
Current status of first-line therapy,anti-angiogenic therapy and its combinations of other agents for unresectable hepatocellular carcinoma
2022-01-10 07:58SalehAlqahtaniMassimoColombo
Saleh A Alqahtani,Massimo G Colombo
Saleh A Alqahtani,Division of Gastroenterology and Hepatology,Johns Hopkins University,Baltimore,MD 21287,United States
Saleh A Alqahtani,Liver Transplant Center,and Biostatistics,Epidemiology,and Scientific Computing Department,King Faisal Specialist Hospital &Research Center,Riyadh 11564,Saudi Arabia
Massimo G Colombo,Liver Center,IRCCS San Raffaele Hospital,Milan 20132,Italy
Abstract Globally,hepatocellular carcinoma (HCC) is a frequently diagnosed malignancy with rapidly increasing incidence and mortality rates.Unfortunately,many of these patients are diagnosed in the advanced stages when locoregional treatments are not appropriate.Before 2008,no effective drug treatments existed to prolong survival,until the breakthrough multi-tyrosine kinase inhibitor (TKI) sorafenib was developed.It remained the standard treatment option for advanced HCC for 10 years,with a battery of other candidate drugs in clinical trials failing to produce similar efficacy results.In 2018,the REFLECT trial introduced another multi-TKI,lenvatinib,which has non-inferior overall survival compared with sorafenib.Thus,offering patients and their treating physicians two effective treatment options.Recently,immunotherapy-based drugs,such as atezolizumab and bevacizumab,have shown promising results in patients with unresectable HCC.This review summarizes clinical trial and real-world data studies of sorafenib and lenvatinib in patients with unresectable HCC.We offer guidance on the optimal choice between the two treatments and discuss the potential of immunotherapy-based combination;when more data become available,this will likely make the choice between sorafenib and lenvatinib somewhat obsolete.
Key Words:Hepatocellular carcinoma;Immune checkpoint inhibitor;Lenvatinib;Multityrosine kinase inhibitor;Sorafenib
INTRODUCTION
Currently,liver cancer ranks as the seventh most common cancer type in the world,being the fourth most common cause of cancer-related death[1].The vast majority of these liver cancers (approximately 80%) arise from hepatocytes and are referred to as hepatocellular carcinoma (HCC)[2].Over the last decades,the global incidence of HCC has been increasing,with a 75% incidence increase of newly diagnosed HCC cases from 1990 to 2015[3].Risk factors for developing HCC consist of viral hepatitis,extreme alcohol intake,and non-alcoholic fatty liver disease (NAFLD)[2].Furthermore,obesity increases the risk of developing NAFLD,and given the ever-increasing obesity epidemic in many parts of the world,the significance of NAFLD-related HCC is predicted to have profound effects in the coming years[4].
For patients with initial-stage HCC,curative therapy strategies,such as liver resection,liver transplantation,or radiofrequency ablation,can still provide long-term survival[2,5].However,many HCC patients receive their diagnosis at progressive stages of the disease when locoregional treatment is no longer an option.When not treated,patients with advanced-stage HCC have a very poor prognosis,with a median overall survival (OS) of 9 mo and a 6-mo OS of 56.6%[6].Until 2008,not a single effective systemic treatment option was available for these patients,an unparalleled situation in oncology.In fact,advanced HCC proved to be notoriously difficult to treat.HCC is not only a very chemo-resistant tumor type,but the constant threat of declining liver function often compromises an effective treatment.Over the last decades,improved insights into the molecular processes that initiate and promote the tumor progression in HCC have facilitated the development of novel molecular treatment modalities that specifically target these disrupted molecular pathways.
In 2008,the multi-tyrosine kinase inhibitor (TKI) sorafenib became the first effective systemic therapy for patients with advanced HCC with a preserved liver function[7].Following its successful introduction into the treatment paradigm for advanced HCC,several other targeted drugs were tested in this setting.Unfortunately,this resulted in a decade of disappointing phase III randomized controlled trials (RCTs).Until 2017,the oral multi-TKI regorafenib reported increased survival rates in patients who received sorafenib[8].Shortly thereafter,the multi-TKIs cabozantinib and ramucirumab were also shown to delay the disease progression and prolong the OS of HCC patients progressing on sorafenib [for ramucirumab,this benefit was limited to patients with an increased alpha-fetoprotein (AFP) concentration][9,10].However,until very recently,not a single clinical trial was able to demonstrate a survival benefit compared to sorafenib in the first-line treatment for patients with progressive HCC.Finally,in 2018,the multi-TKI lenvatinib emerged as a feasible first-line alternative for sorafenib in these patients.In fact,results of the phase III REFLECT trial established that the multi-TKI lenvatinib was non-inferior to sorafenib as a first-line treatment for patients with advanced HCC[11].Thus,physicians now have a choice between two equally effective multi-TKIs in the first-line treatment of these patients.In this article,we review the clinical trial data and real-world data generated with sorafenib and lenvatinib,with a particular focus on the differences between both agents that can be used to steer the treatment choice in an individual patient.
