
FMR1 allele frequencies in 51,000 newborns: a large-scale population study in China
2022-01-12 08:34YuZhangDingWenWuRuLaiYangLinZhuMengYiJiangWenJunWangXueKunLiXiaoLingJiangFanTongQiangShu
World Journal of Pediatrics 2021年6期
Yu Zhang ,2,3 · Ding-Wen Wu ,3 · Ru-Lai Yang ,3 · Lin Zhu · Meng-Yi Jiang · Wen-Jun Wang · Xue-Kun Li ,2,3 ·Xiao-Ling Jiang ,3 · Fan Tong ,3 · Qiang Shu ,3,5
Abstract
Keywords China · Fragile X syndrome · Fragile X mental retardation 1 ( FMR1) gene · Newborn screening · Population frequency
Introduction
Fragile X syndrome (FXS) is one of the most common causes of mental retardation, which accounts for about 20% ofindividuals with X-linked unknown intellectual developmental disorder (IDD) [ 1, 2]. FXS is caused by the amplification of CGG repeats in the 5′ untranslated region ofFMR1gene, which is located on Xq27.3. Amplification of CGG repeats leads to an aggravation of methylation of theFMR1promoter and causes severe inhibition onFMR1expression [ 3, 4]. Translation of certain genes is altered in the absence of FMR1 protein, which causes synaptic connection disturbance and affects the development of brain [ 4].Infants with FXS usually suffer from hypotonia and present with dysplasia in language. Hyperactivity, impulsivity, anxiety and seizures emerge in the second year of life and persist into adulthood. The altered physical features presented in some FXS individuals occur in adolescence, including prominent ears, a long face, flat feet, hyperextensible finger joints, double-jointed thumbs, soft skin and macroorchidism [ 4, 5].
CGG repeats range from 45 to 54 repeats are considered as intermediate, 55-200 repeats are considered as premutation, and CGG repeats over 200 repeats are defined as full mutation [ 3]. It is generally believed that the severity ofindividuals with FXS is associated with the number of CGG repeats. Heterozygous females with a premutation or full mutation allele have also been found to have related symptoms, such as fragile X-associated primary ovarian insufficiency (FXPOI) and fragile X-associated tremor ataxia syndrome (FXTAS) [ 4, 6].Heterozygous females with premutations have a high risk of mother-to-child transmission, through which the CGG repeats expand in their offspring [ 7, 8].
Individuals withFMR1mutations are usually diagnosed with developmental disorders and associated clinical features [ 3, 5, 9]. Though the effects of FXS start from the prenatal period, the symptoms are not obvious at birth [ 10, 11]. The average age of diagnosis of FXS is currently 36 months and can even be older in individuals with milder symptoms [ 11- 13]. This delay in diagnosis prevents early intervention and medical treatments for the affected individuals and also causes stress, financial burden and increased risk of having a second FXS child to the families. Newborn screening is thus needed to promote early identification and to provide family supports[ 14, 15].
In Europe and North America, the reported prevalence of the full mutation in the general population ranges from 1/4000 to 1/5000 in males and from 1/4000 to 1/8000 in females [ 4, 7, 16, 17]. The prevalence of premutation is estimated to range from 1/250 to 1/813 in males and from 1/110 to 1/270 in females [ 4, 15, 18]. A large-scale population survey on the frequencies ofFMR1alleles has not been conducted in the mainland of China. An FXS screening in 553 unrelated Chinese children with unknown IDD (453 males and 87 females) found 5 males with full mutation [ 19]. A small-scaleFMR1mutation screening in a 1145 unaffected Chinese (566 males and 579 females)identified only one premutation in a female [ 20]. The frequency of premutation allele in Taiwan Province of China was 1 in 1674, based on a screening of 10,046 newborn boys [ 21].
In the present study, we report the results of FXS screening in > 51,000 Chinese newborns to determine theFMR1allele frequency in general males and females by using GC-rich PCR and TP PCR systems combined with capillary electrophoresis to analyze the number of CGG repeats. A cohort of 33 children/families that had probands with scores < 2 standard deviations (S.D.) from the cutoff value of the Ages and Stages Questionnaire-Chinese also were subjected to FXS genetic testing to investigate the prevalence and heredity ofFMR1alleles in Chinese children characterized with suspected developmental delay.
