sociodemographic, clinical and cancer-related treatment characteristics and perform targeted early preventive interventions for patients with breast cancer.
1.Introduction
Breast cancer is the most commonly diagnosed cancer in women worldwide[1].With extensive advances in early screening and cancer-related treatment options,the five-year survival rate for patients with breast cancer has increased significantly[2,3].Longterm survival with breast cancer and its subsequent treatment render symptom management increasingly important [4].
Breast cancer constellates multiple co-occurring symptoms caused by disease and treatment[5].Cancer-related symptoms are dynamic and change over time,affecting patients at diagnosis and during treatment and can be persistent or increase in the cancer continuum.Additionally, these symptoms may decrease function and become significant contributors to interrupted medical treatment[5].Symptom trajectories are increasingly recognized as vital in symptom management [6].Nurses must identify the interrelatedness and change in symptoms to guide timely care[7-10].
Understanding the evidence regarding symptom trajectories in the context of breast cancer will allow nurses to identify patients with high-risk symptoms and develop proactive care strategies.A growing body of literature has reported symptom trajectories of patients with breast cancer, but reviews summarizing this important topic are scarce.Therefore, this study used the integrative literature review method to synthesize literature examining symptom trajectories and predictors in this population, aiming to identify systematic efforts to initiate timely and precise screenings for symptom-specific interventions.
2.Methods
A literature review was performed using Whittemore and Knafl’s methodology for integrative reviews [11].The methodological approach comprised five sequential stages: 1) problem identification,2)systematic literature search,3)data evaluation,4)data analysis, and 5) presentation of findings.
2.1.Problem identification
The review was guided by two questions: 1) What symptom trajectories have been reported in patients with breast cancer?2)What factors are associated with increased symptom trajectories?
2.2.Literature search
A comprehensive search of four relevant databases (PubMed,Embase, Web of Science, and CINAHL) was conducted in December 2020.The inclusion criteria of the studies were as follows:1)original qualitative and quantitative literature published between January 2010 and December 2020; 2) international literature published in English from peer-reviewed journals; and 3) literature that focused exclusively on symptom trajectories of patients with breast cancer.Studies were excluded if they did not explicitly report subjects of interest,analyzed mixed cancer types,were of insufficient quality,or were reviews, editorials, or comments.The central terms for combined searches included “breast cancer*” OR “breast tumor*” OR“neoplasm of the breast*” OR “breast neoplasm*” AND “symptom trajectory*” OR “symptom trend*” OR “symptom pattern*” OR“symptom evolution*”OR“symptom change*”AND“predictor*”OR“risk factor*” OR “risk*” OR “associated factor*”.The initial search revealed 841 articles and excluded 435 duplicates.In total, 254 articles were excluded based on their titles and abstracts.Further screening excluded those that analyzed mixed cancer types(n=108)and those whose full-text articles were unavailable(n=17).Twentyseven representative studies that met the inclusion criteria were included in the analysis (Fig.1 ).No articles were excluded after quality appraisal.