In recent years,the growing interest in immune checkpoint inhibition as a new pillar of the cancer treatment paradigm has also spurred the evaluation of these drugs in patients with unresectable HCC.Clinical trials using these immune checkpoint inhibitors (ICIs) in monotherapy demonstrate only a moderate clinical benefit[12,13].In contrast,RCTs evaluating combinations of a TKI and an ICI have generated more convincing results.In fact,results of the phase III IMbrave150 trial recently highlighted that atezolizumab plus bevacizumab had a significantly prolonged OS compared to sorafenib in the first-line treatment of patients with advanced HCC[14].Furthermore,new data are emerging for other first-line ICI-TKI combinations (e.g.,pembrolizumablenvatinib).This review summarizes the results obtained from clinical trials and realworld studies of sorafenib and lenvatinib in patients with unresectable HCC.We offer guidance on the optimal choice between sorafenib or lenvatinib in an individual patient and discuss the potential of immunotherapy-based combinations,which,with more data,will likely make a choice between sorafenib and lenvatinib somewhat obsolete.
SORAFENIB:THE LONG-STANDING STANDARD
Clinical trial data
Sorafenib is an oral multi-TKI that checks and arrests several tyrosine kinases involved in tumor angiogenesis,progression,and apoptosis.It inhibits both vascular endothelial growth factor receptor and platelet-derived growth factor receptor and also targets fms-like tyrosine kinase 3,c-Kit,and several kinases involved in the mitogen activated protein kinase signaling pathway[15].The application of sorafenib as the standard treatment choice in the first-line therapeutic management of patients with advanced HCC was based on the results of two pivotal phase III RCTs.
In the phase III SHARP trial,602 (mainly European) patients with advanced HCC,who did not receive prior systemic treatment,were randomly assigned to receive either sorafenib (400 mg twice daily) or placebo.In order to be eligible for the trial,patients had to have an Eastern Cooperative Oncology Group performance status of ≥2 and have a preserved liver function (Child-Pugh class A)[7].The median age of patients in the trial was 65 years,more than 80% had Barcelona Clinic Liver Cancer(BCLC) stage C disease,and the vast majority (97%) were rated as Child-Pugh A at baseline.The study reached its primary endpoint by proving a significant OS benefit for sorafenib compared to placebo,with a median OS of 10.7 and 7.9 mo,respectively[hazard ratio (HR) 0.69;95% confidence interval (CI):0.55-0.87;P<0.001].Also,in terms of the time to radiological progression,sorafenib outperformed the placebo(median:5.5 movs2.8 mo;HR 0.58;95%CI:0.45-0.74;P<0.001).Objective response rates (ORR) were rare in both arms of the study,with only 2% partial responses with sorafenib compared to 1% with placebo (no complete responses were reported).However,looking at the disease control rate (DCR),a significant benefit was seen for sorafenib compared to placebo (43%vs32%;P=0.002)[7].In the SHARP trial,the incidence of treatment-related adverse events (TRAEs) was reported at 80% with sorafenib compared to 52% with placebo.The most common grade 3/4 TRAEs of sorafenib were diarrhea (8% with sorafenibvs2% with placebo;P<0.001) and handfoot skin reactions (8%vs1%;P<0.001).Despite the relatively low rate of high-grade TRAEs,the rate of therapy discontinuations due to adverse events (AEs) was high at 38%.
The second pivotal trial with sorafenib in patients with progressive HCC was conducted in the Asia-Pacific region and yielded fairly similar results[16].In that trial,a total of 226 advanced HCC patients with a Child-Pugh A liver score were randomly assigned (2:1) to receive either sorafenib (400 mg twice daily) or placebo.Sorafenib also showed a significantly prolonged OS compared to placebo,with a median OS of 6.5 and 4.2 mo for sorafenib and placebo,respectively (HR 0.68;95%CI:0.50-0.93;P=0.014).In addition to this,patients who received sorafenib had a significantly longer time to progression (TTP) compared to patients treated with placebo (median 2.8 movs1.4 mo;HR 0.57;95%CI:0.42-0.79;P=0.0005)[16].
Real-world experience
In the years following the registration of sorafenib for patients with advanced HCC,several studies were set up to evaluate the performance of sorafenib in a real-world setting.In the Italian SOFIA study,269 advanced HCC patients were treated with sorafenib (400 mg twice daily),resulting in a median OS of 10.5 mo (8.4 mo for patients with BCLC-C disease and 20.6 mo for BCLC-B patients)[17].The most common grade 3/4 AEs reported in SOFIA were fatigue (25%),hand-foot skin reactions (9%),hypertension (7%),and diarrhea (6%).Similar to what was reported in SHARP,40% of patients treated with sorafenib in the SOFIA study had to discontinue therapy due to an AE[17].
