
Anatomic resection improved the long-term outcome of hepatocellular carcinoma patients with microvascular invasion:A prospective cohort study
2022-01-10 07:59JiangMinZhouChenYangZhouXiaoPingChenZhiWeiZhang
Jiang-Min Zhou,Chen-Yang Zhou,Xiao-Ping Chen,Zhi-Wei Zhang
Jiang-Min Zhou,Chen-Yang Zhou,Zhi-Wei Zhang,Hepatic Surgery Center,Tongji Hospital,Tongji Medical College,Huazhong University of Science and Technology,Wuhan 430030,Hubei Province,China
Xiao-Ping Chen,Translational Medicine Center,Tongji Hospital,Tongji Medical College,Huazhong University of Science and Technology,Wuhan 430030,Hubei Province,China
Abstract BACKGROUND The long-term effect of anatomic resection (AR) is better than that of nonanatomic resection (NAR).At present,there is no study on microvascular invasion(MVI) and liver resection types.AIM To explore whether AR improves long-term survival in patients with hepatocellular carcinoma (HCC) by removing the peritumoral MVI.METHODS A total of 217 patients diagnosed with HCC were enrolled in the study.The surgical margin was routinely measured.According to the stratification of different tumor diameters,patients were divided into the following groups:≤ 2 cm group,2-5 cm group,and > 5 cm group.RESULTS In the 2-5 cm diameter group,the overall survival (OS) of MVI positive patients was significantly better than that of MVI negative patients (P=0.031).For the MVI positive patients,there was a statistically significant difference between AR and NAR (P=0.027).AR leads to a wider surgical margin than NAR (2.0 ± 2.3 cm vs 0.7 ± 0.5 cm,P<0.001).In the groups with tumor diameters<2 cm,both AR and NAR can obtain a wide surgical margin,and the surgical margins of AR are wider than that of NAR (3.5 ± 5.8 cm vs 1.6 ± 0.5 cm,P=0.048).In the groups with tumor diameters > 5 cm,both AR and NAR fail to obtain wide surgical margin(0.6 ± 1.0 cm vs 0.7 ± 0.4 cm,P=0.491).CONCLUSION For patients with a tumor diameter of 2-5 cm,AR can achieve the removal of peritumoral MVI by obtaining a wide incision margin,reduce postoperative recurrence,and improve prognosis.
Key Words:Microvascular invasion;Hepatocellular carcinoma;Anatomic resection;Surgical margin;Recurrence;Surgery
INTRODUCTION
Hepatocellular carcinoma (HCC) is one of the most common malignancies worldwide,and its high mortality makes it the second leading cause of cancer death[1].Although the poor prognosis of HCC has improved significantly over the last decade due to increased knowledge of HCC behavior,improvements in staging systems,and multiple therapeutic options compared with other malignancies,HCC still has a high mortality rate[2].The prognosis of HCC remains very poor due to the high incidence of recurrence and metastasis,and the 5-year recurrence rate after curative treatment remains high (70%),with 15% of HCC patients developing extrahepatic metastasis[3].One important reason is that tumor cells are able to penetrate the microvasculature,disseminate through the bloodstream to other sites,and form metastatic tumors.Studies have suggested that microvascular invasion (MVI) in HCC is one of the most significant risk factors for recurrence and metastasis