2.3.Data evaluation
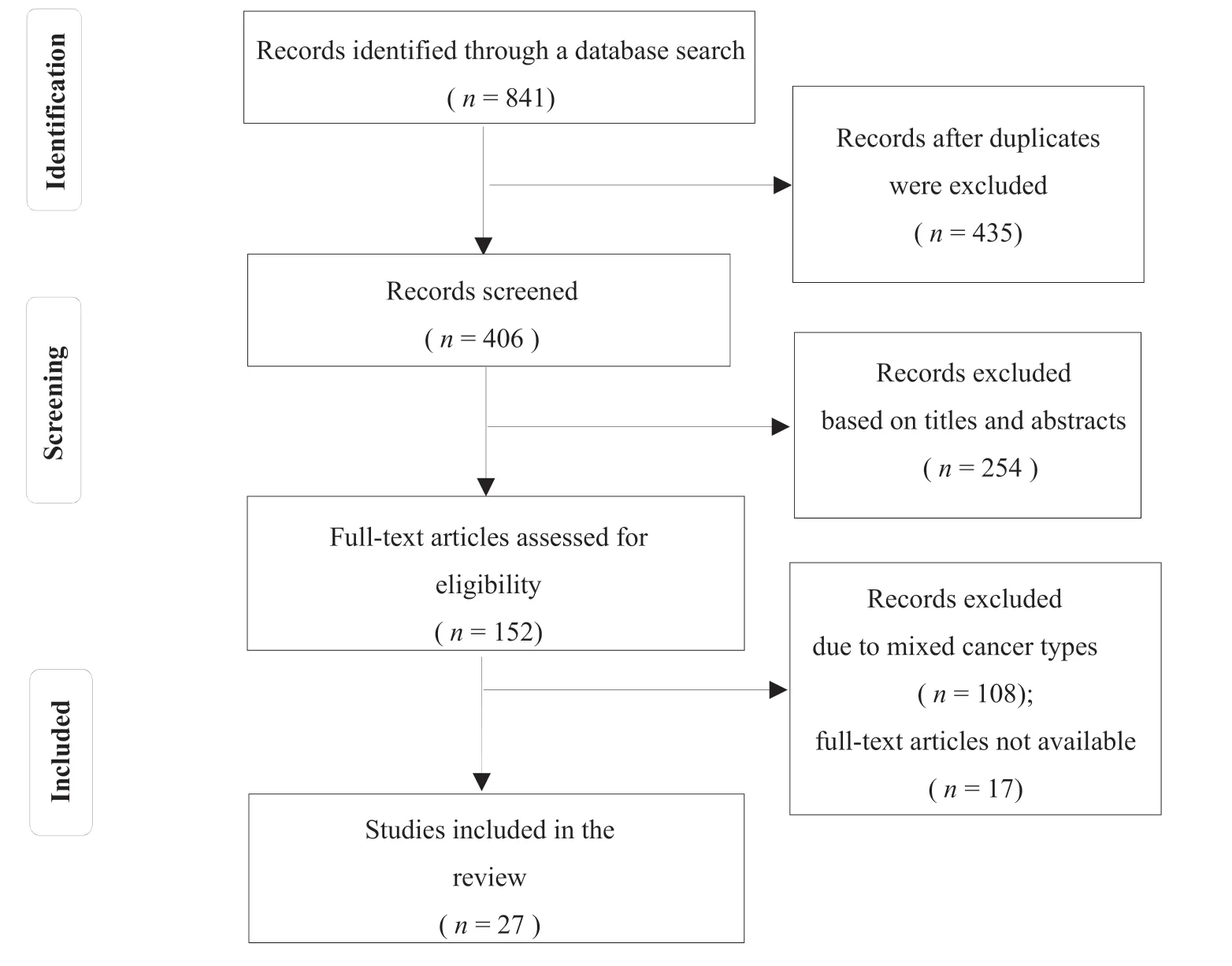
Fig.1. Flow diagram of the study selection.
A review rubric for critical appraisal of the literature was adopted to assess the methodological rigor [12].The Mixed Methods Appraisal Tool (MMAT) 2011 was employed to evaluate the methodological quality of the articles.The total number of assessment criteria assigned the number of criteria met by papers to calculate the MMAT 2011 score.Five categories were included,and papers with a 75% or higher quality indicated high and very high quality [12].Two researchers assessed the articles independently, discussing the quality score using the MMAT.Any discrepancies in the scores were discussed until a consensus was reached.
2.4.Data analysis
Thematic analysis was chosen for an integrative review considering the heterogeneity of the studies [11].Data reduction,display, comparison, conclusion drawing, and verification were performed.The findings were structured into subsections by research and location, the aim of the study, design, methods,sample, key findings, and quality score in a data matrix template.Data were extracted and coded according to the research questions addressed in this review into a manageable framework for all included studies to integrate the results.Subsequently, the data were assembled around corresponding subgroups based on the research topic.Similar data were compared and grouped until the final themes were refined.