The prospective,non-interventional INSIGHT trial also evaluated the safety and efficacy of sorafenib in real-world clinical practice.In this study,including a safety set of 788 HCC patients,the rate of TRAE discontinuations was much lower than in SHARP and SOFIA,as only 15.5% of patients discontinued their therapy because of unacceptable toxicity[18].A possible explanation for this lower rate could be the fact that this study was reported a decade after the introduction of sorafenib.Thus,it is likely that the increased experience of physicians with this agent and the increased knowledge on how to deal with its toxicity profile ultimately resulted in this lower rate of TRAE discontinuation.
Similarly,a large retrospective study from the United States reported lower rates of TRAE discontinuations with sorafenib than those reported in SHARP.In that study,published in 2017,a total of 3094 advanced HCC patients received sorafenib at the normal dose of 800 mgperday.Of them,only 22.4% had to discontinue their therapy for reasons of toxicity[19].In an attempt to reduce further the TRAE drop-out,the possibility of introducing sorafenib at a lower dose (<800 mg/d) was explored,resulting in a decreased pill burden that was less expensive.In addition to this,there were fewer treatment discontinuations due to safety/toxicity concerns (19.6%).With the standard dosing,the median OS reported in this cohort was 233 d (approximately 7-8 mo),which is in line with the SHARP trial[7,19].Among patients who received a reduced dose of sorafenib,the median OS was shorter at 200 d.However,given the fact that patients who received the reduced dose were generally sicker than patients who were deemed to be eligible for the full dose,this comes as no surprise.When compensating for the differences in patient and disease characteristics between patients in the full and reduced dose cohort (propensity score-matched analysis),no difference in OS was found (HR 0.92;95%CI:0.83-1.01)[19].
Among the patients enrolled in these RCTs,many of them had a stable hepatic function with reference to Child-Pugh A disease (SHARP:95% and Asia-Pacific study:97%).However,in real-world settings,there are patients with hepatic dysfunction(Child-Pugh B or C),and for these,the RCTs do not provide a clear answer on the potential benefit of sorafenib.In this respect,real-world data can provide guidance to physicians.Not surprisingly,results of a French case-control study (n=120) indicate that advanced HCC patients with a Child-Pugh A status have a better OS when they are treated with sorafenib than patients who have more advanced liver damage(Child-Pugh B),with a median OS of 13 and 4.5 mo,respectively (P=0.0008)[20].A similar observation was seen in the INSIGHT trial,where the median OS with sorafenib was reported as 17.6 mo for patients with a Child-Pugh A status,decreasing to 8.1 and 5.6 mo for patients with Child-Pugh B or C disease,respectively[18].Finally,the observational GIDEON registry showed that Child-Pugh A patients have a longer OS when treated with sorafenib than patients with Child-Pugh B disease (median OS:13.6 and 5.2 mo,respectively)[21].However,the fact that Child-Pugh B patients do worse on sorafenib than patients with a preserved liver function should not be a reason to reserve sorafenib for patients with Child-Pugh A disease alone.In fact,GIDEON also shows that the overall safety profile and dosing strategy of sorafenib are similar across the different Child-Pugh subgroups[21].In another prospective study by Lealet al[22],in a separate prospective score,specifically focusing on the use of sorafenib in Child-Pugh B patients,a median OS of 6.5 mo was reported,which was longer than historical controls for this population.In this study,sorafenib also proved to be tolerable,with a relatively low rate of TRAE discontinuations (27.7%)[22].As such,these results highlight that selected Child-Pugh B patients may also derive benefit from treatment with sorafenib,with a manageable toxicity profile.
Overall,a large body of real-world data convincingly validate sorafenib as a safe and effective therapy option for patients with advanced HCC and confirm the results obtained in the pivotal RCTs.Furthermore,real-world data have also indicated that given adequate patient selection,sorafenib can also be safe and effective in patients who do not meet the strict inclusion criteria of the SHARP and Asia-Pacific trial.
LENVATINIB:AT LEAST AS GOOD AS SORAFENIB
Since its introduction as a treatment option for patients with advanced HCC,sorafenib has been evaluated against several other targeted agents.However,sunitinib did not prove to be better than sorafenib,and two non-inferiority studies testing brivanib and linifanib against sorafenib turned out to be negative[23].In addition to this,the phase III SEARCH trial,assessing the potential benefit of adding erlotinib to sorafenib in the first-line treatment of patients with advanced HCC,also failed to show a benefit[24].In the background of these numerous negative studies,the positive outcome of the phase III REFLECT trial in 2018,showing non-inferiority of lenvatinib to sorafenib as a firstline treatment for patients with unresectable HCC,came somewhat as a surprise[11].