in HCC following curative surgical resection[4].MVI is defined as clusters of cancer cells observed microscopically in vessels located in the tumor capsule and surrounding liver parenchyma[5].Previous research reported that the incidence of MVI ranged from 15% to 57% in HCC specimens and was associated with tumor size,levels of alpha fetoprotein (AFP),and typical image features[6].Even for patients with HCC,the presence of MVI increases the risk of recurrence and dramatically shortens long-term survival[7,8].The main reason for this is that the residual microthrombosis results in early recurrence.A safe surgical margin is a prerequisite for the complete removal of residual microtumor thrombosis.In HCC,invasion of the portal vein and intrahepatic and distant metastases are frequently observed.Resection of the portal vein invaded by the tumor is one method to decrease the risk of recurrence.Previous research has reported that both anatomic resection (AR) and non-anatomic resection (NAR),with a sufficient margin,can reduce the risk of early recurrence and improve the prognosis of HCC[9,10].A meta-analysis has shown that anatomical hepatectomy is more effective than non-anatomical hepatectomy[11].We defined AR as the complete removal of at least one Couinaud segment containing the focus and the portal vein in the drainage area of the lesion.A complete tumor plus the rim of non-neoplastic liver parenchyma was considered a non-anatomic resection[12].Studies have shown that although the width of the resection margin does not influence the postoperative recurrence rates after liver resection,a wide margin is associated with a lower recurrence risk in patients with venous invasion or microsatellites[12,13].Studies have shown that not all patients are suitable for AR,and controversy remains over the superiority of AR compared to NAR.In general,AR guarantees a wider surgical margin.However,a wider surgical margin means that more healthy liver tissue has to be removed.Almost all patients with HCC have liver cirrhosis,and the excessive removal of non-neoplastic liver parenchyma can lead to liver dysfunction and the morbidities of ascites,jaundice,and hypoalbuminemia.When the tumor is enormous and the remaining liver tissue is insufficient,AR may not be appropriate[14].When the liver volume is insufficient,a surgical margin of at least 5 mm should be secured by NAR whenever possible[15].Therefore,NAR still plays an important role in hepatectomy.Previous studies have shown that AR should be performed when the size of HCC ranges from 2 to 5 cm[10].However,whether AR should be recommended when the diameter is less than 2 cm or greater than 5 cm remains controversial.In addition,whether anatomical hepatectomy improves the prognosis of patients with hepatocellular carcinoma with microvascular invasion regardless of tumor size is unclear.Therefore,the aim of the study is to determine whether AR improves long-term survival in patients with hepatocellular carcinoma (HCC) by removing microvascular invasion (MVI).
MATERIALS AND METHODS
Patient selection
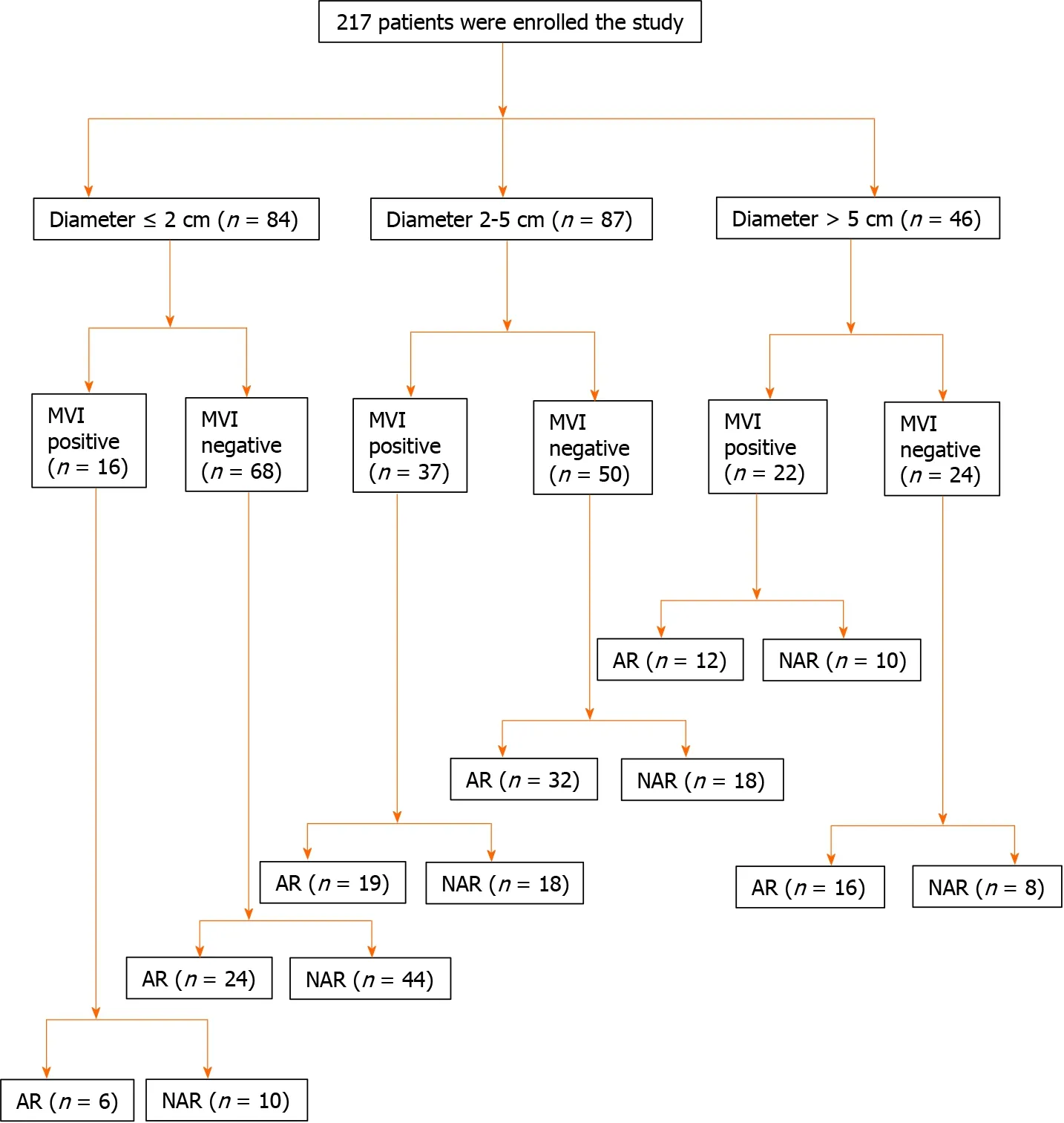
Figure 1 Flow diagram for the study.