3.Results
3.1.Study characteristics
The included studies were from the United States(n=20),Korea(n= 1), Switzerland (n= 1), Germany (n= 1), Canada (n= 1),Denmark (n= 1), Portugal (n= 1), and Singapore (n= 1).Categorization of the key findings permitted the identification of two general themes: physical symptom trajectories and psychological symptom trajectories.The studies focused mainly on physical function, sexual function, pain, fatigue, and sleep disturbance regarding physical symptom trajectories.The targeted symptoms were depression, anxiety, cognitive function, fear of cancer recurrence, and psychological distress regarding the psychological symptom trajectories.The data collection methods used in the included studies were mainly questionnaires, interviews, and laboratory examinations.(Table 1)

Table 1Summary table of evidence for the included studies (n = 27).
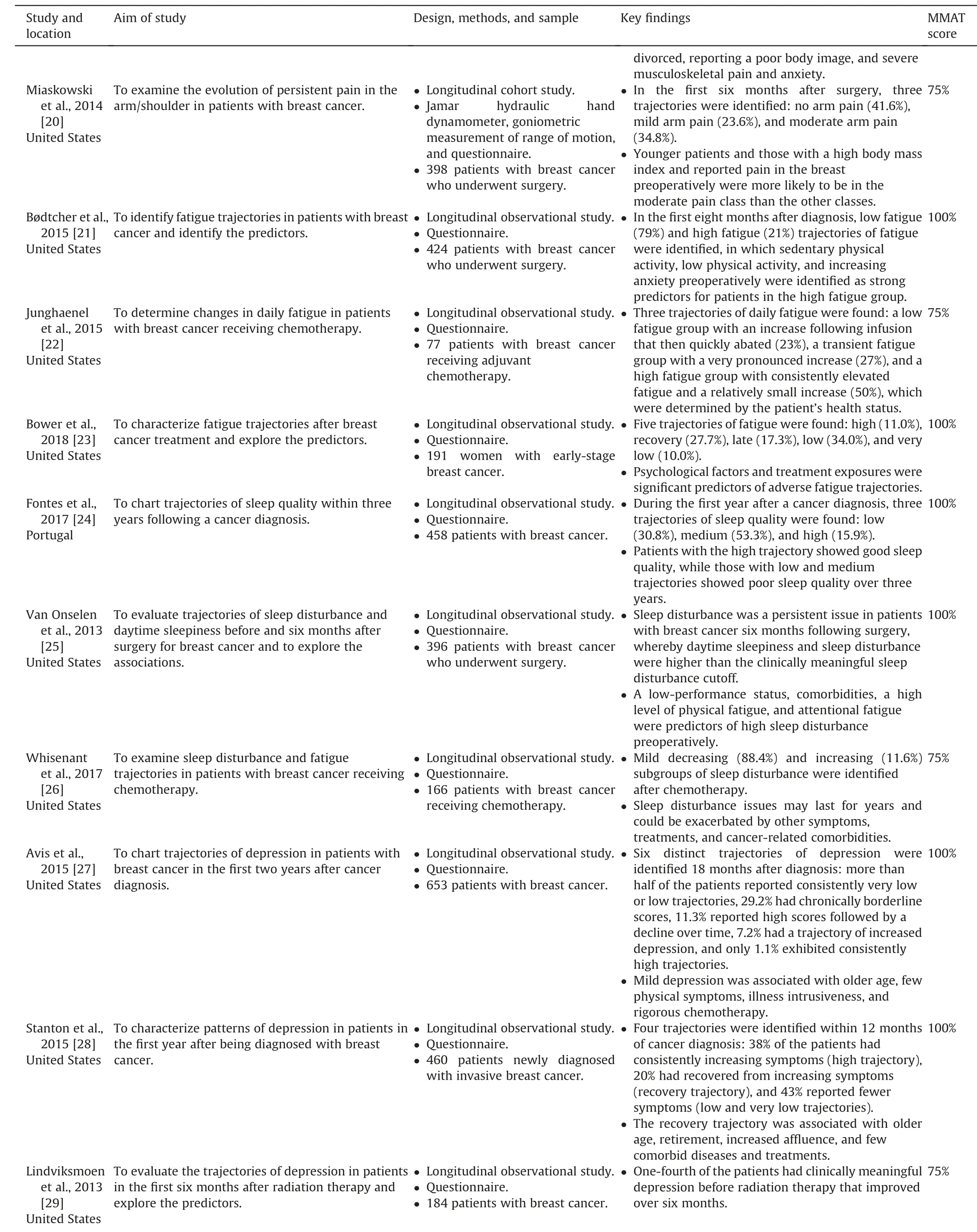
Table 1 (continued)
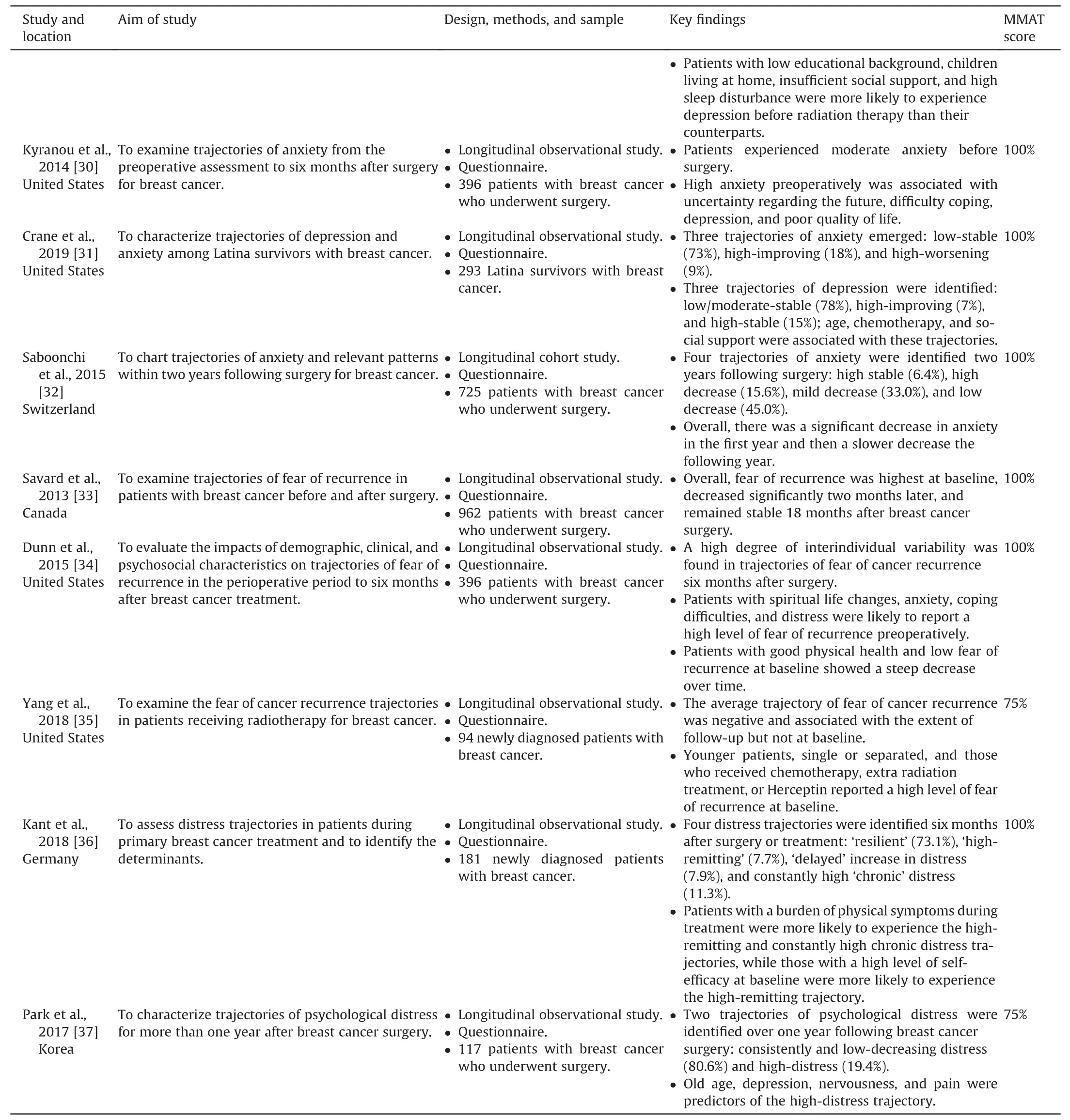
Table 1 (continued)
3.2.Identified themes
The studies were grouped into ‘symptom trajectories of breast cancer’and‘associated factors.’The subthemes identified from the‘symptom trajectories in patients with breast cancer’ theme were symptom trajectories in patients with breast cancer, patients who underwent surgery for breast cancer, and patients who received cancer-related treatment.The subthemes identified from the‘associated factors’theme were socioeconomic,health,and cancerrelated treatment characteristics.