Methods
Study population
The newborn screening of FXS was conducted in Children’s Hospital, Zhejiang University School of Medicine.A total of 51,661 validated samples taken from 28,114 male infants and 23,547 female infants were collected from the hospital Newborn Screening Center between April 2018 and April 2019. Informed consent was obtained from the parents according to the protocol approved by the Institutional Review Board of the Children’s Hospital of Zhejiang University School of Medicine (2018-IRB-076).
A second cohort ofindividuals was recruited from the Department of Behavioral Development of the Children’s Hospital, Zhejiang University School of Medicine.A parent-completed questionnaire, the Ages and Stages Questionnaire-Chinese (ASQ-C) [ 22], was used for developmental assessment. Children with scores < 2 SD from the cutoff value of ASQ in any domain were considered as suspected developmental delay and were enrolled in the FXS genetic testing. Informed consent was obtained from the parents with agreements for publication of any associated clinical information.
Molecular testing protocol
The procedure of the FXS screening is illustrated in Fig. 1.A similar procedure was used for the FXS genetic testing in the cohort of children with ASQ scores < 2 SD from the cutoff value (Supplementary Fig. S1).
Briefly, genomic DNA was extracted using MagaBio dry blood spot genomic DNA purification kit (BIOER, China)according to the manufacturer’s protocol and was quantified with a NanoDrop spectrophotometer (Thermo Scientific,Belgium). Primers specific toFMR1promotor CGG-repeat region were designed (FMR-F and FMR1-R in Supplementary Table S1). GC-rich PCR was prepared according to the manufacturer’s protocol (GC-rich PCR kit, Roche, Switzerland). The sizes of PCR products were analyzed by capillary electrophoresis. Briefly, 