Patient eligibility
The inclusion criteria were:(1) Definitive pathological diagnosis of HCC based on the World Health Organization criteria;(2) Curative resection,defined as complete macroscopic removal of the tumor with negative (R0) margins;(3) No prior anticancer treatment;and (4) Aged between 18 and 80 years.The exclusion criteria were:(1)Distant metastasis;(2) Portal vein tumor thrombosis (PVTT);and (3) Child-Pugh C liver disease.The study was conducted in accordance with the Declaration of Helsinki(as revised in 2013).The study was approved by the Ethical Committee of Tongji Hospital of Tongji Medical College of Huazhong University of Science and Technology,and the number of the approval was TJ-IRB20181101.Informed consent was obtained from each patient included in the study.
Terminology
Completely removing at least one Couinaud segment containing the focus and portal vein in the drainage area of the lesion was defined as an AR.A complete tumor plus a rim of non-neoplastic liver parenchyma was considered an NAR.
Surgical procedure
All surgeries were accomplished by a team who was able to professionally implement a hepatectomy.Patients were placed in supine position and under general anesthesia.The surgical principles were followed according to the corresponding the Union for International Cancer Control TNM classification.Intraoperative ultrasonography was routinely used in all patients to assess the number and size of the tumors,and their relation to nearby vascular structures.Proper hepatic vascular control techniques,including the selective inflow occlusion (SIO) maneuver and intermittent Pringle maneuvers (IPs),were used to reduce bleeding during liver resection.The SIO maneuver is described by the following procedure:dissecting the portal vein,proper hepatic artery,right and left hepatic arteries,and bile ducts followed by continuously blocking the hepatic artery in the tumor bearing lobe with a bulldog clamp.IPs encircling the hepatoduodenal ligament were performed with cycles of clamping and unclamping times of 15 min and 5 min,respectively.
Follow-up and tumor recurrence
The patients were surveilled every 1 mo with ultrasonography and AFP during the first 6 mo after surgery and every 3 mo thereafter.Patients were scheduled to have a computerized tomography (CT) scan every 6 mo and a magnetic resonance imaging(MRI) every year.Recurrence was diagnosed by computed tomography scans,magnetic resonance imaging,digital subtraction angiography,and elevated serum AFP level.We reviewed the governmental death registration and performed telephone follow-ups.Patients were excluded if they were not followed up as required,or their governmental data were incomplete.Follow-up was terminated on May 31,2021.Patients lost to follow-up and with missing data were prematurely excluded.Ultimately,217 eligible patients were enrolled in the study.Death was the primary endpoint and the diagnosis of intrahepatic recurrence and/or extrahepatic metastasis was the secondary endpoint.
Study design
First,all patients were randomized to receive standard anatomic or non-anatomic resection.After surgery,we measured the surgical margin and identified microvascular invasion.We divided them into three groups based on tumor size to compare the effects of anatomic and nonanatomic hepatectomy in subgroups.In addition,the relationship between tumor size and surgical margin was further analyzed.