Clinical trial data
Similar to sorafenib,lenvatinib is a multi-TKI.It primarily inhibits the vascular endothelial growth factor receptor 1-3,fibroblast growth factor receptor 1-4,KIT,and RET (Figure 1)[25].In a single-arm phase II trial,including 46 patients with advanced HCC,lenvatinib at a fixed dose of 12 mg/d was found to have substantial clinical activity.With this regimen,a median OS of 18.7 mo was reported,with 37% of patients obtaining a partial response.However,this came at the cost of considerable toxicity,necessitating a dose reduction and treatment discontinuation in 74% and 22% of patients,respectively[26].Further in-depth analyses of this trial revealed a close correlation between lenvatinib treatment discontinuation and body weight.Based on this finding,the investigators opted to use a weight-adapted lenvatinib dosing in the subsequent phase III trial.
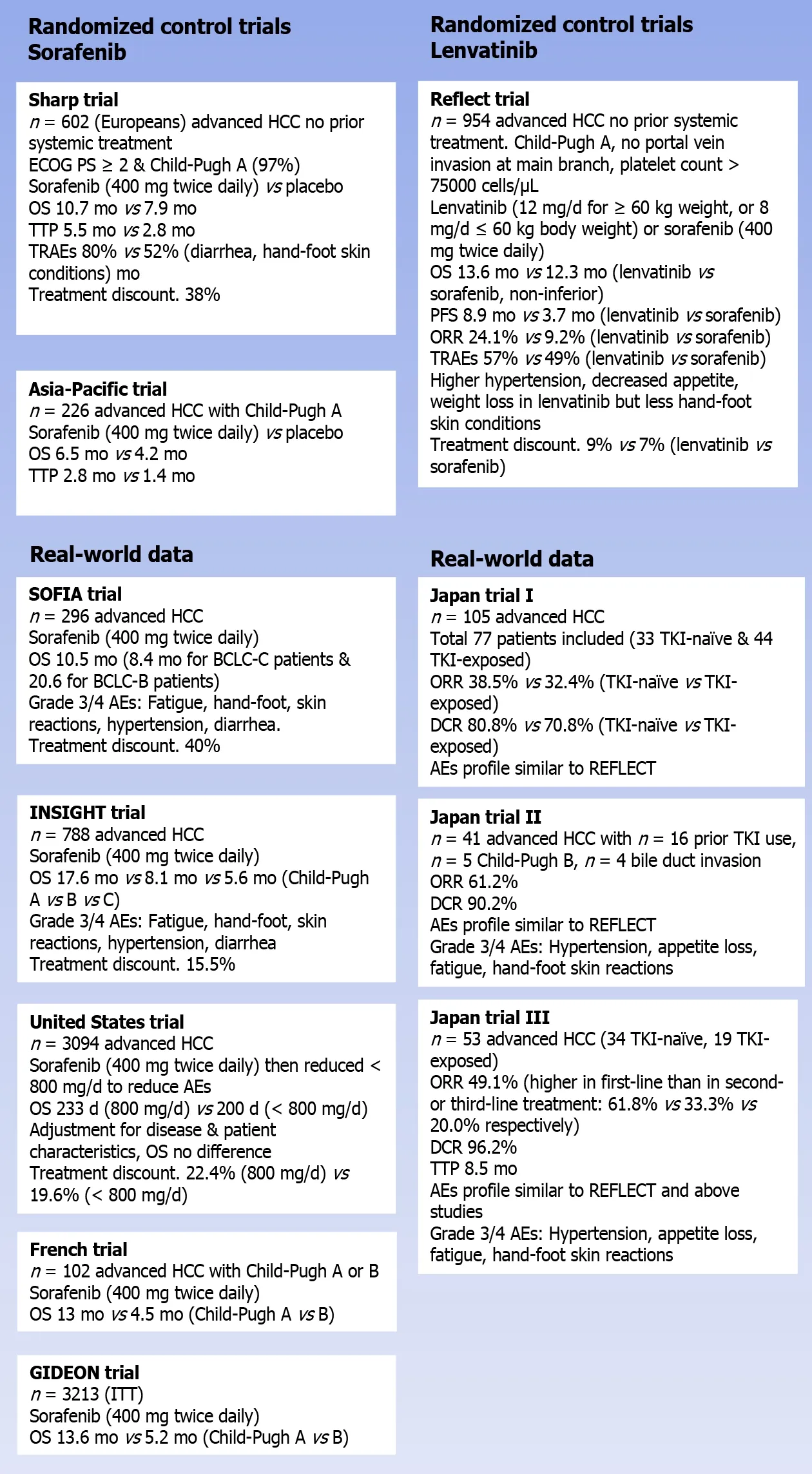
Figure 1 Evolution of clinical trials and real-world data for sorafenib and lenvatinib.