1 μL PCR products, 0.5 μL Liz-600 and 8.5 μL HIDI were mixed and heated at 95℃ for 5 min;then cooled on ice. The mixture was loaded onto the 3730xl Genetic Analyzer (Applied Biosystems, USA), and fragment lengths were read by GeneMarker HID V1.76 software. The number of CGG repeats was calculated according to the formula: CGG repeats = (fragment length - 221)/3 + 4. Typical capillary electrophoresis results of GC-rich PCR were shown in Supplementary Figure S3A-F.
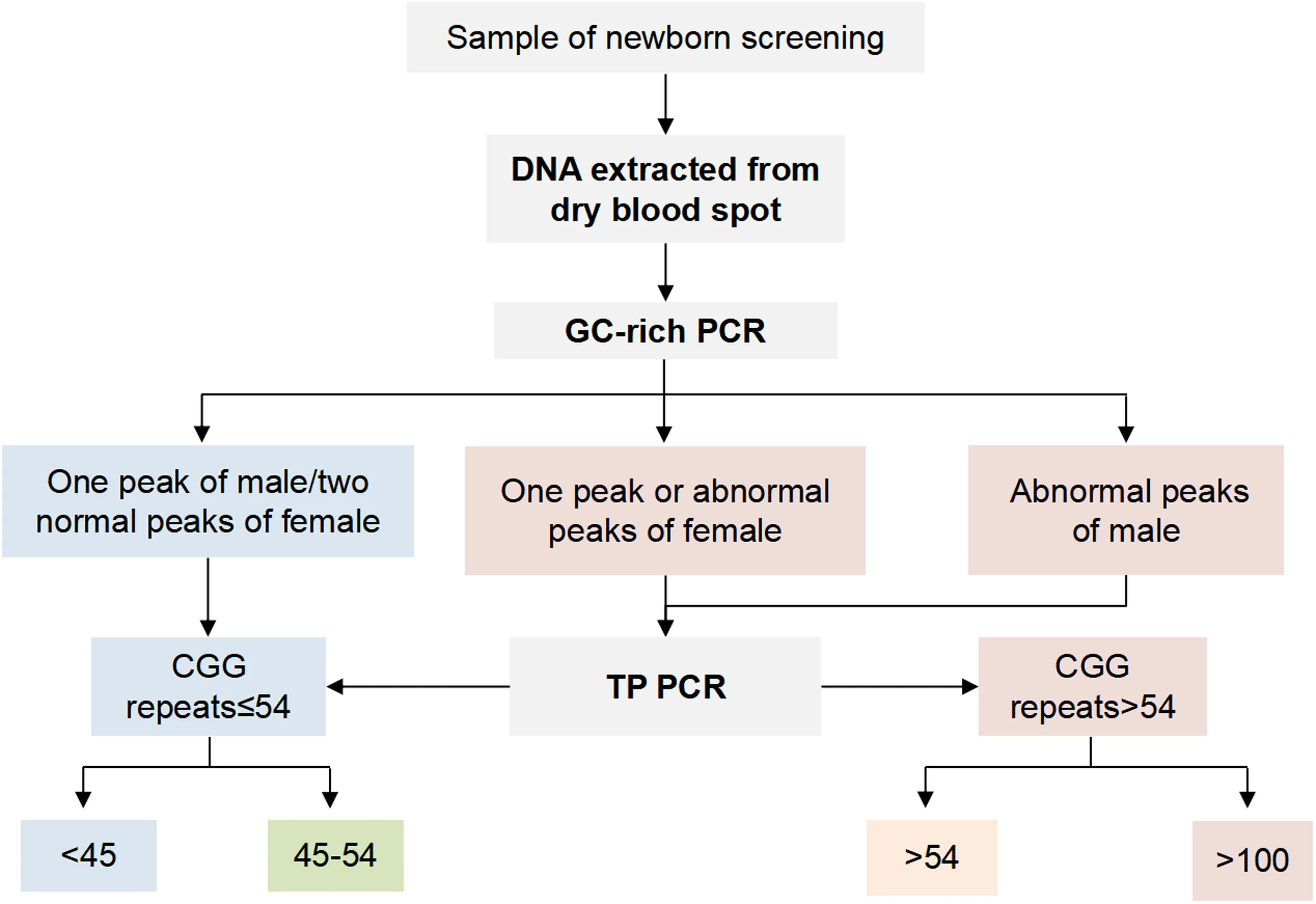
Fig. 1 Diagram of the newborn screening progress. Newborns were recruited from Children’s Hospital, School of Medicine, Zhejiang University from 2018 to 2019. Following the DNA extraction from dry blood spots, GC-rich PCR and TP PCR combined with capillary electrophoresis were performed subsequently to identify the size of the CGG repeats. TP PCR triple repeat primed PCR
A high-resolution and rapid PCR, triple repeat primed PCR (TP PCR), has been established to amplify accurate CGG repeats [ 23, 24]. We designed TP PCR primers to detect the mutation inFMR1and to distinguish normal homozygous and heterozygous large CGG repeats. Primers designed to produce continuous trapezoidal peak groups for TP PCR (FMR-F, tail-primer and TP-primer) are listed in Supplementary Table S1.PCR systems were prepared according to manufacturer’s protocol (GC-rich PCR kit, Roche, Switzerland), and capillary electrophoresis was performed subsequently as described earlier. The typical capillary electrophoresis results of TP PCR are shown in Supplementary Fig.S2 G-H.
Statistical analysis
All data are expressed as means ± standard error. GraphPad Prism (GraphPad Software Inc.) was used for statistical analysis. Unpaired student’sttest was used to determine the differences between groups.P< 0.05 was considered statistically significant.