Statistical analysis
Data are presented as the mean ± SD.The overall survival (OS) was analyzed using Kaplan-Meier survival curves and a log-rank test.Student’st-tests were used for comparison between groups where appropriate.Aχ2test was used for comparison between groups where appropriate.P<0.05 was considered statistically significant.Statistical analyses were performed with SPSS version 19.0.
RESULTS
Patient characteristics
The mean follow-up time was 45.2 ± 6.3 mo (median:46.0 mo;range:30.6-53.4 mo).The cumulative survival rate for all patients was 90%,57%,and 39% at 1,3,and 5 years.All of the category boundaries were defined by the clinical guideline or recognized criterion when continuous variables were categorized.Table 1 demonstrates the clinical and tumor characteristics of the 217 patients with HCC.The mean patient age was 52.6 ± 12.4 years (range:21-74 years).The patients were 90.8%(197/217) male and 9.2% (20/217) female.In total,86.6% (178/217) were positive for hepatitis B virus (HBV) infection and 10 patients were positive for the hepatitis C virus(HCV).Overall,42.4% (92/217) were Barcelona Clinic Liver Cancer (BCLC) 0+A,and 34.6% (75/217) were MVI positive.Eight patients (3.7%) had a hepatic function of Child-Pugh score B and received short-term liver protective therapy before surgery.The clinical and pathological characteristics of the AR and NAR groups are summarized in Table 2.There were no significant differences in age,sex,Child-Pugh class,etc.between the two groups.
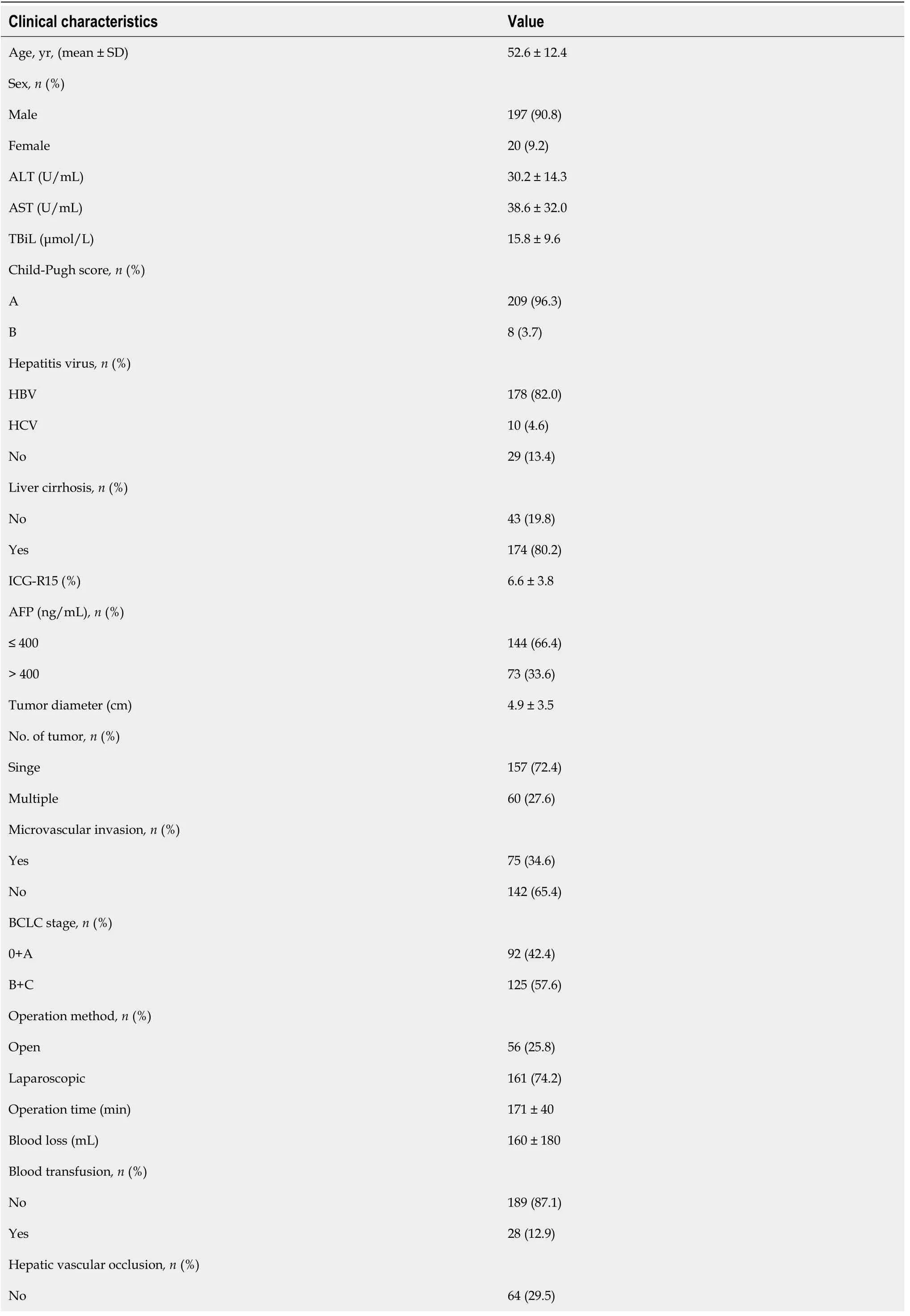
Table 1 Clinical characteristics of 217 patients

AFP:Alpha fetoprotein;ALT:Alanine transaminase;AST:Aspartate aminotransferase;BCLC:Barcelona Clinic Liver Cancer staging system;HBV:Hepatitis B virus;HCV:Hepatitis C virus;ICG R15 (%):Indocyanine green retention rate at 15 min;SD:Standard deviation;TBiL:Total bilirubin.