In the randomized phase III REFLECT trial,a total of 954 patients who did not receive treatment for unresectable HCC were randomly assigned (1:1) to receive either lenvatinib (12 mg/d for patients weighing ≥ 60 kg;8 mg/d for patients weighing<60 kg) or sorafenib (400 mg twice daily).In order to be eligible for the study,patients had to have a Child-Pugh A liver status and were not allowed to have portal vein invasion at the main portal branch.In addition,patients with a platelet count below 75000 cells/μL were excluded.The study’s primary outcome was to demonstrate noninferiority for lenvatinib compared to sorafenib regarding the OS,with a noninferiority margin of 1.08.The median age of the patients enrolled in REFLECT was 62 years;69% had a body weight of ≥ 60 kg,and two-thirds came from Asia-Pacific regions.Extrahepatic spread at baseline was seen in 61% of the patients,while 21%exhibited macroscopic portal vein invasion (macroscopic portal vein invasion and/or extrahepatic spread in 70%).The majority of patients (79%) were classified as having BCLC stage C disease,and 57% had more than one involved disease site.Most of the patient and disease characteristics were well-proportioned between both arms,with some important exceptions.In fact,the number of patients with a hepatitis C etiology was higher in the sorafenib arm than in patients treated with lenvatinib (19%vs26%for lenvatinib and sorafenib,respectively),while the opposite was true for the proportion of hepatitis B-related HCC (53%vs48%).Finally,a marked imbalance was seen in the number of patients with an AFP level of ≥ 200 ng/mL (46%vs39%)[11].
The median OS for patients treated with lenvatinib in the REFLECT trial was reported at 13.6 mo,which was shown to be non-inferior to the 12.3 median OS seen in patients who received sorafenib (HR 0.92;95%CI:0.79-1.06).Besides,lenvatinib induced a significant progression-free survival (PFS) than sorafenib.In fact,compared to sorafenib,the median PFS for patients treated with lenvatinib was more than twice as long as the median PFS obtained with sorafenib (7.4vs.3.7 mo;HR 0.66;95%CI:0.57-0.77;P<0.0001).Importantly,lenvatinib was also shown to be associated with a significantly increased rate of ORR compared to sorafenib.With lenvatinib,an ORR of 24.1% was reported,while only 9.2% of sorafenib-treated patients obtained a partial or complete response (odds ratio;OR 3.13;95%CI:2.15-4.56;P<0.0001) (Table 1)[11].
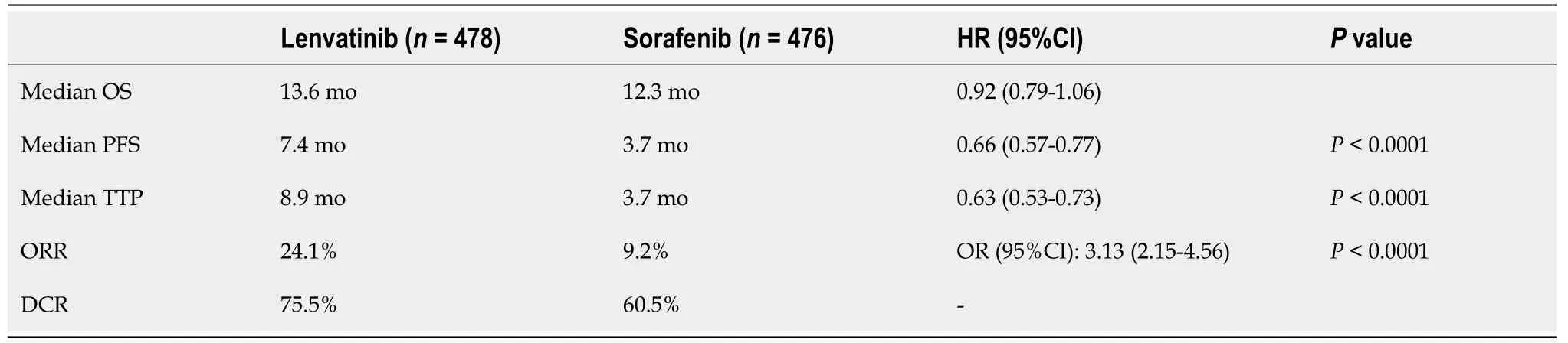
Table 1 Efficacy outcomes in the phase III REFLECT trial[11]
With respect to safety,lenvatinib was found to be associated with a slightly increased rate of grade ≥ 3 treatment-emergent AEs compared to sorafenib (57%vs49%).This difference was mainly fueled by a higher rate of grade ≥ 3 hypertension(23%vs14%) and an increased rate of grade ≥ 3 decreased appetite (5%vs1%) and grade ≥ 3 weight loss (8%vs3%) among patients treated with lenvatinib.In contrast,lenvatinib was associated with a substantially lower incidence of hand-foot skin reactions (all grade:27%vs52%;grade ≥ 3:3%vs11%)[11].The proportion of patients requiring a dose interruption (40%vs32%),dose reduction (37%vs38%),and treatment discontinuation (9%vs7%) was similar in the lenvatinib and sorafenib arms.
