
Unique situation of hepatocellular carcinoma in Egypt:A review of epidemiology and control measures
2022-01-10 07:58ReemEzzatMohamedEltabbakhMohamedElKassas
Reem Ezzat,Mohamed Eltabbakh,Mohamed El Kassas
Reem Ezzat,Internal Medicine Department,Faculty of Medicine,Assiut University,Assiut 71515,Egypt
Mohamed Eltabbakh,Tropical Medicine Department,Faculty of Medicine,Ain Shams University,Cairo 11566,Egypt
Mohamed El Kassas,Endemic Medicine Department,Faculty of Medicine,Helwan University,Cairo 11795,Cairo,Egypt
Abstract Hepatocellular carcinoma (HCC) is the sixth most common primary malignancy worldwide,and the third most common cause of death among cancers worldwide.HCC occurs in several pre-existing conditions,including hepatitis C,hepatitis B virus,and non-alcoholic cirrhosis.Egypt used to be the country with the heaviest hepatitis C virus (HCV) burden.The relationship between HCV and HCC is an important research area.In Egypt,HCC is a significant public health problem.A possible cause for the increasing rates of detection of HCC in Egypt is the mass screening program that was carried by the government for detecting and treating HCV.A multidisciplinary approach is now widely applied to HCC management in health centers all over Egypt.Different treatment modalities are available in Egypt,with success rates comparable to global rates.The Egyptian health authorities have made the elimination of HCV from Egypt a special priority,and this approach should lead to a decrease in number of HCC cases in the near future.In this article we review the current situation of HCC in Egypt,including epidemiological aspects,relevant risk factors for HCC development,strategies,and efforts established by health authorities for the screening and prevention of both HCV and HCC in Egypt.We highlight the different modalities for HCC treatment.
Key Words:Hepatocellular carcinoma;Liver cancer;Hepatitis C virus;Hepatitis B virus;Screening;Egypt
INTRODUCTION
Hepatocellular carcinoma (HCC) is the sixth most common primary malignancy worldwide[1] with higher incidence and prevalence in Africa and Asia[2].The incidence of HCC worldwide has changed over the past few years,with some areas showing decreased rates,and others showing the opposite[3].
In Egypt,the relation between hepatitis C virus (HCV) and HCC is an important research area.Firstly,Egypt has a high recorded HCV transmission rate,with around 416000 new infections each year[4].Secondly,there is known to be a relationship between HCV and HCC development.Thirdly,the programmed screening and follow up that was initiated by the government increased the number of known cases of individuals having both diseases.According to a study carried out by Ziadaet al[5],108 out of 514 patients diagnosed with HCV infection (21%) had focal lesions detected by ultrasound.In another study carried out by Abd-Elsalamet al[6],HCC occurred more frequently in patients with HCV than in those with hepatitis B virus (HBV)infection.These results may indicate the main predisposing factor for the development of HCC in Egypt.
A possible cause for the increase in detection of HCC in Egypt is the mass screening program that was implemented by the government for detecting and treating HCV.Due to this program,many patients were diagnosed and treated for HCC.According to a study carried out by Shakeret al[7],75% of identified HCC cases came from rural areas in Egypt,with 45.7% of individuals ranging in age between 51-60 years.
According to the global cancer observatory,liver cancer represented 19% of all newly diagnosed cases in all ages and both sexes in 2018,with an incidence rate of 32%and a mortality rate of 31%[8].
RISK FACTORS FOR HCC IN EGYPT
HCV
HCV protein expression in infected hepatic cells causes mutation and malignant transformation leading to the development of HCC[9-11].Repeated inflammation,damage and regeneration are believed to be the main cause of malignant transformation[12].HCV infection increases the risk of HCC development up to 20-fold[13].About 0.5%10% of HCV-related cirrhosis leads to HCC annually[14].There are other factors that increase the risk of developing HCC with HCV,such as male gender,smoking,obesity,diabetes,and HBV or human immunodeficiency virus co-infection[14,15].During the era of interferon-based therapy,sustained virologic response (SVR)and HCV eradication was associated with decreased incidence of HCC[16].This outcome was hoped for from the direct-acting antiviral agents (DAAs),but researchers could not reach an agreement on that point.Reiget al[17] found an early recurrence of HCC in patients receiving DAA (27.6%).This was not the case in other studies,that found no increase in recurrence after DAA therapy[18-21].
Another review was published by Reiget al[17],debating about revising the published data,and they concluded that no solid evidence could be reached about the relationship between HCC recurrence and DAA therapy[22].El Kassaset al[23]concluded that there is a possible role of DAAs in HCC recurrence.
Egypt recorded the highest prevalence of HCV worldwide,as a consequence of unsafe IV treatment of schistosomiasis in 1950s until the 1980s[24].A decline was recorded in the prevalence of HCV infection from 14.7% in 2008 to 10% in 2015.This was attributed to the aging of the group who received antischistosomal treatment[25,26].
