
Dynamics of cytokines predicts risk of hepatocellular carcinoma among chronic hepatitis C patients after viral eradication
2022-01-12 08:32MingYingLuMingLunYehChingHuangShuChiWangYiShanTsaiPeiChienTsaiYuMinKoChingchihLinKuanYuChenYuJuWeiPoYaoHsuChengTingHsuTyngYuanJangTaWeiLiuPoChengLiangMingYenHsiehZuYauLinShinnCherngChenChungFengHuangJ
Ming-Ying Lu, Ming-Lun Yeh, Ching-l Huang, Shu-Chi Wang, Yi-Shan Tsai, Pei-Chien Tsai, Yu-Min Ko, Ching-chih Lin, Kuan-Yu Chen, Yu-Ju Wei, Po-Yao Hsu, Cheng-Ting Hsu, Tyng-Yuan Jang, Ta-Wei Liu, Po-ChengLiang,Ming-Yen Hsieh, Zu-Yau Lin, Shinn-Cherng Chen, Chung-Feng Huang, Jee-Fu Huang, Chia-Yen Dai,Wan-Long Chuang,Ming-Lung Yu
Abstract
Key Words: Hepatitis C virus; Hepatocellular carcinoma; Sustained virologic response;Tumor necrosis factor-α; Tumor necrosis factor-like weak inducer of apoptosis; Cytokine
INTRODUCTION
Chronic hepatitis C virus (HCV) infection is a major cause of liver cirrhosis and hepatocellular carcinoma (HCC). As HCV treatment evolves from an interferon (IFN)-based regimen to a therapy based on direct-acting antiviral agents (DAAs), it yields a sustained virologic response (SVR) rate of more than 97 % in chronic hepatitis C patients[1 ,2 ]. However, successful antiviral therapy does not eliminate HCC development. In a meta-analysis of observational studies, IFN therapy decreased the risk of HCC by 76 % in patients with bridging fibrosis or cirrhosis who achieved SVR[3 ].Recent studies have reported that HCC occurrence and recurrence rates are potentially increased in HCV patients treated with DAAs[4 -6 ]. This concern remains controversial due to the heterogeneous cohorts, variations in the inclusion criteria, and short duration of follow-up.
Persistent inflammation is a hallmark of chronic hepatic injury. HCV infection induces endogenous type I and III IFN activation, which activates natural killer (NK)cells[7 ] and leads to the expression of IFN-stimulated genes (ISGs)[8 ]. It causes profound alterations in the cytokine and chemokine signature in peripheral blood.HCV-specific CD8 + T cells play a central role in viral clearance. Chronic HCV infection is characterized by impaired HCV-specific CD8 + T cell responses resulting from viral escape and T cell exhaustion[9 ]. IFN-based therapy failed to recover the function of HCV-specific CD8 + T cells. This result suggested that the damage to CD8 + T cells might be permanent even after virus elimination[10 ]. In contrast, the combination of deleobuvir and faldaprevir resulted in the downregulation of programmed death-1 ,which led to rapid restoration of HCV-specific CD8 + T cell functions[11 ]. DAAmediated HCV clearance is correlated with mitigation of the IFN-α-induced immune response, followed by the downregulation of CXCL10 and CXCL11 and normalization of the phenotype and function of NK cells[12 ].
It is unclear whether host immunological modification after viral eradication influences the development of HCC. Although DAAs are the first choice for HCV clearance, they are not sufficient to abolish hepatic inflammation. Long-term inflammatory responses may change the liver microenvironment and cause irreversible hepatocyte damage. A rapid decline in HCV viral load induced by DAAs results in the reconstitution of immune surveillance[4 ]. HCV eradication during DAA treatment is accompanied by downregulation of type II and III IFN, their receptors, and downstream ISGs[13 ], which may affect the antitumor activity of immune cells. IFNs have immunomodulatory properties that regulate various immune cells to inhibit tumor proliferation and angiogenesis. Unlike IFNs, DAAs have neither antiproliferative nor antiangiogenic properties, which may allow the proliferation of malignant cells.