Table 2 Clinical characteristics of anatomic resection and non-anatomic resection

AFP:Alpha fetoprotein;ALT:Alanine transaminase;AST:Aspartate aminotransferase;AR:Anatomic resection;BCLC:Barcelona Clinic Liver Cancer staging system;HBsAg:Hepatitis B surface antigen;ICG R15 (%):Indocyanine green retention rate at 15 min;NAR:Non-anatomic resection;TBiL:Total bilirubin.
Comparison of types of hepatectomy with prognosis in the 2-5 cm tumor diameter subgroup
The 217 included patients were divided into three groups:diameter ≤ 2 cm (84/217),2-5 cm (87/217) and > 5 cm (46/217).In the diameter 2-5 cm group,there was a statistically significant difference between MVI positive and MVI negative patients (median OS 32.0 mo,95% confidence interval (CI):13.3-50.8 movsnot reached,P=0.031)(Figure 2A).For the MVI positive patients,there was a statistically significant difference between AR and NAR (median OS not reachedvs29.0 mo 95%CI:8.0-43.9 mo,P=0.027) (Figure 2B).However,for the MVI negative patients,there were no statistically significant differences between those who underwent AR and NAR(median OS not reachedvs44.2 mo,95%CI:27.0-61.5 mo,P=0.206) (Figure 2C).This suggests that AR improved OS only in MVI positive patients,but not in MVI negative patients in the diameter 2-5 cm group.In addition,we compared the surgical margin of AR and NAR in the 2-5 cm diameter group.We found that AR led to a wider surgical margin than NAR (2.0 ± 2.3 cmvs0.7 ± 0.5 cm,P<0.001) (Table 3).We speculated that AR can achieve a wide enough surgical margin,which can remove MVI in advance,reducing the risk of postoperative recurrence and improving the prognosis.
15.Ball:A ball is a large party in which the participants dress up in their finest clothes and dance. Balls were exclusively for the privileged and wealthy.
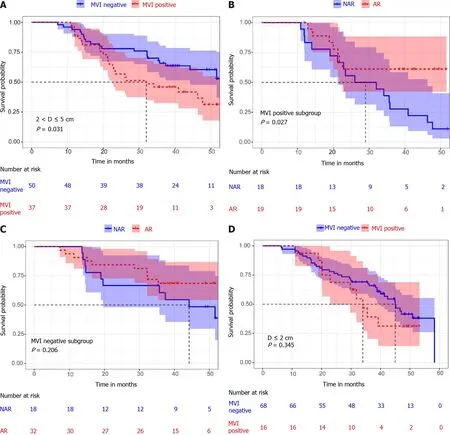
Figure 2 The long-term outcome of hepatocellular carcinoma with different tumor diameters.