In Egypt,genotype 4 is the main genotype,occurring in up to 92.5% of infected patients,followed by genotype 1 (3.6%)[27-30].A study demonstrated that at least in Egypt,the lymphotoxin alpha gene mutation may have a role in susceptibility to HCV infection,and the subsequent development of clinical manifestations[31].
HBV
DNA viruses can be incorporated into a host genome[32],inducing malignant transformation by downregulating tumor suppressor genes and activating oncogenes[9].The annual incidence of HCC is 0.42%[33] which differs according to the presence of HBV infection or cirrhosis[34],with the lifetime risk of HCC development among HBV carriers being from 10% to 25%[32].Antiviral treatment for HBV can decrease HBVDNA levels[35],with improved liver function and histology.There is increasing evidence that nucleos(t)ide analogs (NAs) decrease,but do not eliminate,the risk of HCC development[36,37].
In Egypt,the population prevalence of HBV was 1.4%,with an HBV-HCV coinfection rate of 0.06%[38].The nationwide vaccination program has decreased the prevalence of HBV infection considerably[39,40].The HBeAg negative variant was found to be highly prevalent in Egypt,and represents a late phase of HBV infection with persistent viral replication.This situation will lead to early development of cirrhosis[41].However,16% of patients with HCV have an occult B infection[42] A study carried out by Fouadet al[43] found that 81.9% of their chronic HBV cohort were HBeAg negative.
Of patients with liver cirrhosis,3%-5% develop HCC annually[44].In Egypt,HCC represents nearly 70% of all liver tumors[45].The increased incidence in Egypt may be related to the increased screening carried by the government.and a greater focus on HBV and HCV as predisposing factors in the past few years[46].
Environmental toxins
The liver is the main organ involved in the metabolism of chemical agents[47].It has a characteristic blood supply,and is involved in many metabolic and excretory processes.This causes damage to the liver ranging from fatty liver,hepatocellular injury,cirrhosis,and HCC.
In Egypt,nearly 26% of the population works in agriculture[48],and thus have a high risk of exposure to pesticides.A study carried out by Abou El Azmet al[49] found that 13.87 % of the total HCC in Egypt was associated with risk factors other than HVB or HCV,predominantly pesticides,and superphosphate and ammonium sulfate fertilizers (94.87%,P<0.001) with significant exposure occurring in industry,farming,and residences.The HCC in these cases had specific criteria,being solitary,of smaller size,and having lower alpha fetoprotein (AFP) titers[49].
Aflatoxins are known to have a major role in the development of HCC in Egypt.They are known carcinogenic metabolites of molds,mainlyAspergillus flavus,and parasites that contaminate many agricultural products,such as peanuts,maize,and cotton seed[50].
Beside molds,a study conducted on desserts in Egypt showed that aflatoxin B1(AFB1) was detected at above the acceptable limits of 2 ppb in 70% of samples of one of the dairy desserts,and Aflatoxin M1 exceeded the limits in 10% of each type of sample[51].High serum levels were detected in Egyptians with HCC by a study that was carried out by Dilberet al[52].AFB1 is the main metabolite produced,and is the most carcinogenic,teratogenic,and mutagenic metabolite[53].It was present in high levels in those presenting with multiple hepatic focal lesions over 5 cm in diameter[54].Anwaret al[55] found that presence of Aflatoxins and HCV is connected to hepatic disease progression to G3S3 which indicates HCC.Aflatoxin levels were found to be significantly higher in HCC patients than in cirrhotic individuals and controls in a study conducted by Sharaf-Eldinet al[56].
Non-alcoholic fatty liver disease
Non-alcoholic fatty liver disease (NAFLD) produces abnormal fat accumulation in the liver,without significant alcohol ingestion.NAFLD includes a broad spectrum of liver conditions ranging from steatosis and reaching up to cirrhosis.It is considered to be the most common liver disease related to obesity[57],and is a condition that can progress to HCC[58].HCC development is related to disease progression from NAFLD to non-alcoholic steatohepatitis (NASH).NAFLD can accelerate the disease burden of HCV in terms of morbidity and mortality[59].A study that was carried out on school children in Egypt,fatty liver was prevalent in 15.8% of the study group,and increased significantly with age (P=0.004)[60].NAFLD (56.8%) was a predominant feature among the study population in a study that was conducted by Abd El-Wahab EWet al[61] on 190 adults seeking health check-ups at the outpatient clinic of a tertiary care hospital in Alexandria,Egypt.Fatty liver was detected in 47 (65.3%) children,and in 52 (62.7%) adults in another Egyptian study by Wafaaet al[59].A study concluded that NASH is present in 5.3% of Egyptian patients presenting with HCC[62].This finding reflects the high prevalence of the condition in Egypt,and the subsequent increased risk of HCC transformation.Screening and early detection of the condition indicates the importance of avoiding further burdens on public health,as in the campaign carried out by the Egyptian government last year with respect to the detection of obesity,diabetes,and hypertension as predisposing causes for NAFLD.