The identification of HCV patients who maintain a high risk of HCC following successful antiviral therapy remains an unmet need. Hepatocarcinogenesis despite HCV clearance is still unclear. First, this study aimed to investigate the impact of differential cytokine expression profiles on the development of HCC among chronic hepatitis C patients with advanced fibrosis who achieved SVR. Second, we attempted to identify immune biomarkers to predict the risk of HCC after successful antiviral therapy.
MATERIALS AND METHODS
Subjects
One hundred treatment-naïve chronic hepatitis C patients with advanced fibrosis treated with either pegylated IFN/ribavirin or IFN-free DAA who achieved SVR were recruited from Kaohsiung Medical University Hospital since 2003 . Patients were required to satisfy any one of the following criteria to be diagnosed with advanced fibrosis (F3 /4 ): Fibrosis-4 (FIB-4 ) index > 3 .25 [14 ], transient elastography (Fibroscan) >9 .1 kPa, or acoustic radiation force impulse elastography > 1 .81 m/s. The exclusion criteria were coinfection with hepatitis B, hepatitis D or human immunodeficiency virus; history of liver transplantation; prior presence of HCC; decompensated liver cirrhosis; malignancy; alcoholism; primary biliary cholangitis; α1 -antitrypsin deficiency; autoimmune hepatitis; renal function impairment; and psychiatric conditions.
Treatment
In the IFN group, the patients were subcutaneously administered peginterferon α-2 a(180 μg/wk) plus weight-based ribavirin (1200 mg/d for weights ≥ 75 kg or 1000 mg/d for weights < 75 kg) for 24 to 48 wk depending on the HCV genotype. In the DAA group, the physician selected IFN-free DAA regimens for 12 to 24 wk that were discreetly based on the HCV international treatment guidelines (The Asian Pacific Association for the Study of the Liver, European Association for the Study of the Liver and American Association for The Study of Liver Diseases).
Outcome assessment
SVR was defined as undetectable HCV RNA throughout 12 wk (SVR12 ) for the DAA group or 24 wk (SVR24 ) for the IFN group after completion of antiviral therapy[15 ,16 ].The primary endpoint was the occurrence of new-onset HCC. Standard HCC surveillance [abdominal ultrasound and α-fetoprotein (AFP) every six months] was performed during the follow-up[17 ]. HCC development within six months of initiation of antiviral treatment was excluded. Proof of HCC was directly linked to the National Cancer Registration of Taiwan in Health and Welfare Data Science Center (Taiwan).This study was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (No. KMUHIRB-E(I)-20180307 & KMUHIRB-G(II)-20170020 ).Written informed consent was acquired from all participants.
HCV genotyping and quantification
Anti-HCV antibodies were identified by a third-generation commercially available enzyme-linked immunosorbent assay (Abbott Laboratories, Chicago, IL, United States). HCV RNA was quantified by real-time polymerase chain reaction assay with a lower limit of detection of 12 IU/mL (RealTime HCV; Abbott Molecular, Des Plaines IL, United States)[18 ]. HCV genotypes were determined using a commercial kit(Abbott RealTime HCV Genotype II; Abbott Molecular, Des Plaines, IL, United States).
Cytokine measurement
Serum samples were collected from the participants at baseline and SVR24 . In total, 64 serum cytokines and chemokines (Supplementary Tables 1 -3 ) were measured by the magnetic bead multiplex immunoassay according to the manufacturer’s instructions(Merck KGaA, Darmstadt, Germany)[19 ,20 ]. In brief, a calibration curve based on 1 :3 dilutions of the highest standard was used for quantification. Beads were premixed and put into wells containing diluted serum and reagents. After fixation of the antigen on the capture antibody linked with the microspheres, a biotinylated detection antibody was added. The concentration of the analyte was quantified based on the bead color and the intensity of the fluorescent signal using the multiplex Luminex-200 (Luminex Corporation, Austin, TX, United States). All samples were analyzed in duplicate.
