
Efficacy of acupuncture as an adjuvant to speech and language therapy for aphasia after ischemic stroke:a protocol of systematic review and meta-analysis
2022-01-13 06:59:56BoMoSangShiZheDengTingHaoKaiHangSunTeBaJingBoZhaiXiaoFengZhaoZhiHongMeng
Medical Data Mining 2021年4期
Bo-Mo Sang ,Shi-Zhe Deng ,Ting Hao ,Kai-Hang Sun,Te Ba,Jing-Bo Zhai,Xiao-Feng Zhao*,Zhi-Hong Meng*
1Department of Clinical Acupuncture,First Teaching Hospital of Tianjin University of Traditional Chinese Medicine,Tianjin 300380,China.2National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion,Tianjin 300380,China.3Institute of Traditional Chinese Medicine,Tianjin University of Traditional Chinese Medicine,Tianjin 301617,China.
Abstract Background:Aphasia is one of the common complications of stroke.Speech and language therapy is a conventional treatment for aphasia following stroke.However,rehabilitation often remains unsatisfactory after speech and language therapy alone.Acupuncture may be effective for aphasia after stroke.We designed this systematic review to assess the efficacy and safety of acupuncture as an adjunct to speech and language therapy for aphasia following ischemic stroke.Methods: An extensive search will be performed in databases including Cochrane Central Register of Controlled Trials,PubMed,Web of Science,EMBASE,China National Knowledge Infrastructure,Sinomed,Wei Pu Date and Wan Fang Data.No limitation will be set in language,publication date or status of the study.The primary outcomes include scores of Western Aphasia Battery and Aphasia Quotient.The secondary outcomes include Scales of Clinical Rehabilitation Research Center Aphasia Examination,Communicative Abilities in Daily Living,Aphasia Battery of Chinese,Chinese Functional Communication Profile,adverse reactions,etc.Results: All of the data will be processed with Review Manager software.Cochrane ‘risk of bias’ tool will be used to assess the risk of bias.Conclusion: This study will contribute to the selection of appropriate therapies for aphasia after ischemic stroke and the development of clinical guidelines on this topic.
Key words:Acupuncture,Speech and language therapy,Aphasia,Ischemic stroke,Protocol
Background
Ischemic stroke is one of the leading causes of death worldwide [1].The prevalence of ischemic stroke is likely to increase globally [2].Aphasia occurs in one-third of patients with stroke and can disable brain areas associated with understanding,reading,writing,etc [3].A study reported that aphasia might increase the cost in stroke patients [4].
A guideline from American Heart Association recommends speech and language therapy (SLT) for aphasia following stroke [5].However,rehabilitation often remains unsatisfactory after SLT alone [6].Therefore,complementary therapies for aphasia after stroke are still needed.
Acupuncture has been used in China for thousands of years and has gained an increasing popularity in some Western countries.A systematic review showed that acupuncture could improve the neurological function of patients with stroke [7].A clinical study found that acupuncture could reduce the severity of aphasia and improve the ability of communication in daily life in patients with aphasia after stroke [8].Another research found that Xingnao Kaiqiao acupuncture combined with SLT could significantly improve the language function of patients with ischemic motor aphasia compared with SLT alone [9].We aim to conduct a systematic review to investigate the efficacy and safety of acupuncture as an adjuvant therapy to SLT for aphasia in patients with ischemic stroke.
Methods
This protocol is developed based on the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA-P) [10].It has been registered in PROSPERO (No.CRD42021230262).
Eligibility criteria
Types of studies.This meta-analysis will include randomized controlled trials of acupuncture therapy plus SLT for aphasia after ischemic stroke.The type of language used in the study or publication status will be unlimited. We will remove duplicates and quasi-randomized controlled trials.
Types of participants.Patients with aphasia following ischemic stroke will be considered.Stroke should be diagnosed according to the criteria from the World Health Organization,computerized tomography,magnetic resonance imaging,etc [11,12].Aphasia should be diagnosed according to Western Aphasia Battery (WAB),Aphasia Battery of Chinese (ABC),etc [13-15].
Types of interventions.Acupuncture combined with SLT will be considered in the experimental group.The type,frequency and duration of acupuncture will be unlimited.SLT alone or combined with sham acupuncture will be allowed in the control group.If possible,pharmacological or other non-pharmacological treatments should be the same between the two groups.
Outcome measures.The primary outcomes include WAB and Aphasia Quotient.The WAB is a tool to assess language functions associated with aphasia [13].Aphasia Quotient is a summary score calculated by WAB to measure the overall severity of language defect in aphasia [16].
The secondary outcomes include ABC,Chinese Functional Communication Profile,Clinical Rehabilitation Research Center Aphasia Examination,Communicative Abilities in Daily Living,adverse reaction,etc.ABC and Clinical Rehabilitation Research Center Aphasia Examination are developed to assess the impairment or severity of aphasia especially for Chinese patients [14,15].Chinese Functional Communication Profile is used to evaluate the verbal communication of aphasia patients after stroke [17].Communicative Abilities in Daily Living can be used to evaluate the daily activities [18].