3.2.1.Symptom trajectories in patients with breast cancer
Nine studies focused on symptom trajectories in patients with breast cancer.Trajectories of depression[10,27,28,31],anxiety[31],cognitive function [16], sexual function [19], fatigue [23], sleep disturbance [24], and psychological distress [36]were identified.
Four studies described trajectories of depression [10,27,28,31],one of which also examined trajectories of anxiety [31].The targeted population included patients from diagnosis to survivorship[10], newly diagnosed patients with breast cancer [27,28], and Latina women with breast cancer [31].A large proportion of patients with breast cancer were grouped into low trajectories of depression [10,27,28,31].Rottmann et al.[10]identified three trajectories of depression in couples with breast cancer,half of whom reported a low trajectory, accounting for the most significant proportion of the sample.Similar trajectories were found for partners, with 67% of the samples grouped into a low depression trajectory.The results were supported by Avis et al.[27], who reported that over half of the patients reported consistently very low or low trajectories, and 29.2% reported chronically borderline scores.A small percentage of the sample reported a high trajectory of depression, although the pattern varied [27].Stanton et al.[28]reported that the majority of newly diagnosed patients with breast cancer had low depression symptoms, 43% of whom reported low symptom trajectories (low and deficient trajectories).However, a large proportion of patients had consistently increasing symptom trajectories (high trajectory, 38%), and this proportion was relatively larger than that of patients diagnosed a long time ago, as reported by Rottmann et al.[10](13%) and Avis et al.[27](8.3%).Based on the results,newly diagnosed patients were more likely to experience high trajectories of depression than those who were not newly diagnosed.Trajectories of depression in Latina women with breast cancer were in accordance with the conclusions of Rottmann et al.[10]and Avis et al.[27], who found low/moderate-stable(78%), high-improving (7%), and high-stable (15%) trajectories.Similarly, trajectories of anxiety in this population were identified as low-stability (73%), high-improvement (18%), and highworsening (9%) trajectories, which were partly consistent with the trajectories of depression [31].Overall, most patients with breast cancer did not report high trajectories of depression.
Five studies focused on symptom trajectories of vulnerable populations, including old patients [16]and young patients [19].For senior patients with nonmetastatic invasive breast cancer,Mandelblatt et al.[16]stated that trajectories of cognitive function were consistent with the aging theory.Most older patients with breast cancer maintained an excellent cognitive function status,while a small proportion reported an accelerated decline during chemotherapy [16].One study identified trajectories of sexual function in young patients (<40 years) in the first five years following a cancer diagnosis [19].Nearly 90% of the patients experienced persistent sexual disturbance, although most had stable and mild symptom trajectories.Patterns for psychological distress were better in newly diagnosed patients with breast cancer,most of whom reported a resilient trajectory(73.1%).Compared with sexual burden and distress trajectories,symptom disturbance(fatigue and sleep disturbance) was more prominent over time.Patients with high and recovery trajectories of fatigue accounted for the largest proportion of patients with early-stage breast cancer(40%) [23].Sleep disturbance was a severe symptom disturbance,especially in newly diagnosed patients [24].Fontes et al.[24]reported that nearly 80%of newly diagnosed patients had medium or high trajectories for sleep quality.During the three-year follow-up,a large proportion of patients reported persistently poor sleep quality before treatments and during follow-up.
3.2.2.Symptom trajectories in patients who underwent surgery
Seven studies focused on symptom trajectories in patients who underwent breast cancer surgery.Trajectories of pain [20], fatigue[21],sleep disturbance[25],anxiety[30,31],depression[31],fear of recurrence[33,34],and psychological distress[37]were identified.