Statistical analysis
Student’sttest and the Mann-WhitneyUtest were performed to compare the continuous variables. The chi-square (χ2) test with Yates correction or Fisher’s exact test was used to assess the categorical variables. Differences in the cumulative incidence of HCC between groups were analyzed by Kaplan-Meier survival analysis and the log-rank test. The risk factors for HCC were evaluated using multivariate Cox regression analysis. In conjunction with receiver operating characteristic area (ROC)analysis[21 ], the optimum cutoff value to distinguish between the risk strata was calculated by the Youden index[22 ]. The performance of biomarkers to predict the risk of HCC was calculated by time-dependent ROC curve analysis. The area under the ROC area (AUROC) was assessed by the timeROC package of R software (http://www.r-project.org). The statistical power for the comparison of survival curves between two groups under the Cox proportional hazards model was calculated by the powerSurvEpi package of R software. A two-tailedPvalue < 0 .05 was considered statistically significant. The statistical analysis was conducted by the Statistic Packages for Social Science Program (SPSS v19 .0 for Windows, SPSS Inc., United States). The statistical methods of this study were reviewed by Dr. Tsai PC from Kaohsiung Medical University.
RESULTS
Baseline demographics
The baseline demographics of the study subjects are shown in Table 1 . There were no significant differences in age, sex, HCV genotype, FIB-4 index, or AFP levels between the DAA and IFN groups. HCV RNA was significantly higher in the DAA group thanin the IFN group. Aspartate aminotransferase, alanine aminotransferase and hemoglobin A1 c (HbA1 c) were significantly elevated in the IFN group compared to the DAA group.

Table 1 Baseline demographics of study subjects
Cumulative probability of HCC development
HCC developed in 12 (IFN group n = 11 , DAA group n = 1 ) of the 97 patients over 459 person-years of follow-up. Three patients were excluded because HCC occurred within six months of initiation of the antiviral treatment. The mean follow-up time was 7 .46 years [interquartile range (IQR) = 3 .65 -12 .23 ] in the IFN group and 1 .84 years (IQR= 1 .19 -2 .43 ) in the DAA group. The annual incidence of HCC was 2 .95 % in the IFN group and 1 .16 % in the DAA group. The Kaplan-Meier survival analysis showed no statistical significance in the accumulative probability of HCC between the IFN and DAA groups (log-rankPvalue = 0 .712 ) (Figure 1 ).
Cytokines associated with HCC development

Figure 1 Kaplan-Meier survival analysis. HCC: Hepatocellular carcinoma; IFN: Interferon; DAA: Direct-acting antiviral agent.
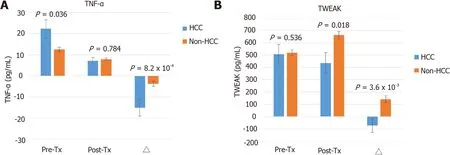
Figure 2 Cytokine expression between the hepatocellular carcinoma and non-hepatocellular carcinoma groups among chronic hepatitis C patients with advanced fibrosis. A: Tumor necrosis factor-α; B: Tumor necrosis factor-like weak inducer of apoptosis. Δ = (posttreatment cytokine level) -(pretreatment cytokine level). The bar represents the means ± SE. The P value was tested by the Mann-Whitney U test. HCC: Hepatocellular carcinoma; TNF-α:Tumor necrosis factor-α; TWEAK: TNF-like weak inducer of apoptosis; IFN: Interferon; Pre-Tx: Pretreatment; Post-Tx: Posttreatment.
In total, 64 cytokines were used to analyze the relationship with HCC (Supplementary Table 1 ). Seven of the sixty-four cytokines were excluded from subsequent analysis because more than 80 % of the samples were below the limit of detection.Members of the tumor necrosis factor (TNF) superfamily, including TNF-α and TNFlike weak inducer of apoptosis (TWEAK), were associated with the development of HCC. The baseline TNF-α level was significantly elevated in the HCC group compared to the non-HCC group (22 .22 ± 4 .33 vs 12 .53 ± 1 .03 pg/mL, P = 0 .036 ). There was no significant difference in the posttreatment TNF-α levels between the HCC and non-HCC groups. The change in TNF-α levels (ΔTNF-α) before and after treatment significantly differed between the HCC and non-HCC groups (-15 .11 ± 3 .93 vs -3 .78 ±1 .16 pg/mL, P = 8 .2 × 10 -4 ) (Figure 2 A). The baseline TWEAK expression was similar in both groups. The posttreatment TWEAK level was significantly lower in the HCC group than in the non-HCC group (434 .82 ± 84 .18 vs 660 .65 ± 30 .34 pg/mL, P = 0 .018 ).ΔTWEAK showed a reciprocal change between the HCC and non-HCC groups and achieved statistical significance (-71 .78 ± 54 .56 vs 142 .81 ± 27 .69 pg/mL, P = 3 .6 × 10 -3 )(Figure 2 B).
