
Therapeutic efficacy observation of warm needling moxibustion plus spine subtle adjusting manipulation for cervical radiculopathy
2021-12-17 10:52:34PanGuoliang潘国良ZengLiang曾亮DongXiaowei董晓薇
Pan Guo-liang (潘国良), Zeng Liang (曾亮), Dong Xiao-wei (董晓薇)
Shanghai Pudong Hospital (Fudan University Pudong Medical Center), Shanghai 201399, China
Abstract
Keywords: Acupuncture Therapy; Warm Needling Moxibustion; Manual Therapies; Tuina; Massage; Neck Pain;Radiculopathy; Cervical Spondylosis
With the change of modern living habits, the incidence of cervical spondylosis is increasing year by year. According to the data released by the World Health Organization, the global incidence of cervical spondylosis is second only to that of cardiovascular and cerebrovascular diseases. Cervical radiculopathy is the most common type of cervical spondylosis[1], often causing motor, sensory, and reflex neurological disorders due to the stimulation to unilateral or bilateral spinal nerves[2]. The clinical manifestations are mainly radiculopathy pain and (or) decreased skin sensation in the compressed nerve root distribution area[3], which will seriously affect patients’ quality of life.At present, it is generally believed that the protruding nucleus pulposus, the localized hypertrophy of the posterior longitudinal ligament, and the formation of spurs in the uncovertebral joint can compress the spinal nerve root and cause radiculopathy symptoms[4]. How to solve the problem of nerve root compression is the key to the treatment of cervical radiculopathy. Relevant studies have shown that warm needling moxibustion can relieve local muscle spasms and loosen nerve root adhesions[5]. In addition, spine subtle adjusting manipulation provides a more relaxing internal environment for compressed nerve roots by adjusting the relative position of vertebral joints[6]. In this study, we observed the effect of warm needling moxibustion plus spine subtle adjusting manipulation for the treatment of cervical radiculopathy.
1 Clinical Materials
1.1 Diagnostic criteria
Met the diagnostic criteria for cervical radiculopathy in theExpert Consensus on Standardization of Diagnosis and Treatment of Cervical Radiculopathy[3]. There were localized nerve root compression manifestations, typical radiculopathy symptoms and signs, with the range consistent with the cervical spinal nerve innervation area;with positive Eaten test or Spurling’s test; X-ray or CT examination showed bone hyperostosis or osteophytes around nerve roots due to cervical degenerative changes,or intervertebral foramen stenosis; MRI examination indicated nerve root compression.
1.2 Inclusion criteria
Those who met the above diagnostic criteria; aged 18 to 65 years old; those who had other diseases at the same time but did not need special treatment during the treatment period, nor affect the clinical trial protocol of the first diagnosis; those who stopped other therapies and drugs that might affect the result evaluation in this study; agreed to participate in this trial and signed informed consent.
1.3 Exclusion criteria
Those with surgical indications; those with abnormal imaging findings but without clinical symptoms of the cervical spine; patients with frozen shoulder, thoracic outlet syndrome, tennis elbow, and cervical bone parenchymal lesions (such as tuberculosis and tumors)that mainly present as upper-limb pain; patients with pregnancy or severe diseases not suitable for acupuncture.
1.4 Elimination and dropout criteria
Those who discontinued treatment due to fainting during acupuncture and other adverse reactions; those who had an aggravated condition, or developed complications that may affect the clinical observation should stop the trial according to the physician’s judgment; serious deviations occurred in the implementation of the clinical protocol during this trial,such as poor compliance, which made it unable to evaluate the efficacy; those who terminated treatment due to other irresistible non-treatment factors.
1.5 Statistical methods
All data were statistically analyzed by the SPSS version 18.0 statistical software. The measurement data in normal distribution and having homogeneous variance were expressed as mean ± standard deviation (±s).The pairedt-test was applied to the comparisons of intragroup data. Independent samplet-test was applied to the comparisons between the groups. The measurement data in non-normal distribution or without homogeneous variance were expressed as median(minimum, maximum) [M (min, max)], and processed by Mann-WhitneyU-test for the comparisons between the groups. Wilcoxon’s signed-rank test was applied to the intra-group comparisons. The counting data were expressed by rate, and analyzed by Chi-square test.P<0.05 was considered to indicate a statistically significant difference.
1.6 General data
All cases enrolled in this study were collected from the Acupuncture and Tuina Clinic of the Traditional Chinese Medicine Department of Shanghai Pudong Hospital(Fudan University Pudong Medical Center) between March 2019 and October 2019. All the patients had signed the informed consent before participating in this trial. A randomized single-blind controlled clinical study was conducted. A total of 70 cases were randomly divided into an observation group and a control group by the random number generated by the SPSS version 18.0 statistical software, with 35 cases in each group. There were no dropout cases during the trial. By statistical analysis, there were no statistically significant differences in the data of gender, age, or duration of disease between the two groups (P>0.05), indicating that the two groups were comparable (Table 1).