Four studies explored symptom trajectories in patients with breast cancer within one year of surgery[20,21].Miaskowski et al.[20]stated that most patients did not have pain or had mild pain in the first six months after surgery(78.2%).However,approximately one-third of the patients experienced moderate arm pain.Similar patterns were observed for fatigue trajectories in this population.Bødtcher et al.[21]reported that about 80% of patients were grouped into a low fatigue group, while one-fifth were grouped into a high fatigue group in the first eight months after a cancer diagnosis.In contrast, a large proportion of the patients were bothered by significant sleep disturbance [25]and anxiety [30]within six months postoperatively.
Four studies explored psychological symptom trajectories in patients with breast cancer for more than one year after surgery[32-34,37].One study identified four trajectories of anxiety within two years following surgery, in which 93.6% of the patients reported decreased trajectories [32].In addition, a significant decrease appeared in the first year for trajectories of anxiety,followed by a slower rate of trend in the second year [32].The significant decrease in overall trajectories of fear of recurrence two months after surgery was earlier than that of anxiety[33].Patients also showed a high degree of interindividual variability regarding trajectories of fear of recurrence within six months after surgery[34].Unlike trajectories of anxiety and fear of recurrence, most patients (80.6%) reported having consistently and low-decreasing trajectories of psychological distress over one year after breast cancer surgery[37].
3.2.3.Symptom trajectories in patients who received cancer-related treatment
Nine studies identified symptom trajectories in patients who received cancer-related treatment.Trajectories of physical activity[13], cognitive function [14,15,17], cardiovascular function [18], fatigue [22,26], sleep disturbance [26], depression [29], and fear of recurrence [35]were identified in this population.Four studies identified symptom trajectories in patients who received systemic breast cancer treatment [13,14,17].
Lucas et al.[13]explored the trajectory of physical activity at baseline, six months later, and after primary breast cancer treatment.Patients with medium trajectories of physical activity accounted for the largest proportion of the sample (45.5%).However, a high percentage of patients also reported low trajectories(42.5%).Patients in the high vigorous-intensity physical activity group accounted for only approximately one-tenth of the sample,which suggested a lack of physical activity in this population.Trajectories for cognitive function showed a more positive trend.Bender et al.[17]examined trajectories of executive function,concentration, and visual working memory in early-stage postmenopausal patients receiving adjuvant therapy.However,patients were more likely to experience adverse trajectories of cognitive function during the first 18 months following chemotherapy [14].
Four studies targeted patients receiving chemotherapy for breast cancer.Three left ventricular ejection fraction trajectories were identified,in which stable and modest trajectories accounted for 91% of the sample [18].The opposite trend was identified in trajectories of fatigue [22]and sleep disturbance [26], in which most of the patients had elevated trajectories.Ng et al.[15]examined trajectories of cognitive function in early-stage patients receiving chemotherapy for breast cancer.Data were collected before chemotherapy(T1)and six weeks(T2),12 weeks(T3),and 15 months (T4) after chemotherapy.Five cognitive function trajectories were identified, with 53.4% of patients not reporting clinically significant cognitive issues, 16.0% reporting acute cognitive impairment in T2 and T3, 30.5% reporting clinically significant cognitive impairment at T4, and 11.5% reporting persistent cognitive impairment.These findings were not inconsistent with Mandelblatt et al.[16]or Bender et al.[17].One study explored trajectories of fear of recurrence in newly diagnosed patients receiving radiotherapy [35].The findings showed that the average trajectory of fear of recurrence was negative.
3.2.4.Associated factors
3.2.4.1.Socioeconomic factors.Age was identified as one of the predictors of symptom trajectories in patients with breast cancer.For instance, young patients were more likely to report symptom burdens of pain[20],sexual function[19],and depression[10].Old patients, especially those receiving chemotherapy, were susceptible to adverse trajectories of cognitive function[14,16,17].However,aging and retired patients reported low levels of depression after cancer diagnosis [27,28].
Regarding body mass index(BMI),patients who had a high BMI[20]were likely to report pain following breast cancer surgery and had low physical function and vitality after primary breast cancer treatment [13].An unhealthy lifestyle, including smoking cigarettes, may increase a patient’s risk of experiencing physical process trajectories [13].A sedentary lifestyle and low preoperative physical activity level were associated with high fatigue trajectories in patients following breast cancer surgery [21].