Among the HCV patients treated with pegIFN/ribavirin, the baseline TNF-α level was significantly higher in the HCC group than in the non-HCC group (22 .55 ± 4 .72vs9 .13 ± 7 .79 pg/mL, P = 0 .017 ). The posttreatment TNF-α concentration was comparable between the HCC and non-HCC groups. ΔTNF-α levels significantly declined in HCC compared to non-HCC patients (-15 .86 ± 4 .22 vs -4 .56 ± 1 .85 pg/mL, P = 0 .007 )(Supplementary Figure 1 A). The dynamic change in TWEAK did not show significant variations between the HCC and non-HCC groups (Supplementary Figure 1 B).
Cox regression analysis of the relationship between the differentially expressed cytokines and HCC
In univariate Cox regression analysis, FIB-4 (≥ 9 vs < 9 , crude HR = 4 .04 , 95 %CI: 1 .27 -12 .86 , P = 0 .018 ), HbA1 c (≥ 7 vs < 7 %, crude HR = 5 .38 , 95 %CI: 1 .38 -20 .99 , P = 0 .015 ),pretreatment TNF-α (≥ 18 vs < 18 pg/mL, crude HR = 5 .15 , 95 %CI: 1 .57 -16 .87 ,P=0 .007 ), ΔTNF-α (≤ -5 .7 vs > -5 .7 pg/mL, crude HR = 11 .07 , 95 %CI: 2 .27 -53 .87 , P = 0 .003 ),and ΔTWEAK (≤ -70 vs > -70 pg/mL, crude HR = 4 .01 , 95 %CI: 1 .20 -13 .40 , P = 0 .024 )were significant predictors of HCC. Multivariate stepwise Cox regression analysis revealed that ΔTNF-α was the only independent risk factor for HCC (HR = 11 .54 ,95 %CI: 2 .27 -58 .72 , P = 0 .003 ) (Table 2 ).
Among the HCV patients treated with pegIFN/ribavirin, univariate Cox regression showed that the significant predictors of HCC included sex, FIB-4 (≥ 9 vs < 9 ), HbA1 c,baseline TNF-α (≥ 18 vs < 18 pg/mL) and ΔTNF-α (≥ -5 .7 vs < -5 .7 pg/mL). The association between ΔTWEAK (≤ -70 vs > -70 pg/mL) and HCC was borderline statistically significant. Stepwise multivariate Cox regression revealed that the ΔTNF-α level was the only independent risk factor for HCC in the IFN group (HR = 9 .98 , 95 %CI:1 .88 -52 .87 , P = 0 .007 (Supplementary Table 2 ).
Subgroup analysis for the association between TNF-α and HCC
Since age and diabetes mellitus were important risk factors for HCC, the subjects were further stratified by age and HbA1 c. The high- and low-risk groups were dichotomized based on ΔTNF-α with a cutoff value of -5 .7 pg/mL. The multivariate Cox regression analysis revealed that the high-risk group (ΔTNF-α ≤ -5 .7 pg/mL) had an 11 -fold cumulative probability of HCC compared to that of the low-risk group (HR =11 .02 , 95 %CI: 1 .86 -65 .17 , P = 0 .008 ) among HCV patients with HbA1 c less than 7 %. In the younger population (age < 65 years old), the HCC risk was borderline significant between the high- and low-risk groups (HR = 8 .51 , 95 %CI: 0 .78 -92 .86 , P = 0 .079 ).Among patients with both HbA1 c < 7 % and age below 65 years old, the high-risk group had a 20 -fold cumulative probability of HCC in comparison with the low-risk group (HR = 19 .99 , 95 %CI: 0 .90 -443 .91 , P = 0 .058 ) (Figure 3 ). The level of ΔTNF-α did not influence the development of HCC in either the patients aged ≥ 65 years old or with HbA1 c ≥ 7 % (Supplementary Figure 2 ).