Real-world experience
Obviously,as lenvatinib only entered the HCC arena in 2018,the real-world evidence with this agent is more limited compared with sorafenib data.To date,the available real-world data with lenvatinib almost universally originate from Japan.
The largest real-world dataset for lenvatinib reported to date includes data from 105 unresectable HCC patients treated with lenvatinib across 48 clinics in Japan[27].After excluding patients who started lenvatinib at a reduced dose and with a short observation time,77 patients were eligible for a response (33 TKI-naïve,44 TKI-exposed).Both the ORR and the DCR at 4 wk did not differ significantly between TKI-naïve and TKI-pretreated patients (38.5%vs32.4% and 80.8%vs70.8%,respectively).The AE profile of lenvatinib seen in this study was largely in line with what was reported in REFLECT[27].
In a second study,a total of 41 patients with unresectable HCC were treated with lenvatinib.Interestingly,of these patients,23 (56%) would not have been eligible for the REFLECT trial,mainly because of a prior history of TKI use (n=16),a Child-Pugh B score (n=5),and the presence of bile duct invasion (n=4).In this cohort,lenvatinib was associated with an ORR of 61.0% and a DCR of 90.2%.Overall,5 patients (12.2%)experienced a complete response to lenvatinib.Interestingly,both the ORR and the DCR did not differ between patients who met the REFLECT criteria or not (P=0.83 and 0.79,respectively).In patients with a Child-Pugh B score,the ORR was 60% (3/5),while this was 100% in the 4 patients with bile duct invasion.With respect to safety,no major differences were seen between REFLECT eligible and ineligible patients,with a similar rate of grade ≥ 3 AEs.Lenvatinib in this cohort caused the following AEs most commonly:Hypertension (68.3%,grade ≥ 3 12.2%),appetite loss (68.3%;2.4%),fatigue(58.5%;0%),and hand-foot skin reactions (56.1%,14.6%).As such,these real-world data demonstrate that lenvatinib induces a high early response rate with good tolerability in advanced HCC patients who did and did not meet the REFLECT trial inclusion criteria[28].
A third Japanese real-world study yielded fairly similar results,in which 57 unresectable HCC patients were treated with lenvatinib,of whom 53 were eligible for response (34 TKI-naïve,19 TKI-exposed).In this cohort,lenvatinib therapy resulted in an ORR of 49.1% (26/53) and a DCR of 96.2% (51/53).Of note,the ORR was higher in patients receiving lenvatinib in first-line (61.8%) compared to patients receiving a second- (33.3%) or third-line (20.0%) treatment.The median TTP in the entire cohort was reported at 8.5 mo,and also for this endpoint,the outcome was better when lenvatinib was used as a first-line treatment.In addition,this real-world study revealed that patients with a better liver functional reserve had a higher response rate to lenvatinib and a longer TTP.Similar to REFLECT,the most common AEs with lenvatinib were hypertension (54.7%,grade ≥ 3:15.1%),fatigue (49.1%,7.5%),and a decreased appetite (37.7%,0%).Hand-foot skin reactions were reported in 26.4% of the patients (all grade 1/2)[29].
In a multi-center retrospective study,including 77 patients with advanced HCC,lenvatinib was associated with an ORR of 29.9% (similar to REFLECT) and a DCR of 77.9%.Interestingly,thyroid dysfunction and appetite loss were found to be associated with a worse and shorter PFS[30].In this respect,Hiraokaet al[31] also identified appetite loss as a dismal prognostic factor for advanced HCC patients treated with lenvatinib[31].As such,these AEs should be managed with care in patients treated with lenvatinib.
LENVATINIB OR SORAFENIB:HOW TO CHOOSE?
As illustrated above,robust RCT data and convincing real-world results have identified both sorafenib and lenvatinib as effective and safe first-line treatment options for patients with unresectable HCC.This brings us to a logical next question:How should physicians choose between both agents? When making such a decision,several patient and disease characteristics,including liver function and concomitant medication,need to be taken into account.In addition,financial implications need to be considered,especially given the ever-increasing pressure on healthcare budgets.