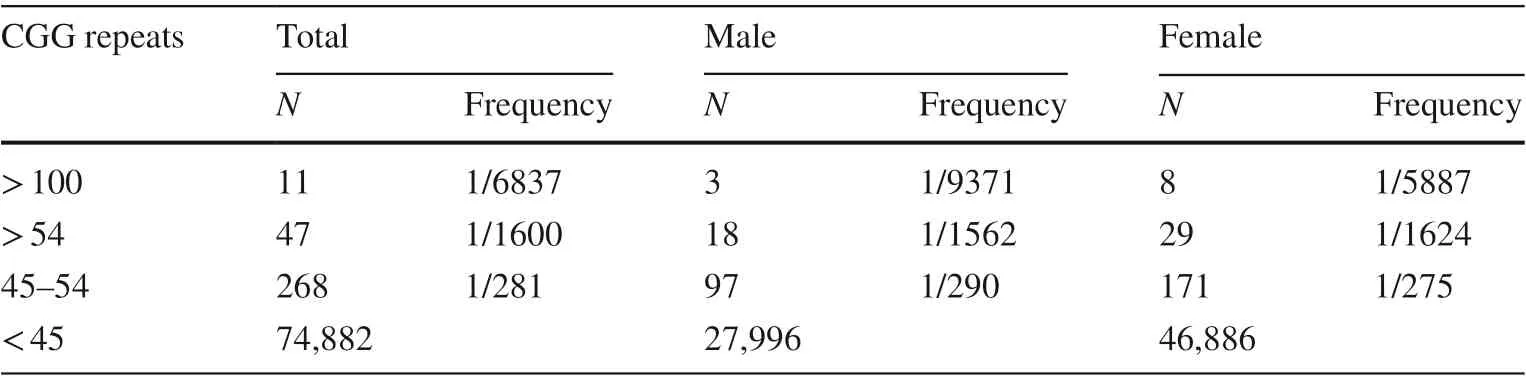
Table 1 Prevalence of fragile X syndrome mutations in the general newborn cohort
Results
FMR1 allele sizes and frequencies in males and females
FMR1allele sizes of 28,114 male infants and 23,547 female infants were analyzed in this study. We found 97 males with intermediate alleles (CGG repeats range from 45 to 54, 1/290) out of a total of 28,114 males (Table 1).Of the 18 males with CGG repeats > 54 (1/1562), three were with CGG repeats over 100 (1/9371). The average allele size in the 15 males with 55-100 repeats was 61.07 ± 1.375 repeats.
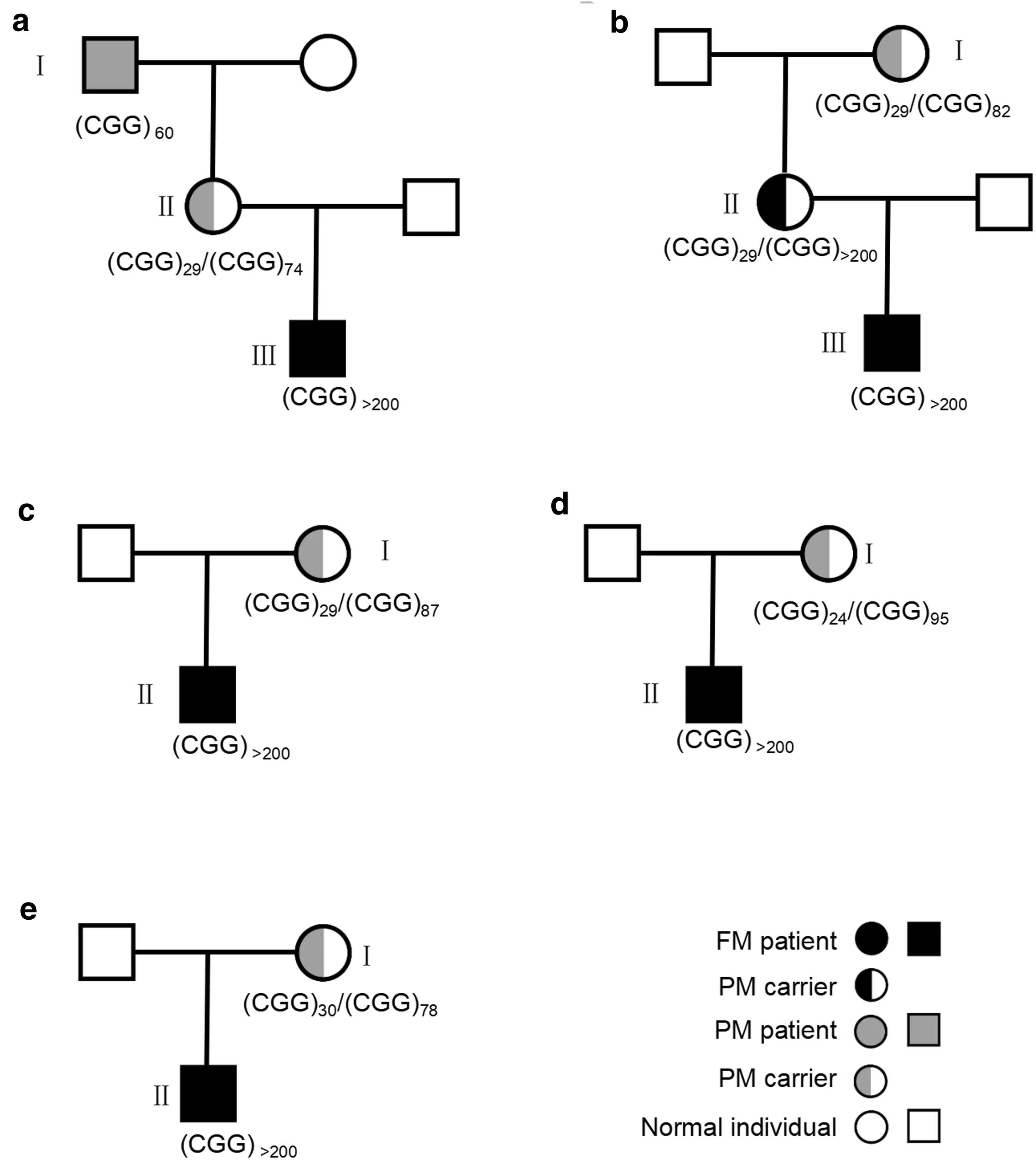
Fig. 2 Pedigrees of families with fragile X syndrome. Squares and circles denote males and females, respectively. Full mutation and premutation are presented as black symbols and grey symbols, respectively, whereas normal individuals are presented as white symbols. a:A male proband tested positive for full mutation with over 200 CGG repeats by blood spot. Further testing revealed that the proband’s mother had a premutation allele with 74 CGG repeats, and the maternal grandfather had a premutation allele with 60 CGG repeats, while the maternal grandmother had two normal alleles. b: A male proband with the full mutation, and his mother had a full mutation allele.Proband’s maternal grandmother was a premutation heterozygote with 82 CGG repeats. c, d, e: families with a male proband with full mutation whose mother had a premutation allele. FM full mutation,PM premutation. The validation data are shown in supplementary Figure S3