Lifestyle factors (alcohol consumption,smoking,and dietary factors)
Excessive alcohol consumption is a well-known risk factor for developing HCC[62].In the European Union,60%-80% of liver-related mortality is caused by excessive drinking[63] and alcohol-related chronic disease is considered to be the second most common indication for liver transplantation,accounting for approximately 40% of all primary liver transplants[64].In Egypt,this risk is low[48,65-67].Heavy alcohol consumption increases the risk of HCC by up to 16%[68].The risk is increased by 5- to 7-fold with heavy ethanol consumption for more than 10 years[69,70].
Smoking is another factor that may lead to HCC,due to the tobacco[71].A Korean study reported a connection between primary liver cancer and smoking with the risk increased by up to 50% compared with non-smokers[72].Bakir and Ali-Eldin[73]concluded that 64% of Egyptian patients with HCC are smokers.Abou El Azmet al[49]reported that heavy smoking is one of the primary risk factors for non-B non-C HCC in Egypt.Another study mentioned smoking as one of the main causative agents for HCC in Egypt[5].Another Egyptian study documented an increased risk of HCC development in patients with a smoking pattern of 20 cigarettes per day for more than 29 years[74].
Obesity
Around 1.9 billion people around the world are overweight,and 600 million are suffering from obesity[75].Obesity is related to the development of many metabolic disorders,including diabetes mellitus and hypertension,with an increased burden of HCC development.Premorbid obesity is associated with up to a two-fold risk of HCC related mortality[75].It has been suggested that for every 5 unit increase in body mass index (BMI),there is a 39% increased risk of HCC[76].In another study,carried out by Calleet al[77],the HCC related mortality in obese men (BMI,30-34.9 kg/m2) was 1.9 times the number in men with normal BMI (BMI 18.5-24.9 kg/m2).
In Egypt,a study on primary school students showed that the overall prevalence of obesity and overweight was 13.9% and 16.2% respectively[78].In adults,it is estimated to be present in 61%70% of the whole population aged 20 and above,with a prevalence of 18%22% in men and 39%48% in women[79].Aitsi-Selmiet al[80] investigated the relationship between wealth,education,and obesity among 49058 Egyptian women using the Demographic and Health Surveys’ datasets.Obesity was mainly recorded among women with a primary education or less,and whether they are poor or wealthy.A survey of young people in Egypt[81] found that consuming more white bread and carbonated drinks is directly related to their economic state.
Genetic factors
Some hereditary liver diseases with genetic mutations are believed to carry a risk for HCC development.These diseases are Wilson disease,hemochromatosis,alpha-1 antitrypsin deficiency,tyrosinemia,glycogen storage diseases,and porphyrias.The same is true for polymorphisms with increased risk for HCC.Polymorphisms inUGT1A7,MnSOD,andIL-1Bwere reported to be significantly associated with risk[82].HCV and HBV infection are reported to increase the risk of gene mutation,leading to the development of HCC[83-87].
In an Egyptian study,the TNF-α-308 G > A polymorphism was associated with increased HCC risk in an Egyptian population,but no significant difference was found for cytokines interleukin (IL)-1β and IL-10[88].In another study on Egyptian patients,XRCC1 G28152A (rs25487) and XRCC7 G6721T (rs7003908) polymorphisms were found to have a role in susceptibility to HCC in the Egyptian population[89].
Epidermal growth factor gene polymorphism 61*G was found to be positively associated with HCC risk in Egyptians.Uncreased concentration of EGF was associated with the G/G genotype[90].
The prevalence of hereditary hemochromatosis in Egypt is reported to be 0.5%[50].This indicates that hereditary disorders are not a major cause of HCC.
Preventive measures:HCV control in Egypt
In 2015,10% of the population tested positive for HCV antibodies,which would amount to around 5.5 million persons at that time[91].As a major cause of HCC in Egypt,after the World Health Assembly’s decision in 2016 to eliminate HCV,the Egyptian government decided to begin a nationwide campaign for the detection and treatment of HCV in Egypt[92].More than two million individuals were treated by the year 2018 under the umbrella of this campaign,with cure rates reaching 90%.Disease elimination was achieved mostly by the decrease in the cost of direct-acting antiviral drugs implemented by the Egyptian government.This process was first applied to identified chronic patients.The government then began mass screening of the population,to facilitate rapid and effective elimination of the disease.Screening was done in all of the hospitals related to universities,military hospitals,rural health units,and police hospitals.This was achieved by moving teams to other areas,using gathering spaces,factories,and open places to aid in the screening.Finger prick rapid diagnostic tests were used.Patients reported positive were scheduled for evaluation and treatment plans.Between October 2018 and April 2019,79.4% of the targeted population participated spontaneously in the screening,with higher female than male participation (84.5%vs74.6%).By the end of September 2019,1148346 (76.5%) of screened individuals were reported to have viremia,and treatment was started in 91.8% of them.Out of these people,465992 reached 12-wk follow up after ending treatment.At this stage,386103 (82.9%) had a known treatment outcome,and 381491(98.8%) of those with a known outcome had a SVR.Of the 93651 patients with viremia who did not show up for treatment,53445 who were reached reported having treatment in private[93].