Family factors and education were predictors of trajectories of depression.Patients with low relationship quality [10], children living at home[29],and those with insufficient social support were more likely to report high trajectories of depression.In addition,divorced patients were more likely to report severe musculoskeletal pain and anxiety symptoms in the first five years following cancer diagnosis than nondivorced patients.Regarding education,patients with a low educational background were more likely to experience depression before radiation therapy [10,29].
3.2.4.2.Health characteristics.Numerous health characteristics were identified to impact symptom trajectories in patients with breast cancer.For instance, patients with persistent and high fatigue were more likely to be anxious in the context of breast cancer than those without such fatigue[21].Patients with high fatigue and poor cognitive function before therapy were more likely to report low trajectories of executive function, concentration, and visual working memory.Additionally,daily fatigue during chemotherapy was associated with patients’ health status [22,23].However, fatigue, in addition to low health status and multiple comorbidities,were predictors of high sleep disturbance preoperatively [25].
Low trajectories of depression were found to be related to only a few physical symptoms [27].In contrast, patients in good physical health showed a steep decrease in the trajectories of fear of recurrence over time beginning six months after breast cancer treatment [34].
Interactions of symptoms were found in symptom trajectories over time.For instance, there were associations between cooccurring symptoms and cognitive functions, whereby high levels of depression,anxiety,and fatigue at enrollment were predictors of a low degree of cognitive function [14].Similar trajectories of anxiety and depression were found in this review,which suggested a close association and interaction between the two symptoms[14,30].Regarding trajectories of distress,depression,nervousness,and pain were found to be predictors of a high-distress trajectory for patients one year after breast cancer surgery [37].
3.2.4.3.Cancer-related treatment.Cancer-related treatment was a significant predictor of adverse symptom trajectories, such as fatigue [23], cardiovascular function [18], anxiety [19], and depression [10,27,28].In the included studies, chemotherapy was one of the most commonly reported risk factors for depression [10,27,28]and cognitive function [14,17].Patients with the persistent decline or significant early decline trajectories of left ventricular ejection fraction were more likely to receive radiotherapy and another therapy than patients with a different trajectory [18].In addition,treatment with oophorectomy or ovarian suppression was associated with severe musculoskeletal pain and anxiety in young breast cancer patients [19].
4.Discussion
This review synthesized the existing knowledge to provide insight into symptom trajectories of patients with breast cancer.Despite overall similarities in appraisal at baseline, patients reported different symptom trajectories overtime associated with their sociodemographic, health, and cancer-related treatment characteristics.
Most of the included studies examined trajectories of symptoms and the relevant predictors,which allowed for the assumption that individuals belonged to underlying subgroups.For patients with breast cancer, most were likely to have low trajectories of depression [10,27,28,31].However, newly diagnosed patients tended to report high trajectories of depression in addition to persistent sleep disturbance problems, which should be considered [24,28].Young patients were likely to report trajectories of persistent and mild sexual symptoms [19].For early-stage patients with breast cancer,fatigue was a persistent symptom over time [23].However,cognitive function impairment was not common among old patients with breast cancer [16].
Among patients who underwent surgery, most reported significant sleep disturbance [25]and anxiety [30]shortly after surgery.However, a decreasing trend was likely to emerge one year after surgery[32].An earlier significant decrease was identified for overall trajectories of fear of recurrence within two months after surgery[33].A high burden of pain was not common for patients in the first six months after breast cancer surgery [20].However,approximately one-third of the patients experienced moderate arm pain, which showed a high degree of interindividual variability[20].Psychological distress did not present a decreasing trend,with most of the patients reporting low-decreasing trajectories of psychological distress consistently over one year after surgery [37].
For patients who received cancer-related treatment,only a small proportion had a high level of physical activity after cancer-related treatment over time [13], which suggests the need for nurses to promote their physical activity.Cognitive function impairment was not common among early-stage patients receiving adjuvant therapy,while chemotherapy could impair the cognitive function of old patients [15,17].Average negative trajectories of fear of recurrence were observed in the follow-up for newly diagnosed patients receiving radiotherapy [35].Elevated trajectories of fatigue and sleep disturbance [26]were found in patients receiving chemotherapy [22], while cardiovascular function impairment was less concerned in this population.