Comparison of types of hepatectomy with prognosis in the subgroup with a tumor diameter less than 2 cm
Among patients with a diameter less than 2 cm,there was no statistically significant difference between MVI positive and MVI negative patients (median OS 34 mo 95%CI:27.6-40.4 movs45.0 mo 95%CI:39.4-50.6 mo,P=0.345) (Figure 2D).In addition,there was no statistically significant difference in overall survival between patients who received AR and NAR,whether MVI positive or MVI negative (median OS 32.4 mo 95%CI:13.0-46.3 movsnot reached,P=0.097;median OS 46.6 mo,95%CI:32.8-60.4 movs41.3 mo,95%CI:34.6-48.1 mo,P=0.869) (Figure 3A and B).By comparing the surgical margins of AR and NAR patients,we found that although the AR margins were wider than those of NAR patients,the margins of both were greater than 1 cm(3.5 ± 5.8 cmvs1.6 ± 0.5 cm,P=0.048) (Table 3;Figure 4B).If a surgical margin of 1 cm is ensured,it can be clinically regarded as a R0 resection.Thus,for patients with a tumor of less than 2 cm in diameter,both AR and NAR can achieve a wide surgical margin to ensure the removal of MVI.
Comparison of types of hepatectomy with prognosis in the subgroup with a tumor diameter larger than 5 cm
In the group with a diameter > 5 cm,the prognosis of MVI positive patients was significantly worse than that of MVI negative patients (median OS 24.0 mo,95%CI:15.7-32.4 movsnot reached,P=0.004) (Figure 3C).However,there was no statistically significant difference in overall survival between patients who received AR and NAR,whether MVI positive or MVI negative,(median OS 27.2 mo,95%CI:21.9-32.5 movs20.1 mo,95%CI:5.6-28.8 mo,P=0.428;median OS not reachedvs38.3 mo,95%CI:19.5-60.5 mo,P=0.714) (Figures 3D and 4A).In addition,there were no statistically significant differences between AR and NAR in surgical margins and the margins of both were less than 1 cm (0.6 ± 1.0 cmvs0.7 ± 0.4 cm,P=0.491) (Table 3;Figure 4B).For patients with tumors larger than 5 cm in diameter,neither AR nor NAR could obtain a wide enough surgical margin to ensure the removal of MVI.