There have been no screening programs for HCC in Egypt until now.Because HCC in Egypt is mostly diagnosed early,as more patients are diagnosed under surveillance,the survival duration is longer than in other African countries[94].The effect of treatment itself is controversial.A study carried by El Kassaset al[23] reported:“Our data point to a high (i.e.,almost 4 times) increased rate of recurrence after DAA treatment for patients with a history of successfully treated HCC,when compared to similar patients who were not given DAAs”.
After HCV elimination,decreased rates of HCC were expected,but Reiget al[17]found exactly the opposite tendency after using direct-acting antiviral drugs for HCV treatment.
This work was followed by a paper that emphasized the early occurrence of HCC in patients receiving DAAs for HCV[18].Another study produced different results,in which no difference in the cumulative incidence was found in developingde novoHCC in patients with HCV and those treated by DAAs or interferon-based therapy[95].Similar results were reached by Cabibboet al[96].A study on patients with HCVrelated cirrhosis treated with DAAs and subsequently developing HCC reported a relation between age,Child-Pugh classification,liver stiffness,history of HCC,and the development of HCC[18].In 2019,a study on 7344 patients concluded that DAAs decrease the risk of developing HCC[97].
An Egyptian study concluded that DAAs do not increase the risk of HCC recurrence,but still did not recommend abolishing it,rather implementing close follow up[98].Another study denied the occurrence of HCC after DAAs although a high incidence of recurrence was still found.This study also suggested that high AFP before treatment is a good predictor for developing HCC[99].
Immunization for HBV and protection against HCC was discussed in a study on an analysis of 1509 patients with HCC in Taiwan.The study concluded that risk reduction of HCC is obvious after immunization of infants against HBV[100].The HBV vaccination program in Egypt began in 1992 with a schedule of 2,4,and 6 mo of age.This program was not associated with simultaneous screening for pregnant women[101].A multicenter study was carried on 3600 children aging from 9 mo to 16 years old to assess the effectiveness of the Egyptian vaccination program.The study concluded that the vaccination is protective from 1 years to 16 years post vaccination[40].Another study assessed the benefit of follow up post vaccination response and seroprotection persistence,to determine the importance of booster doses in healthy subjects.A protective level of HBsAb was found (> 10 IU/mL) among 66.7% of all individuals studied[102].The risk of HCC danger is escalated by co-infection with occult HBV in HCV patients[103].
HCC SCREENING
Screening programs gain value when the benefits from screening are greater than the expected harm.A large randomized controlled trial showed benefits for screening noncirrhotic HBV patients for the development of HCC,leading to improved early detection,better treatment,and better survival rates[104].An association between screening for HCC and improvement in three-year survival rates is well established[105].A study observed the difference between the survival rates of HCC in Japan and in Hong Kong.Japan has an intensive screening program unlike Hong Kong.The survival rate was 52vs17.8 mo[106].In spite of the psychological or financial harm that could result from screening for HCC,the benefits overweigh the harm.Cirrhotic patients show an annual risk of 2%-4% of developing HCC which makes screening highly recommended in all cirrhotic patients whatever the etiology[107,108].
The risk of progression to HCC in non-cirrhotic patients has ranges from 7% to 54%,varying according to etiology and geographic distribution[109].The most common etiological factors for this condition are obesity,aflatoxins,NAFLD,genetic mutations,smoking,inherited diseases,and sex hormones[107,109-112].Non-cirrhotic liver HCC has a better prognosis and better results following surgical intervention than cirrhotic liver HCC[113].In the European Association for the Study of the Liver 2018 report,a risk stratification model was recommended for non-cirrhotic HCC patients,namely PAGE-B (platelet,age,gender,hepatitis B),that is currently used in non-cirrhotic HBV patients[114,115].
The risk of HCC development in cirrhotic patients is from 2% to 4% annually.This high risk makes screening an obligation for all cirrhotic patients,whatever their etiology[107,111].Screening is mainly to be done for compensated cirrhosis with Child-Pugh class A and B,while class C is to be offered liver transplantation[116].