The phase III REFLECT trial showed non-inferiority of lenvatinib compared to sorafenib and even demonstrated a numerically longer median OS in lenvatinibtreated patients compared to patients treated with sorafenib (13.6 movs12.3 mo).This difference did not meet the statistical threshold to demonstrate superiority of lenvatinib compared to sorafenib.However,in a critical appraisal of REFLECT,as acknowledged by the authors,this lack of superiority might have been influenced by elements in the study design[32].First of all,both the baseline AFP level and the presence of macrovascular invasion were not used as a stratification factor for the randomization in REFLECT.As a result,a higher proportion of patients in the lenvatinib arm had macrovascular invasion (23%vs19%) or an elevated AFP level (≥200 ng/mL:46%vs39%)[11].It is likely that this higher incidence of poor prognostic factors in the lenvatinib cohort had an influence on the survival outcome of these patients.Another demographic imbalance that might have influenced the trial outcome relates to the HCC etiology.In fact,a higher proportion of patients in the sorafenib arm had HCC with a hepatitis C etiology compared to the lenvatinib arm(19%vs26%)[11].This difference is of clinical importance given the fact that the treatment effect of sorafenib depends on the hepatitis status of patients,with the best OS prospects for patients with hepatitis C virus-positive HCC.A third and final element from REFLECT that might have diluted the OS benefit of lenvatinib is that patients with invasion of the main portal vein and patients with a disease bulk of more than 50% of the liver were excluded from the study.As a result,the trial selected patients who were more likely to be eligible for subsequent therapy after disease progression on the study drug.This hypothesis is confirmed by the high proportion of patients in both the lenvatinib arm (33%) and sorafenib arm (39%) who received some form of post-study anticancer therapy in REFLECT[11].These subsequent therapies have likely prolonged the post-progression survival of patients in both treatment arms,diluting the potential OS benefit obtained with one of the two agents in the firstline setting.The fact that the median OS obtained with sorafenib in REFLECT was the longest ever reported with sorafenib in a large RCT further supports the idea that poststudy therapies had an important influence on the OS analysis of this trial[7,11,16,23,24].As such,several elements of the REFLECT trial design might have mitigated the true OS benefit of patients treated with lenvatinibvssorafenib.However,it is important to underscore that these statistical speculations should only be seen as hypothesis-generating.This should not be used as an argument to claim a survival superiority of lenvatinib over sorafenib in the first-line treatment of advanced HCC patients.
As such,a critical evaluation of the OS analysis of REFLECT does not help physicians to make a choice between both TKIs in their clinical practice.Perhaps,more practical advice can be derived from the detailed subgroup analysis performed in the trial.In general,the effect of lenvatinib and sorafenib on OS was consistent across all the investigated subgroups.Nevertheless,some subgroups seemed to have a slightly better OS when treated with lenvatinib instead of sorafenib.With respect to HCC etiology,particularly patients with a hepatitis B virus infection seemed to derive a more pronounced OS benefit from lenvatinib compared to sorafenib (median OS:13.4 movs10.2 mo;HR 0.83;95%CI:0.68-1.02).Regional differences were also seen:While patients with a Western origin had a fairly similar median OS with lenvatinib and sorafenib (13.6 movs14.2 mo),patients from Asia-Pacific displayed a numerically longer median OS with lenvatinib (13.5 movs11.0 mo;HR 0.86;95%CI:0.72-1.02).Finally,the presence of macroscopic portal vein invasion and/or extrahepatic spread(median OS:11.5 movs9.8 mo;HR 0.87;95%CI:0.73-1.04) and a baseline AFP level ≥200 ng/mL (median OS:10.4 movs8.2 mo;HR 0.78;95%CI:0.63-0.98) seemed to be associated with a more pronounced treatment effect with lenvatinib[11].
As indicated earlier,lenvatinib was found to be superior to sorafenib in terms of response rate[11].This finding can be used to make treatment decisions in clinical practice.It is well established that sorafenib mainly induces its survival benefit in patients with advanced HCC by stabilizing the disease.However,in some patients (e.g.,patients with bulky disease),a tumor response may be warranted to alleviate symptoms.When faced with such a patient,lenvatinib is probably the better choice.
Both sorafenib and lenvatinib come with a specific toxicity profile,and these differences should be taken into account when opting for one of the two agents.For example,given the high incidence of hypertension reported with lenvatinib,it seems wise to avoid this agent in patients with baseline hypertension or other cardiovascular risk factors.
Finally,the treatment cost should be considered,especially in the context of the ever-increasing pressure on healthcare budgets.In this respect,two independent costeffectiveness analyses demonstrate that lenvatinib is more cost-effective than sorafenib in the first-line treatment of patients with unresectable HCC[33,34].
As of now,no standard therapies are available for patients who encountered lenvatinib failure.Sorafenib can be considered in such cases,given that about onefourth of patients in the REFLECT trial received sorafenib while taking lenvatinib as the first-line medication[35].Recently,a Japanese pilot study has suggested the potential therapeutic benefit from ramucirumab after lenvatinib failure in HCC patients;nevertheless,another study with more patients could not confirm such benefits in the post-progression treatment[36,37].