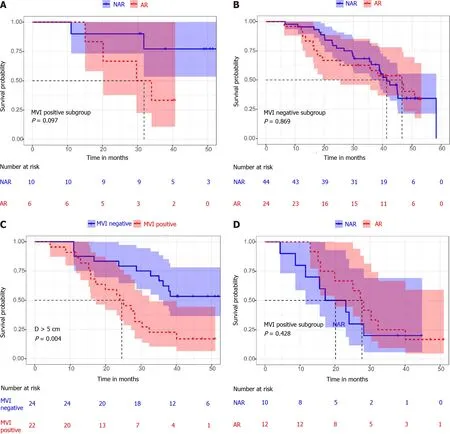
Figure 3 The long-term outcome of hepatocellular carcinoma with different tumor diameter.
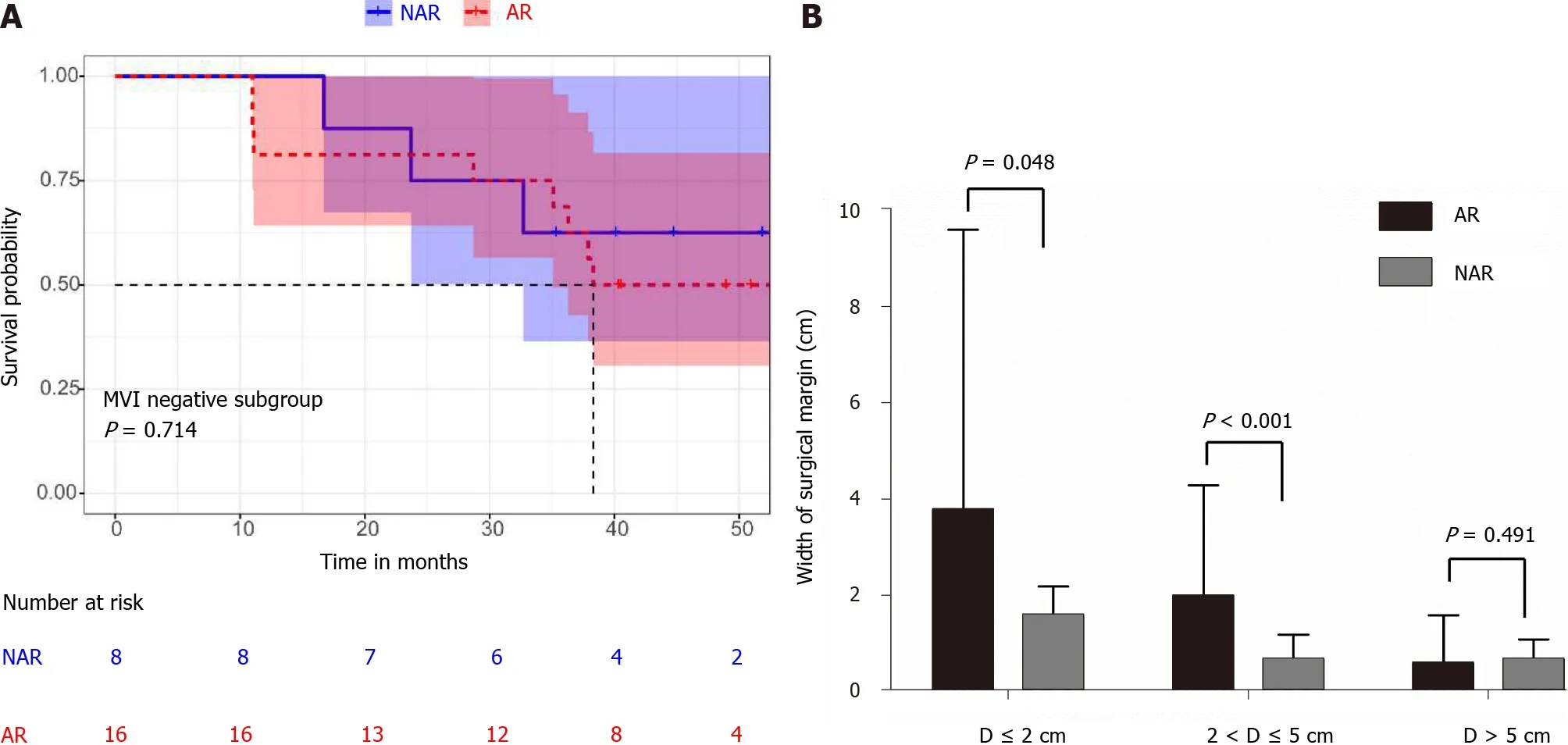
Figure 4 Kaplan-Meier analysis of the overall survival (A) and comparison of surgical margins in patients with different tumor diameters(B).

Table 3 The surgical margin of different tumor diameter groups
DISCUSSION
At present,surgeons consider hepatectomy and liver transplantation the optimal therapies to improve prognosis in HCC;however,tumor recurrence is still an important cause of death in patients[16].Previous research has demonstrated that microvascular invasion is a vital risk factor for the prognosis of HCC patients after curative hepatectomy[17].As long as a surgical margin of 1 cm is ensured,it can be clinically regarded as an R0 resection[18].The margin of microvascular invasion is generally no more than 1 cm.Therefore,an R0 resection enables the complete removal of the liver tissue invaded by the microvascular thrombosis.In contrast,positive margins were associated with a worse prognosis[19,20].Previous studies have shown that a wider surgical margin has been associated with a better prognosis among patients with HCC[21-23].In addition,a previous study has shown that AR led to a better OS than NAR.In a multivariable analysis,an AR was one of the prognostic factors[9].AR can reduce the risk of tumor residues and recurrence due to the elimination of venous tumor thrombosis within the resected domain,when at least one complete Couinaud segment and the portal vein in the drainage area of the lesion are removed[24,25].However,almost all patients with HCC have liver cirrhosis and excessive removal of non-neoplastic liver parenchyma can lead to liver dysfunction and the morbidities of ascites,jaundice,and hypoalbuminemia.