Screening methods
Ultrasound is the most widely used imaging technique for regular screening for HCC.It has many advantages,being easy,readily available,non-invasive,and inexpensive.The sensitivity of ultrasound in detecting HCC is not more than 45%[117],especially in lesions less than 1 cm in diameter[118].It is affected by the operator,the patient ability to hold their breath during examination,and the nodularity of the liver,which makes the detection of new lesions difficult,with some areas unreachable,like the dome of the liver.Obesity and NASH renders examination difficult which,decreasing the efficacy of the procedure[119].In such cases,magnetic resonance imaging (MRI) and computed tomography (CT) scanning can replace ultrasound[120,121],but they are not cost effective,so they are not considered as first-line screening methods for HCC[119,121].
Biomarkers
AFP is the biomarker most widely used in screening for HCC[122].Although it is readily available,inexpensive,and easy to perform,its addition in the guidelines along with ultrasound was debatable.The American Association for the Study of Liver Diseases recommends using ultrasound,with the use of AFP to be judged by the clinician according to the patient’s condition[107].However,European guidelines recommend using ultrasound with no AFP needed[123].
In Egypt,HCV is the main etiological factor for liver cirrhosis,followed by HCC.Liver elastography is a documented method for assessing liver stiffness.A study investigated its role in the early detection of HCC in HCV cirrhotic patients.It recorded cutoff value of 24 kPa for diagnostic prediction of HCC produced sensitivity 100%,specificity 83.3%,PPV 94.5%,NPV 77.3%,and AUC 89%[124].Another study discussed the superiority of an abbreviated MRI protocol over AFP and ultrasound in detecting small hepatic focal lesions in post HCV cirrhotic patients[125].
A scoring system was suggested by Abdelazizet al[126].The HCC Multidisciplinary Clinic-Cairo University (HMC-CU) score (Logit probability of HCC=-2.524 + 0.152 ×age -0.121 × Hb -0.696 × INR -1.059 × Alb + 0.022 × AFP + 0.976 × Sex.Male=1,Female=0),with a cutoff of 0.559 was superior to other scores for predicting HCC,having a sensitivity of 90% and a specificity of 80.6%.In 2010,El-Zayadiet al[127]investigated the effect of surveillance of HCC on tumor staging and treatment options in Egypt.The study divided the patients into two groups:(1) For those who followed screening regularly;and (2) Who were diagnosed as HCC as first presentation with no screening program followed.They produced variable results three months after interval screening was suggested,as the doubling time of the tumor size is from 1 mo to 19 mo,and as HCV is the main predisposing factor in Egypt.The study reported that surveillance increased the detection of small lesions in the absence of vascular invasion.
A prospective study carried out by Gomaaet al[46] on 2000 patients diagnosed with HCC reported that BCLC has the best prognostic stratification for Egyptians with HCC.Salamaet al[128] suggested adding leptin to AFP for HCC screening in Egyptians.All of these studies were trials from separate centers to detect and screen for HCC in Egypt.
TREATMENT OF HCC IN EGYPT
HCC is a disease with different modalities of treatment.Surgical resection comes in the first place,followed by liver transplantation.Ablative techniques come next,including ethanol (percutaneous ethanol injection),microwave (MWA) or radiofrequency (RFA),catheter-directed trans arterial chemoembolization (TACE) or radioembolization(TARE).Last comes external beam radiation therapy in the form of stereotactic body radiation therapy or proton beam therapy,systemic targeted small molecule tyrosine kinase inhibitors (TKIs),check-point inhibitor immunotherapy,and investigational agents.
A multidisciplinary approach has been now widely recognized and is the mainstay in managing HCC in different health centers all over Egypt.This approach includes a scientific committee with the patient of HCC presented to it,and through discussion is performed,along with counseling the patient with different treatment options.
Surgical intervention
Surgery for HCC includes tumor resection or liver transplantation.Liver transplantation is the best choice,as the whole organ is replaced by a new one,and the underlying pathology is ended forever.However,this is not possible in all cases.Milan criteria were developed to diagnose a patient’s suitability as a candidate for liver transplantation[129].When it is inconvenient to do transplantation,surgical resection of HCC comes next.In non-cirrhotic patients,tumors less than 5 cm are best offered resection as the best treatment modality from an oncological point of view[130].However,partial resection carries the risk of tumor recurrence[131].Tumor size is not a contraindication for partial hepatectomy,but other factors such as extrahepatic metastasis,vascular invasion,main bile duct affection and portal hypertension may affect the decision[132].In an Egyptian study carried out by Zakariaet al[132],the researchers concluded that total tumor volume is an appropriate prognostic measure to evaluate the tumor burden in HCC patients.Assessment of the hepatic function and future remnant liver are cornerstones in the liver resection decision[133].A study carried out by Senbelet al[134] concluded that hepatic resection is an effective treatment for Child-Pugh A patient candidates for liver transplant.A study at Assuit university hospital reported 28 cases that underwent hepatic resection for HCC from 2013-2017.The study defined low serum albumin,high MELD score and high Child score to be risk factors for developing post-resection liver failure[135] in 268 patients who had undergone hepatic resection between the years 2010 and 2019 in Mansoura University,Egypt[136].