IS A CHOICE FOR TKI MONOTHERAPY STILL RELEVANT?IMMUNOTHERAPY-BASED COMBINATION THERAPIES AS A NEW STANDARD IN THE FIRST-LINE TREATMENT OF ADVANCED HCC
Since 2008,sorafenib has been the long-standing standard of care in the first-line treatment for patients with unresectable HCC.It took until 2018,with the publication of the REFLECT trial,before an alternative for sorafenib became available.Recently,results presenting the potential benefits of immunotherapy-based combinations may bring in a crucial change in therapeutic strategies for patients with advanced HCC.In the phase III IMbrave 150 trial,atezolizumab anti-PD-L1) plus bevacizumab (antivascular endothelial growth factor) was compared to sorafenib as a first-line treatment of patients with advanced HCC.The atezolizumab-bevacizumab combination showed a significant and clinically meaningful OS improvement compared to sorafenib(median OS not reachedvs13.2 mo;HR 0.58;95%CI:0.42-0.79;P=0.006).At the 12-mo landmark,67.2% of patients in the combination arm were still alive,12% more than the 54.6% OS rate seen with sorafenib at 12 mo.Besides,the median PFS was 6.8 movs4.3 mo (atezolizumab-bevacizumabvssorafenib;HR 0.59;95%CI:0.47-0.76;P<0.0001).This combination regimen had an expected drug safety profile,with a late deterioration in patients’ quality of life[14].Based on these findings,in May 2020,the United States Food and Drug Administration approved this combination for treating patients with unresectable HCC who had not previously received systemic treatment.In addition,the European Society for Medical Oncology updated its HCC guidelines and endorsed the atezolizumab-bevacizumab combination as a regimen that can be considered a first-line treatment option for advanced HCC patients[35].While the groundbreaking outcome of the trial led to the approval of the new treatment in 16 countries,the same has been questioned for its generalizability,owing to the short duration of the trial follow-up and the lack of both safety and efficacy data in Western patients,in whom liver cancer has a different molecular profile than in Asian patients and in patients with metabolic tumors,autoimmune disorders,and transplanted organs.Interesting results were also obtained with a second immunotherapy-based combination consisting of pembrolizumab (anti- programmed death-ligand 1) and lenvatinib.In an open-label phase Ib trial,104 patients with advanced HCC (BCLC stage B or C,Child-Pugh A,and an Eastern Cooperative Oncology Group performance score of 0-1) were treated with lenvatinib (12 mg/d in patients weighing ≥ 60 kg;8 mg/d in<60 kg) in combination with pembrolizumab (200 mg intravenously every 3 wk).Among the 100 eligible patients,an impressive ORR of 46% was obtained,which is markedly higher than 24% and 17% ORR obtained with lenvatinib or pembrolizumab monotherapy in the REFLECT and Keynote-224 trials,respectively[11,38,39].The responses to the lenvatinib-pembrolizumab combination also proved to be durable,with a median response duration of 8.6 mo.The median OS reported with this combination was unprecedented at 22 mo,while patients had a median PFS of 9.3 mo[36].Based on these findings,the United States Food and Drug Administration granted a breakthrough designation for the use of this combination in the first-line treatment of patients with advanced HCC.However,after the publication of the IMbrave 150 results,this breakthrough designation was put on hold (at that point,pembrolizumab-lenvatinib no longer showed evidence of meaningful improvement over available therapies and,as a result,no longer met the criteria for accelerated approval).Currently,the lenvatinib-pembrolizumab combination is being compared to lenvatinib alone in the randomized phase III LEAP-002 trial,which includes 750 unresectable HCC patients who have not received previous treatment for HCC(NCT03713593).The results of this study are eagerly awaited.
CONCLUSION
Since 2008,sorafenib has been the undisputed standard of care for patients with unresectable HCC who have not received previous treatment for their advanced disease.It took until 2018 for an alternative drug to emerge.In fact,the publication of the pivotal REFLECT trial demonstrated that lenvatinib is non-inferior to sorafenib in terms of OS in the first-line treatment of patients with unresectable HCC.In addition,lenvatinib was shown to be associated with a higher ORR and significantly longer PFS than sorafenib.This leaves patients and clinicians with two equally effective first-line treatment options for patients with unresectable HCC.For physicians to choose which TKI is best to use,they need to consider the individual patient and disease characteristics and consider the specific toxicity profile of both agents.The recent publication of the IMbrave 150 trial demonstrating the superiority of atezolizumab-bevacizumab combination over sorafenib in this setting will radically change the way we treat this disease type.Additionally,the results with the pembrolizumab-lenvatinib combination are very promising but require further validation in larger,randomized trials.Overall,the results obtained with these immunotherapy-based combination regimens are very convincing and will likely make a choice between sorafenib and lenvatinib in this patient group somewhat obsolete.
 World Journal of Gastrointestinal Oncology2021年12期
World Journal of Gastrointestinal Oncology2021年12期
- World Journal of Gastrointestinal Oncology的其它文章
- Management of obstructive colon cancer:Current status,obstacles,and future directions
- Role of endoscopic ultrasound in anticancer therapy:Current evidence and future perspectives
- Mesenchymal stem cell-derived exosomes for gastrointestinal cancer
- Gender differences in the relationship between alcohol consumption and gastric cancer risk are uncertain and not well-delineated
- Pancreatic intraductal papillary mucinous neoplasms:Current diagnosis and management
- Combined treatments in hepatocellular carcinoma:Time to put them in the guidelines?