HCC predictive model
Based on previous analyses, the FIB-4 index, HbA1 c, ΔTNF-α, and ΔTWEAK were selected as parameters to predict the risk of HCC. The HCC predictive model was as follows: Score = 4 × FIB-4 (≥ 9 , yes = 1 , no = 0 ) + 5 × HbA1 c (≥ 7 , yes = 1 , no = 0 ) + 11 ×ΔTNF (≤ -5 .7 , yes = 1 , no = 0 ) + 4 × ΔTWEAK (≤ -70 , yes = 1 , no = 0 ).
The weighting coefficient for each parameter was derived from the crude hazard ratio of the univariate Cox proportional hazards model. The performance of this HCC predictive model was assessed by time-dependent ROC curve analysis. In overall cases, the 3 -year, 5 -year, 10 -year, and 13 -year areas under the ROC curve (AUCs) were 0 .882 , 0 .864 , 0 .903 , and 1 .000 , respectively (Figure 4 A). In the IFN group, the 3 -year, 5 -year, 10 -year, and 13 -year areas under the ROC curve (AUCs) were 0 .782 , 0 .802 , 0 .870 ,and 1 .000 , respectively (Figure 4 B).
Kaplan-Meier analysis for HCV patients stratified by risk scores
To classify the predictive score according to the risk of HCC, the patients were further stratified into low- (score = 0 -7 ), intermediate- (score = 8 -15 ), and high-risk groups(score > 15 ). In the high-risk group, the 3 -year, 5 -year, and 10 -year cumulative risks of HCC were 20 .0 %, 40 .0 %, and 60 .0 %, respectively. In the intermediate-risk group, the 3 -year, 5 -year, and 10 -year cumulative probabilities of HCC were 11 .4 %, 16 .9 %, and 31 .0 %, respectively. In contrast, none of the low-risk patients had HCC within 14 years of follow-up after successful viral eradication among the overall cases (log-rankPvalue = 6 .8 × 10 -6 ) (Figure 5 A). Likewise, the Kaplan-Meier survival analysis revealed a significant difference in the cumulative probability of HCC among the IFN group stratified by the risk scores (log-rankPvalue = 9 .6 × 10 -5 ) (Figure 5 B).
DISCUSSION
This study revealed that there was no significant difference in the risk of HCC between the DAA and IFN groups after successful antiviral therapy. Downregulation of TNF-α and TWEAK increased the risk of hepatic carcinogenesis. ΔTNF-α was identified as an independent predictor of new-onset HCC among HCV patients with SVR. The effect of TNF-α was more prominent in young adults with normoglycemia. An HCC predictive model comprising FIB-4 , HbA1 c, ΔTNF-α, and ΔTWEAK had excellent performance,with 3 -, 5 -, 10 -, and 13 -year areas under the curve of 0 .882 , 0 .864 , 0 .903 , and 1 .000 ,respectively. The 5 -year accumulative risk of HCC was 0 .0 %, 16 .9 %, and 40 .0 % in the low-, intermediate-, and high-risk groups, respectively. These findings remained statistically significant among the HCV patients treated with pegIFN/ribavirin.Because there was only one HCC in the DAA group, the role of TNF-α in HCC shouldbe further verified in this population. The HCC risk could be modified by the preexisting host background and adjusted by the immune signatures after viral eradication. This predictive model helps clinicians adopt appropriate surveillance strategies for chronic hepatitis C patients following successful antiviral therapy according to the risk of HCC.

Table 2 Factors associated with the onset of hepatocellular carcinoma: Univariate and multivariate Cox regression models
Our study showed that elevation of pretreatment TNF-α levels raised the possibility of new-onset HCC. Consistent with our study, Tarhuniet al[23 ] found that HCVrelated cirrhotic patients carrying TNF-α 308 G>A had higher basal TNF-α production and exhibited a higher risk of HCC. Elevated basal TNF-α indicates sustained hepatic inflammation accompanied by persistent liver damage, which is susceptible to carcinogenesis. A systematic review showed that TNF-α was one of the strongest host genetic predictors for HCC in HCV-infected patients[24 ]. These findings suggested that the immune background was affected before antiviral therapy.