In Arab countries,3804 liver transplants were done between the period 1990-2013,of which living donor liver transplantation (LDLT) was 80%,and deceased donor liver transplantation was 20%.Fifty-six percent of the reported cases were in Egypt[137].In Egypt,the only source for a liver graft is from a living donor.From 2001 to 2019,1230 cases of liver transplantation were reported from three transplantation centers in Egypt.Of them,394 cases were HCC transplanted patients.In a retrospective study done by the surgical team in Dar ALfouad,Egypt,60 patients with HCC who had undergone liver transplant within and beyond the Milan criteria were investigated for their clinical outcome.The results were as follows:“Overall 1-,3-,and 5-year survival rates were 98.3%,93.5%,and 71.4%.Overall disease-free survival rates at 1,3,and 5 years were 96.6%,93.5%,and 64.2%.There was no statistically significant difference in overall survival time between patients within and beyond the Milan criteria.Factors affecting recurrence were the tumor grade,lobar distribution,size of the largest nodule,and the total tumor burden in the explanted liver”[138].In a study done by Galalet al[139],the researchers concluded that AFP may predict HCC recurrence after LDLT (area under the curve=0.806) at cutoff values of more than 66 ng/mL,with 60%sensitivity,94.3% specificity,42.9% positive predictive value,and 97.1% negative predictive value.
We in Egypt have certain constants regarding liver transplantation as an option for HCC treatment,the major issue being the high cost of the operation,and the difficulty of finding a proper matched donor,as only living donor transplant is allowed in Egypt.Nevertheless,the success rate of liver transplant in Egypt is comparable to international results.So,it became of importance to allow health insurance coverage for liver transplantation operations in public health centers as a better treatment option for Egyptian HCC patients.
Local ablation techniques
Using thermal ablation for hepatic focal lesions has many advantages,such as the ability to repeating the maneuver,low morbidity and very few complications[140].MWA ablation provides better results in areas with high blood flow,or near vessels,because it is not affected by the heat sink effect[141].An Egyptian study carried out by Solimanet al[142] aimed to investigate the efficacy of MWA ablation in risky areas adjacent to other organs,near the diaphragm,and near blood vessels.In the study group,MWA reached ablation rates of 100%,75%,and 87.5% for lesions close to the gall bladder,perivascular lesions,and subcapsular lesions,respectively.Another study done at Menoufia university,Egypt,compared single local ablative and combined techniques in HCC.The combined locoregional method provided better results[143].However,Kamalet al[144] found no difference between MWA ablation and RFA ablation in treating HCC.Due to the high incidence of HCC related HCV in Egypt,the high risk of recurrence in those patients was investigated by Sharaf-Eldinet al[145].The study concluded that in those patients,the presence of hepatomegaly,heterogenous liver,and splenomegaly,a sign of portal hypertension,together with tumor factors such as large size,bilobar affliction,and lesions near the liver capsule,showed a significant association with tumor recurrence.
TACE
TACE is the treatment of choice for patients with intermediate stage HCC,according to BCLC[123].It is also the standard treatment in non-resectable HCC[107].It is considered to be a palliative treatment,with positive impacts on survival and quality of life[146].Since Seldinger described his technique in 1953,many intravascular procedures have been used[147].This was followed by percutaneous selective angiography and arterial infusion of vasopressin by catheterization for controlling gastrointestinal bleeding.For more than a decade there was a debate about the use of chemotherapy to support TACE over trans arterial embolization[148].Many studies supported TACE for providing both embolectomy and chemotherapy,and for keeping a good hepatic reserve for better survival[149-151].TACE is not used only in nonresectable HCC,but also for downstaging before liver transplantation[152],and has good outcomes and overall survival[153].Farouk Ahmedet al[154] found that the main etiology for HCC in Egypt is HCV.Patients who were inappropriate for transplantation,being outside of the Milan criteria,were chosen for downstaging by TACE before transplant.The study showed that good selection of patients for downstaging by TACE has good outcomes on liver transplantation.The patients’ quality of life post TACE was evaluated by Fouadet al[155] in a study on 99 patients with HCC.The study showed improved quality of life after three months.In another Egyptian pilot study,RFA ablation showed better results with respect to quality of life than TACE[156].
TARE
Guidelines recommend TACE as the standard line of treatment for BCLC-B,but the results are still not very satisfactory[157].Radiation from external beams to the liver is not effective in delivering lethal doses,as HCC is radio-resistant[158].Radioembolization with Yttrium-90 microspheres is a recently used catheter-based treatment for HCC.It can be performed safely in patients with portal vein thrombosis,due to its low embolic effect[159].TARE has the advantages of short hospital stay[160],prolonged time until progression[148],and long progression free survival[161].