For female newborns, in a total of 47,094 X-chromosomes, 171 chromosomes were found with intermediate alleles (CGG repeats range from 45 to 54, 1/275) (Table 1).29 chromosomes were found with CGG repeats > 54(1/1624), of which, eight chromosomes were found withFMR1CGG repeats over 100 (1/5887). All the female newborns identified with CGG repeats > 54 were heterozygotes carriers. The average size of the alleles identified in females with 55-100 repeats was 68.14 ± 2.140 repeats(N= 21), which was significantly higher than that in males(P= 0.0233, unpaired Student’sttest).
FMR1 mutation frequency in children with ASQ scores < 2 SD
Clinical samples from 33 unrelated children with ASQ scores < 2 SD were analyzed with GC-rich PCR and TP PCR(Supplementary Table S2). A total of seven male patients were identified with FXS full mutation. One XXY male heterozygote and one female heterozygote with premutation also were identified in this cohort. Thus,FMR1mutations were present in up to 27.27% of children with ASQ scores < 2 SD.
Southern blot analysis or improved TP PCR was performed for the family members of five boys identified with full mutations (Fig. 2). The results showed that while one of the mothers carried heterozygous full mutation, all of the other four carried heterozygous premutations, indicating that premutation alleles were expanded to full mutations when transmitted from the mother.