Interestingly, the abrupt decline in TNF-α levels after successful antiviral therapy increased the risk of HCC in our study. This implies a potential modification of the immune milieu by antiviral therapy that may trigger HCC development. Stimulation of the immune system effectively protects tissues from malignant cell invasion. Both cytotoxic T lymphocytes and NK cells are potent effectors in immune surveillance.TNF-α mediates the immune response against tumor cells by creating a microenvironment toward immunogenic activation rather than suppression[25 ]. Suppression of TNF signaling enables tumor cells to evade attack by cytotoxic T lymphocytes and attenuatein vivoantitumor responses[26 ]. Antiviral therapy may disrupt the balance from TNF-α activation to inhibition in immune surveillance. Alternatively, Debeset al[27 ] found that HCV patients with early-onset or recurrent HCC within 18 mo maintained stable or even higher TNF-α levels after DAA therapy. This implied that those patients might exhibit precarcinogenic or ongoing carcinogenic activity induced by TNF-α in response to occult HCC.

Figure 3 Multivariate Cox regression analysis of tumor necrosis factor-α associated with hepatocellular carcinoma in subgroups.Comparison of the cumulative probability of hepatocellular carcinoma development divided by Δtumor necrosis factor-α with a cutoff value of -5 .7 pg/mL in patients with (A) hemoglobin A1 c (HbA1 c) < 7 %, (B) age < 65 years old and (C) HbA1 c < 7 % and age < 65 years old. The P value was adjusted by age, sex, Fibrosis-4 index,and HbA1 c. HR: Hazard ratio; CI: Confidence interval; HCC: Hepatocellular carcinoma; TNF-α: Tumor necrosis factor-α; HbA1 c: Hemoglobin A1 c.

Figure 4 Time-dependent receiver operating characteristic curve analysis for the hepatocellular carcinoma predictive model. IFN:Interferon; AUC: Area under the curve.
Both TNF-α and TWEAK belong to members of the TNF superfamily. These cytokines are mainly produced by macrophages, monocytes, and lymphocytes.TWEAK is a multifunctional cytokine that regulates a variety of cellular activities,including cell proliferation, differentiation, apoptosis, inflammation, and angiogenesis,viathe fibroblast growth factor-inducible 14 receptor[28 ]. TWEAK appears to attenuate the innate response switch to adaptive immunity[29 ]. In addition, TWEAK is a weak inducer of apoptosis and also participates in tissue repair[30 ]. In chronic liver injury and repair, TWEAK appears to initiate liver progenitor cell expansion and ductal proliferation[31 ]. Hyperstimulation of inflammatory cells simultaneously results in excessive matrix deposition by activated hepatic stellate cells and myofibroblastsviathe lymphotoxin-β signaling pathway[32 ]. Our study showed that posttreatment TWEAK expression was upregulated in the non-HCC group. Viral clearance alleviates the inflammatory status in the liver. It provides a microenvironment to facilitate the reconstruction of hepatocytes aided by TWEAK, which may further delay HCC development.
Our study confirms the consensus that DAA treatment does not markedly increase the risk of HCC compared to IFN treatment[33 ]. Most evidence has shown a decline in HCC risk regardless of whether SVR was achieved by IFN alone, DAA-only, or combined regimens[34 ]. However, successful antiviral therapy cannot eliminate the risk of HCC. The standard surveillance strategy (ultrasound and AFP every six months) advocates for all HCV patients. However, interindividual variations in HCC risk raise the question of whether the recommendations for HCC screening should be adjusted. Age, male sex, diabetes mellitus, and advanced fibrosis are well-known independent predictors of HCC after viral eradication[35 -37 ]. In the absence of diabetes mellitus and old age (> 65 years old), the presence of ΔTNF-α ≤ -5 .7 pg/mL increased the risk of HCC in patients with advanced fibrosis by 20 -fold after HCV clearance. According to this HCC predictive model, patients with scores exceeding 15 should be closely monitored, since the 5 -year cumulative risk of HCC reaches up to 40 .0 %. Nevertheless, none of the HCC cases had been identified over 14 years of follow-up in patients with a score of less than 7 . The surveillance intervals may be extended among HCV patients achieving SVR in the absence of concurrent risk factors.In the post-DAA era, the risk model-based algorithm provides a cost-effective surveillance strategy for HCC.