Hamedet al[162] investigated the efficacy of Yttrium-90 on 20 Egyptian patients with intermediate and advanced HCC,with good outcomes even in the presence of compromised liver functions.Similar results were produced by Hettaet al[163],in a study in which TARE was investigated in advanced HCC with or without portal vein thrombosis.TARE Y90 showed the best results,especially in advanced stage disease,when compared to TACE in a study on 86 Egyptian patients with intermediate HCC[164].
Systemic therapies
Treatment for advanced HCC is now based on systemic therapy relying on TKIs,antiangiogenesis agents,and immunotherapy[123].Before the development of sorafenib,no drug was available that could provide this improved overall survival in such patients[165].Sorafenib is an oral multi-kinase inhibitor with anti-proliferative and anti-angiogenic properties.It acts by inhibiting vascular endothelial growth factor receptor (VEGFR) -2 and -3 tyrosine kinases,platelet-derived growth factor receptor(PDGFR)-β tyrosine kinases,and rapidly accelerated fibrosarcoma kinases[166].Sorafenib was first used in cases with well-preserved liver function,but results from the Global Investigation of Therapeutic Decisions in Hepatocellular Carcinoma and of its treatment with sorafenib (GIDEON) found a similar safety profile,irrespective of Child-Pugh staging[167].Routine use of sorafenib in patients with underlying liver dysfunction is not recommended.
Lenvatinib (Lenvima,Eisai) is an oral TKI of fibroblast growth factor receptor(FGFR),VEGFR,PDGFR-α,rearranged during transfection,and KIT.It has been accepted as a first-line therapy for unresectable HCC since August 2018[168].Regorafenib (Stivarga,Bayer) came next.It is a potent oral inhibitor of angiopoietin-1 receptor (Tie2),VEGFR,PDGFR,and FGFR,and was studied by Bruix and colleagues in patients who did not respond to sorafenib.It was approved by the FDA based on this multinational study[169].
A study on sorafenib in Egypt claimed that it cannot be used except in patients with Child A and low disease burden[170].The same recommendation was made by Abdel-Rahmanet al[171].When sorafenib was studied in Egyptian patients with advanced HCC,it gave better outcomes,overall survival,and progression free survival when compared to no treatment[172].It is,however,considered to be a costly treatment for the Egyptian patients,as was found in a study carried out by Hamdy Elsisiet al[173],in which they concluded that “sorafenib does offer increased survival and quality of life at an increased cost but at an incremental cost effective ratio that exceeds the nationally accepted cost-effectiveness threshold”.Hanafy showed that a combination of sorafenib and low dose capecitabine is effective in advanced HCC in an Egyptian population[174].
A comprehensive summary of studies discussing the results of different treatment modalities for HCC in Egypt is presented in Table 1.
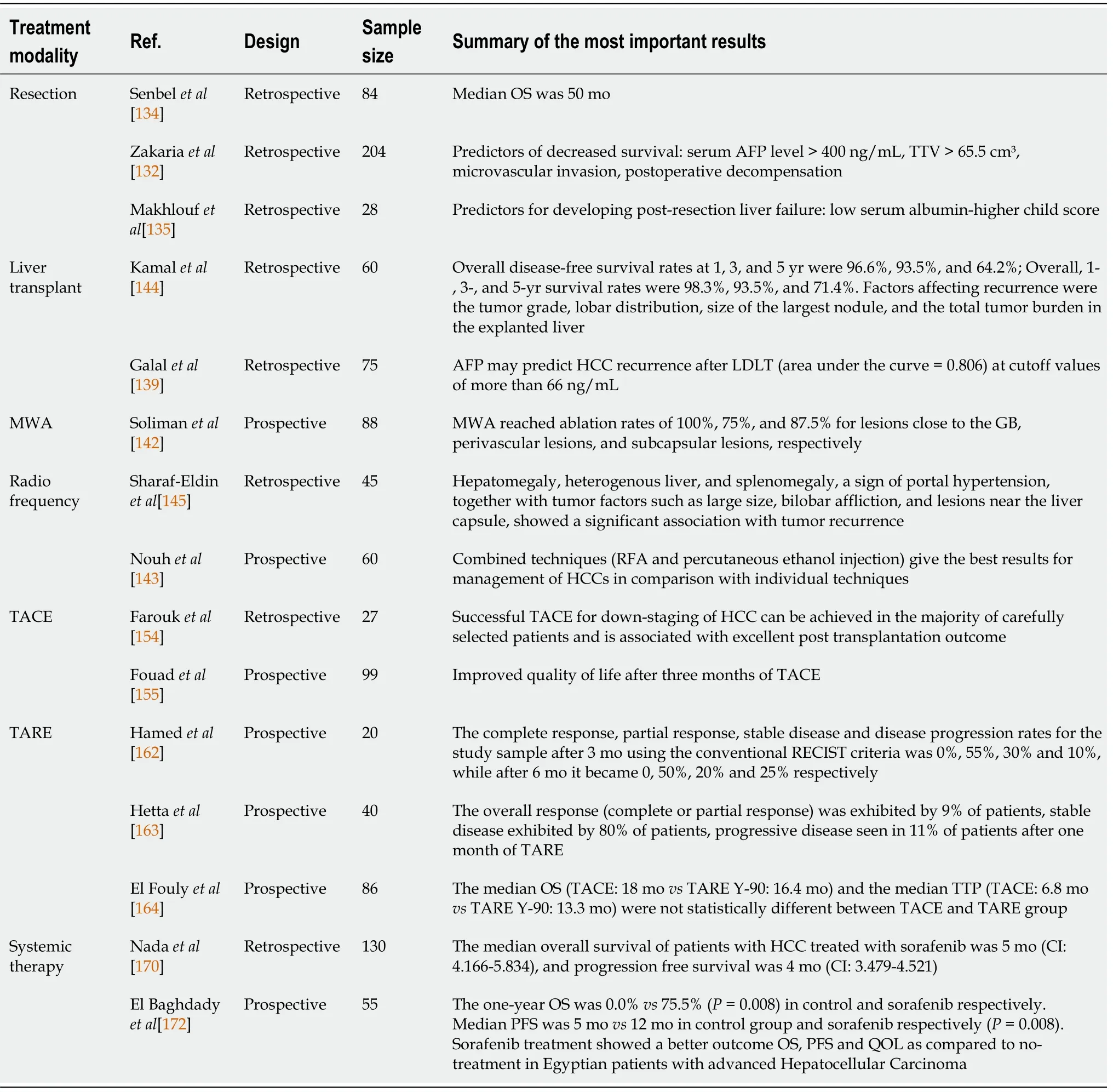
Table 1 Summary of studies discussing the results of different treatment modalities for hepatocellular carcinoma in Egypt
NATIONAL POPULATION-BASED CANCER REGISTRY PROGRAM