Interactions between symptoms should not be ignored when nurses evaluate and participate in patients with breast cancer.These interactions may change certain symptom trajectories.These results support existing evidence showing associations of depression and anxiety in patients with breast cancer [14,30,38,39].For distress,depression,and pain symptoms increase a patient’s risk of reporting high levels of distress trajectories after breast cancer surgery [37].Fatigue and sleep disturbance were two interacting symptoms in patients with breast cancer receiving chemotherapy[26].In addition,sleep disturbance issues could be exacerbated by symptoms,such as anxiety and pain[40],which may appear in the form of symptom clusters.The potential mechanism for such variation should be explored in future studies.
The results revealed some populations who were vulnerable to the related symptoms.For instance, old and postmenopausal patients with breast cancer,especially those receiving chemotherapy,seemed to be at high risk for cognitive impairment [16].Older women at diagnosis may have a less cognitive reserve, placing them at an increased risk for poor cognitive function with cancer therapy [17].However, young patients with breast cancer were more likely to report cancer-related sexual dysfunction,such as low desire, arousal or lubrication issues, and dyspareunia, demonstrating a need for targeted information support [19,41].In addition, newly diagnosed patients were vulnerable to negative trajectories of sleep quality [24], depression [28], and fear of recurrence [35].
A high BMI,a low relationship quality,parental responsibilities,insufficient social support, a low educational background, and an unhealthy lifestyle may increase the risk of negative symptom trajectories in patients with breast cancer.Concurring symptoms and poor health status also contributed to adverse symptom trajectories.Patients receiving chemotherapy, radiotherapy, oophorectomy, or ovarian suppression may be at high risk for adverse symptoms over time.These factors should be stressed in the evaluation and intervention of patients with breast cancer.
5.Strengths and limitations
Our study has several strengths.First, this is one of few studies to synthesize the available knowledge of symptom trajectories in patients with breast cancer and identify its predictors.Second,the integrative review method of Whittemore and Knafl was adopted to reduce potential bias.Some limitations should be acknowledged in this review.First, database searches were limited to PubMed,Embase, Web of Science, and CINAHL.Second, only peer-reviewed papers published in English were included, which may have impacted the generalization of the results.
6.Conclusion
This study illustrated interindividual variability in symptom trajectories among patients with breast cancer.Individual heterogeneities were identified in patients with different characteristics over time despite overall trends.The inclusion of sociodemographic,clinical and cancer-related treatment characteristics before the high-risk course, followed by targeted early preventive interventions conducted by nurses, is highly recommended.Future studies are needed to investigate how symptom trajectories are amenable to guide interventions that can aid in the long-term rehabilitation of patients with breast cancer.
Statement of ethics approval
This study does not need ethical approval as it is a review of literature.
Funding
This research was supported by the Youth Project of National Natural Science Foundation of China (72004033) and the Natural Science Foundation of China (72074054).The funding provided assistance in the language editing service of the manuscript.
CRediT authorship contribution statement
Tingting Cai:Conceptualization, Methodology, Writing - original draft, Writing - review & editing.Yueshi Huang:Data curation, Writing - review & editing.Qingmei Huang:Writing -review & editing, Funding acquisition.Haozhi Xia:Writing - review&editing.Changrong Yuan:Conceptualization,Methodology,Writing - original draft, Writing - review & editing, Funding acquisition.
Declaration of competing interest
The authors declare that there are no conflicts of interest.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2021.12.011.
 International Journal of Nursing Sciences2022年1期
International Journal of Nursing Sciences2022年1期
- International Journal of Nursing Sciences的其它文章
- The development of an evidence-informed Convergent Care Theory:Working together to achieve optimal health outcomes
- The development and implementation of a model to facilitate self-care of the professional nurses caring for critically ill patients
- Self-endangering: A qualitative study on psychological mechanisms underlying nurses’ burnout in long-term care
- Early mobilization implementation for critical ill patients: A crosssectional multi-center survey about knowledge, attitudes, and perceptions of critical care nurses
- Distress management in cancer patients:Guideline adaption based on CAN-IMPLEMENT
- Demand analysis of an intelligent medication administration system for older adults with chronic diseases based on the Kano model