Our data indicated that AR improved OS only in MVI positive patients,but not in MVI negative patients in the 2-5 cm diameter group.We speculated that AR can achieve a wide enough surgical margin,which can remove MVI in advance,reduce the risk of postoperative recurrence,and improve the prognosis.For patients with a tumor diameter of less than 2 cm,both AR and NAR can obtain a wide surgical margin to ensure removal of MVI.Therefore,patients with a diameter less than 2 cm,both AR and NAR,can achieve a good prognosis.In other words,an R0 resection enabled the removal of the liver tissue invaded by the MVI regardless of whether AR or NAR was chosen by the surgeon.This suggests that AR is not necessary for tumors with a diameter of less than 2 cm,as long as sufficient surgical margin is ensured.However,in the > 5 cm group,both AR and NAR cannot guarantee sufficient surgical margin,which is one of the reasons why tumors with a diameter of more than 5 cm have a worse prognosis than tumors with a diameter of less than 2 cm.We believe that the surgeon needs to consider whether the residual liver volume and liver function reserve are sufficient when faced with a very large tumor.Therefore,for tumor diameters larger than 5 cm,the width of the resection margin should be increased appropriately when a sufficient liver volume and a good liver function can be ensured.
Limitations
The limitations of this study are the relatively small samples,short follow-up time,and a single study center cohort study.A multicenter clinical trial should be designed to further validate the prognostic significance of types of hepatectomy in HCC.
CONCLUSION
For patients with a tumor diameter of 2-5 cm,AR can achieve the removal of peritumoral MVI by obtaining a wide incision margin,reduce postoperative recurrence,and improve prognosis.
ARTICLE HIGHLIGHTS
Research background
At present,most studies suggest that anatomical resection is more effective than nonanatomical resection in the tumor diameter ranging from 2 cm to 5 cm.However,for tumors smaller than 2 cm and larger than 5 cm in diameter,the advantage of anatomic hepatectomy is not significant.Why is that? Does anatomic resection (AR) have an advantage over non-anatomic resection (NAR) in hepatocellular carcinoma (HCC)patients with microvascular invasion (MVI)?
Research motivation
Our study aimed to determine the effects of AR and NAR in different tumor diameter stratification.Further analysis shows that AR improves patient outcomes by obtaining a wider surgical margin.
Research objectives
This study compared the efficacy of AR and NAR in different tumor diameter subgroups in a prospective cohort study.
Research methods
First,all patients were randomized to receive standard anatomic or non-anatomic resection.After surgery,we measured the surgical margin and identified microvascular invasion.We divided them into three groups based on tumor size.
Research results
When the tumor is enormous and the remaining liver tissue is insufficient,AR may not be appropriate.For patients with a tumor diameter of 2-5 cm,AR can achieve the removal of peritumoral MVI by obtaining a wide incision margin,reducing postoperative recurrence and improving prognosis.For patients with a tumor of less than 2 cm in diameter,both AR and NAR can obtain a wide surgical margin to ensure the removal of MVI.AR should not be recommended for those patients.For patients with tumors larger than 5 cm in diameter,neither AR nor NAR could obtain a wide surgical margin to ensure removal of MVI.
Research conclusions
The doctor should ensure sufficient surgical margin on the premise of ensuring the safety of the operation.Therefore,for patients with a tumor diameter of 2-5 cm,AR should be strongly recommended.
Research perspectives
The study could guide doctors in their choice of surgical procedures.In general,AR guarantees a wider surgical margin.However,a wider surgical margin means that more healthy liver tissue has to be removed.Almost all patients with HCC have liver cirrhosis,and the excessive removal of non-neoplastic liver parenchyma can lead to liver dysfunction and the morbidities of ascites,jaundice,and hypoalbuminemia.When the tumor is enormous and the remaining liver tissue is insufficient,AR may not be appropriate.
ACKNOWLEDGEMENTS
The authors would like to thank Dr.Chang Shu who is a of statistics (Translational Medicine Center,Tongji Hospital,Tongji Medical College,Huazhong University of Science and Technology) for her technical assistance of statistical analysis.
 World Journal of Gastrointestinal Oncology2021年12期
World Journal of Gastrointestinal Oncology2021年12期
- World Journal of Gastrointestinal Oncology的其它文章
- Management of obstructive colon cancer:Current status,obstacles,and future directions
- Role of endoscopic ultrasound in anticancer therapy:Current evidence and future perspectives
- Mesenchymal stem cell-derived exosomes for gastrointestinal cancer
- Gender differences in the relationship between alcohol consumption and gastric cancer risk are uncertain and not well-delineated
- Pancreatic intraductal papillary mucinous neoplasms:Current diagnosis and management
- Combined treatments in hepatocellular carcinoma:Time to put them in the guidelines?