The Egyptian National Cancer Registry Program (NCRP) was launched in 2008 to represent a source for cancer incidence figures in Egypt[175].NCRP stratified Egypt into 3 geographical areas:lower,middle,and upper.Data are regularly collected from specialized cancer treatment centers that are scattered all over the country map.Results of NCRP showed that HCC was the first among the most frequently observed cancers in lower and middle Egypt and the 2ndin upper Egypt (Figure 1).
Figure 1 Proportion and age standardized rate of liver cancer in lower,middle,and upper Egypt (results of the National Population-Based Cancer Registry Program).
HCC SCREENING AFTER HCV TREATMENT WITH DAAS
A major breakthrough was noted after the national campaigns of fighting and screening HCV,in which all of the population was screened for HCV,and basic laboratory results and ultrasonography were performed[93,176].Many HCC patients were discovered and provided with treatment options.Despite the high safety profile of DAAs therapy,which enabled treatment of advanced cases and with expected lower incidence rate of HCC post-treatment,there were some contradictory reports on HCC incidence rates post SVR[177].
The major drawback in our campaign in Egypt was lack of a program after achieving SVR for continued screening for HCC after cure of HCV,with a resultant faulty impression of the patient that they were completely cured,with no need for lifetime follow up and screening for HCC.
This is why it is important to highlight the importance of screening for HCC for all individuals with SVR for cirrhotic features for life.Increasing public awareness of the importance of the screening is warranted just as in the national screening campaign for breast cancer in Egypt 2020[178].
Major screening programs in Egypt,like the National Initiative of 100 Million Healthy Individuals and Breast Cancer 2020 have produced high success rates[178].Now it is time for proper guidance and screening programs for HCC in Egypt.
CONCLUSION
HCC is a disease posing a rising burden in Egyptian society.HCV is the main etiology in our country,with an expected decline following the decline in HCV incidence.HBV is the second most important etiology in Egypt.Mass vaccination campaigns are the only way to stop the disease and ameliorate its effects.A registry of the different modalities for management for HCC is still lacking in Egypt,and will require a more systematized effort between different centers.A national campaign is crucial for early diagnosis and management.
 World Journal of Gastrointestinal Oncology2021年12期
World Journal of Gastrointestinal Oncology2021年12期
- World Journal of Gastrointestinal Oncology的其它文章
- Management of obstructive colon cancer:Current status,obstacles,and future directions
- Role of endoscopic ultrasound in anticancer therapy:Current evidence and future perspectives
- Mesenchymal stem cell-derived exosomes for gastrointestinal cancer
- Gender differences in the relationship between alcohol consumption and gastric cancer risk are uncertain and not well-delineated
- Pancreatic intraductal papillary mucinous neoplasms:Current diagnosis and management
- Combined treatments in hepatocellular carcinoma:Time to put them in the guidelines?