Figure 5 Kaplan-Meier survival analysis for chronic hepatitis C patients stratified by the risk scores. IFN: Interferon.
The advancement of high-throughput technology makes early HCC detection more feasible. Currently, integrating multiomics data for HCC screening is also frequently observed[38 ]. The GALAD score consists of clinical factors (sex, age) and biomarkers(AFP, AFP-L3 , and Des-carboxyprothrombin) that have an excellent performance to predict HCC, with an AUROC up to 0 .97 [39 ]. Using a miRNA panel (miR-22 , miR-199 a-3 p) with AFP provided high diagnostic accuracy (AUROC = 0 .988 ) for the early detection of HCC in HCV patients[39 ]. The methylation pattern of circulating cell-free DNA (APC, SFRP1 , GSTP1 , and RASSF1 A) has demonstrated sufficient detection value to distinguish HCC patients from healthy controls[40 ]. Nevertheless, a majority of studies collected a cohort with a small sample size, and the analytical methods varied even in the same testing platform. These factors have limited the clinical application of these biomarkers.
Even though the sample size was limited in this pilot study, the statistical power was sufficient to be reliable. In overall cases, the statistical power of the association between ΔTNF-α and HCC was 99 .9 % to reject the null hypothesis at a P value < 0 .05 under a hazard ratio of 11 .54 . In the IFN group, the statistical power of ΔTNF-α on HCC risk was 94 .6 % to reject the null hypothesis at a P value < 0 .05 under a hazard ratio of 9 .98 . There are several limitations to this study. Although expensive IFN-free DAAs have been on the market since 2014 , the National Health Insurance in Taiwan has reimbursed DAAs for HCV patients with advanced fibrosis since 2017 . The followup time in most HCV patients treated with DAAs was less than 3 years. Owing to the small sample size and short follow-up time of the DAA group, a larger study cohort is necessary to validate the performance of this predictive model. IFN may induce distinct host immune alterations in comparison with DAA. As only one HCC case was identified in the DAA group throughout the follow-up period, it was unable to compare the diversity of cytokine profiles regarding HCC between the IFN and DAA groups. This predictive model was restricted to HCV patients with advanced fibrosis following successful antiviral therapy. Additionally, the optimal cutoff value should be further verified in other populations. The parameters of this predictive model were composed of serum cytokines involving the TNF superfamily. Host inflammation elicited by other etiologies may interfere with the predictive accuracy. Serum cytokines may not reflect the microenvironment within hepatocytes. To interpret this HCC predictive model, more care should be given to HCV patients presenting coinfection with other viruses, inflammatory disease, or malignancies.
CONCLUSION
This study revealed that downregulation of TNF-α increases the risk of HCC among HCV patients following successful antiviral therapy. Inhibition of TNF-α may attenuate host immune surveillance against tumor cells. Our findings provide a clue for the pathogenesis of hepatocarcinogenesis and a strategy for HCC surveillance based on risk stratification. With the development of high-throughput molecular technology, it is believed that more novel biomarkers will be applied in the early detection of HCC in the future.
ARTICLE HIGHLIGHTS


Research conclusions
Downregulation of serum TNF-α significantly increased the risk of HCC after HCV eradication.
Research perspectives
Our findings provide a clue for the pathogenesis of hepatocarcinogenesis and a strategy for HCC surveillance based on risk stratification.
 World Journal of Gastroenterology2022年1期
World Journal of Gastroenterology2022年1期
- World Journal of Gastroenterology的其它文章
- Viral hepatitis in 2021 : The challenges remaining and how we should tackle them
- Risk of hepatocellular carcinoma after hepatitis C virus cure
- Artificial intelligence in the diagnosis and management of colorectal cancer liver metastases
- Advances in traction methods for endoscopic submucosal dissection: What is the best traction method and traction direction?
- Focal adhesion kinase-related non-kinase ameliorates liver fibrosis by inhibiting aerobic glycolysis via the FAK/Ras/c-myc/ENO1 pathway
- Gastric pentadecapeptide BPC 157 in cytoprotection to resolve major vessel occlusion disturbances,ischemia-reperfusion injury following Pringle maneuver, and Budd-Chiari syndrome