Discussion
This study reported a large-scale FXS screening of newborns conducted in mainland China. The results revealed that the frequency of CGG repeats > 100 was 1/9371 in males and 1/2943 in females, and the frequency of CGG repeats > 54 was 1/1561 in males and 1/1624 in females.The frequency of intermediate allele was 1/290 in males and 1/275 in females. Our results suggested a lower prevalence of FXS premutation in Chinese than in Caucasians [ 4, 17, 18]. The prevalence of carriers with CGG repeats > 54 (1/812) identified in our study is higher than that reported previously, which was conducted in the adult Chinese Han population (1/1113) [ 20] and in the Japanese general population (0 in 1155) [ 25]. We also have investigated 33 children with suspected developmental delay(ASQ < 2 SD) forFMR1mutations and have found that the positive rate was as high as 27.27%. Family-based studies revealed that the number of CGG repeats amplified in X chromosome transmission.
Though premutation is less likely to cause mental retardation compared to full mutation, premutation could still cause late-onset disorders including learning and developmental problems at childhood and increased risk for anxiety, attention deficit, mild depression, hypertension, cardiac arrythmias and FXTAS in adulthood [ 4, 16]. For female carriers,FXPOI is another symptom needing vigilance [ 4, 16]. Premutation has a high risk of expansion to the full mutation when transmitted to offspring. Currently, the age of diagnosis for FXS full mutation is 35-37 months, and the age of diagnosis for FXS premutation is even older [ 26]. Early identification ofFMR1mutation by newborn screening allows more attention from medical care, proper treatments and information for further family planning.
In summary, we reported the first large-scale FXS screening conducted in the mainland of China with over 51,000 newborns. Our results supported the inclusion of FXS testing in newborn screening and especially for children who are susceptible to developmental delay, which would be helpful for early diagnosis and interventions.
Supplementary Information The online version contains supplementary material available at https:// doi. org/ 10. 1007/ s12519- 021- 00473-6.
Acknowledgements We would like to express our gratitude to the children and their families for their participation.
Author contributions JZ and DW contributed equally to this paper. QS and XL contributed to conceptualization and funding acquisition, JZ,DW, LZ, MJ and WW performed the investigation and data analysis,FT, DW and RY contributed to resources, data curation and validation.QS supervised the study, JZ and XJ drafted and revised the manuscript.XJ, FT and QS contributed equally to this paper. All authors have reviewed and approved the final manuscript.
Funding This study was supported by the Key Research and Development Program of Zhejiang Province (2017C03009 to Q. S.),the National Key Research and Development Program of China(2017YFC1001703 to Q. S.). Q. S. was also supported by the Fundamental Research Funds for the Central Universities (2014QNA6002).
Data availability statement The processed supporting data have been provided in the manuscript. Additional original data are only available from the corresponding author Q.S. on reasonable request.
Compliance with ethical standards
Ethical approval The study has been approved by the Institutional Review Board of the Children’s Hospital of Zhejiang University School of Medicine (2018-IRB-076). Informed consent to participate in the study have been obtained from the parents.
Conflict of interest Author Qiang Shu and Xue-Kun Li are members of the Editorial Board for the World Journal of Pediatrics. The paper was handled by the other Editor and has undergone rigrous peer review process. Author Qiang Shu and Xue-Kun Li were not involved in the journal's review of or decisions related to, this manuscript. In addition, two patents on the primers and testing kits used in this study were pending. No other financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
 World Journal of Pediatrics2021年6期
World Journal of Pediatrics2021年6期
- World Journal of Pediatrics的其它文章
- Muscle strength and its association with cardiometabolic variables in adolescents: does the expression of muscle strength values matter?
- Vestibular function of pediatric patients with sudden sensorineural hearing loss: based on vertigo symptom and vestibular function testing
- Evaluation of a new frequency-volume chart for children with primary monosymptomatic nocturnal enuresis: a prospective, comparative study
- Consensus statement on the epidemiology, diagnosis, prevention,and management of cow's milk protein allergy in the Middle East:a modified Delphi-based study
- Treatment of pediatric mild persistent asthma with low-dose budesonide inhalation suspension vs. montelukast in China
- Haploidentical hematopoietic stem cell transplantation for pediatric patients with chronic active Epstein-Barr virus infection:a retrospective analysis of a single center