Search strategies
We will search related studies in Web of Science,Cochrane Central Register of Controlled Trials,PubMed and EMBASE.Wan Fang,Sinomed,China National Knowledge Infrastructure and Wei Pu will be also reviewed since their inception.The search terms include cerebrovascular disorders,brain ischemia,stroke,aphasia,dysphasia,language,speech,acupuncture,electroacupuncture,acupoints,etc.We will also check the reference lists of included articles.Some international clinical trials registry platforms such as Clinical Trials.gov will also be searched.
Screening of studies
The studies identified from the extensive search will be checked independently by two researchers (KS,TB).The titles and abstracts will be checked based on the selection criteria listed above.If there is any doubt about whether the study should be excluded,we will review the full text of the study.The disagreements will be resolved by the other member of our research team (SD) who decides whether to include or exclude an article.Figure 1 shows the flow chart of screening studies [19,20].
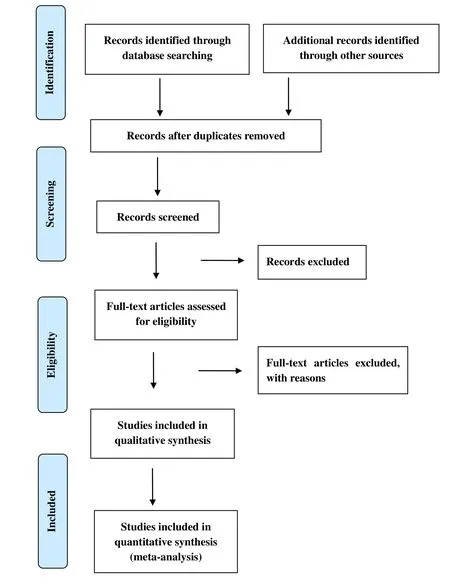
Figure 1 PRISMA flow chart of screening studies
Data extraction
The electronic data extraction table will be made with Excel and tested in advance.Two researchers (KS,TB)will independently tease out the information about participants,methods,interventions,outcomes,etc.Disagreement will be resolved by a third author (SD)or through discussion.If necessary,we will contact the author for more information.
Risk of bias assessment
The risk of bias for each included study will be assessed by two researchers (KS,TB) independently based on Cochrane 'Risk of bias' tool involving selection bias,performance bias,etc [21].The risk of bias in each part is classified as high,low,or unclear.A third researcher (SD) will resolve the disagreements.
Statistical analysis
We will use Review Manager V.5.3 software to perform the meta-analysis.Mean difference will be used for quantitative indicators measured by the same tool across studies.Standardized mean difference will be used for quantitative outcomes measured by the different tools across studies.Risk ratio will be used for dichotomous indicators.Meanwhile,95%confidence intervals of risk ratio,mean difference or standardized mean difference will be provided.The heterogeneity of the included studies will be evaluated byI2value.We will use the fixed-effects model to conduct the meta-analysis whenI2is less than 50%.IfI2is equal or greater than 50%,we will select the results of the meta-analysis with random-effects model.We will perform descriptive analysis when it is not feasible to combine results with the meta-analysis.Possible sources of the heterogeneity will be investigated by using subgroup analyses or sensitivity analysis.If necessary,publication bias will be assessed by the funnel plot,Begg’s or Egger’s test.
Classification of the evidence
We will use the GRADEpro Guideline Development Tool to create a summary table of results [22].The quality of the evidence will be assessed independently by two researchers (SD,TH) based on the Grading of Recommendations Assessment,Development and Evaluation (GRADE).Any dispute will be discussed and resolved by a third researcher (BS).
Discussion
We will comprehensively search relevant studies and critically evaluate the efficacy of acupuncture as an adjunct therapy to SLT for aphasia in patients with ischemic stroke.We will publish the results of this systematic review in a peer-reviewed scientific journal.Our findings will contribute to the selection of appropriate interventions for aphasia after ischemic stroke and the development of clinical guidelines on this topic.

- Medical Data Mining的其它文章
- Based on Network Pharmacology to Explore the Action Mechanism of Caulis Sinomenii-Caulis Piperis Kadsurae Herb Pair in the Treatment of Rheumatoid Arthritis
- Molecular mechanism of Mimenghua Granules in treating dry eye
- Construction of miRNA-mRNA regulatory network and drug prediction for ulcerative colitis associated colorectal cancer
- The research on rule of Acupoints and Massage Manipulations selection for Postischemic Stroke Constipation based on association rule and entropy clustering analysis
- NiuHuangJiangYa capsule for hypertension:a Bayesian dose-response analysis of multiple N-of-1 trials