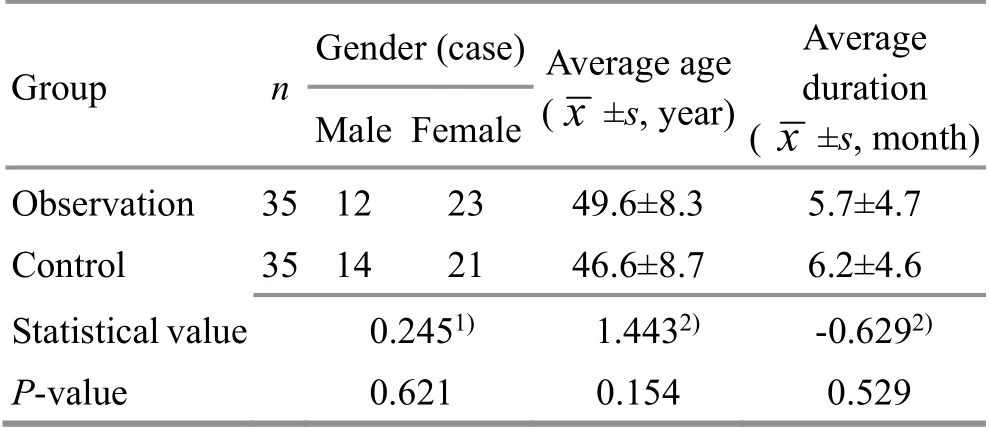
Table 1. Comparison of the general data between the two groups
2 Treatment Methods
2.1 Observation group
Patients in the observation group were treated with warm needling moxibustion plus spine subtle adjusting manipulation.
2.1.1 Warm needling moxibustion
Major acupoints: Bilateral C3-C6Jiaji (EX-B 2) points.
Adjunct acupoints: Binao (LI 14), Quchi (LI 11) and Waiguan (TE 5) were added for patients with upper-limb numbness; Baihui (GV 20) was added for patients with dizziness; auricular point sticking therapy [Shenmen (TF4),Liver (CO12), Kidney (CO10), Heart (CO15) and Subcortex(AT4)] was added for patients with insomnia.
Methods:The Hwato brand disposable sterile acupuncture needles of 0.25 mm in diameter and 40 mm in length (Suzhou Medical Appliance Factory, China)were used for the acupuncture treatment. The patient took a prone position with acupoint areas fully exposed.After routine sterilization, the bilateral C3-C6Jiaji (EX-B 2)points were punctured to the extent that the patient felt soreness. Then the physician slubbed the moxa floss of about 2.5 cm in length (about 2 g) onto those needle handles, and ignited it (careful to prevent falling and scalding). Replaced with new moxa floss after the old one burnt out, three moxa cones for each acupoint. The needles were retained for 20 min.
2.1.2 Spine subtle adjusting manipulation
Releasing manipulation: The physician first An-Pressed and Rou-Kneaded both sides of the cervical spine with the thumb, from light to heavy. After about 5 min, the physician An-Pressed bilateral Fengchi (GB 20)with fingers for about 1 min. Then applied Gun-Rolling manipulation to supraspinatus and levator scapulae for about 5 min.
Subtle adjusting manipulation: Firstly, the physician made the patient relax the neck muscles, then held one side of the mandible with one hand and pressed the head on the opposite side with the other hand, and then slowly turned the head from side to side.
Ca-Scrubbing manipulation: Wintergreen oil ointment was successively applied to the neck Jiaji (EX-B 2) points,Dazhui (GV 14), Tianzhu (BL 10) and Jianjing (GB 21) of the patients with Ca-Scrubbing manipulation, till the skin was slightly red and hot.
2.1.3 Operation sequence and the course of treatment
Warm needling moxibustion was performed first every time, and then spine subtle adjusting manipulation was performed. Each treatment time was 35-40 min. The treatment was performed once every Monday,Wednesday, and Friday for a total of four weeks, 12 times in total.
2.2 Control group
The control group was treated with only the same warm needling moxibustion treatment as the observation group. The point selection, acupuncture needle specification, operation methods, and the treatment course were all as same as those in the observation group.
3 Observation of Curative Efficacy
3.1 Observation items
The visual analog scale (VAS) was used to assess the pain degree before and after treatment. The highest score of VAS was 10 points. The higher the score, the more severe the pain.
3.2 Criteria for curative efficacy
According to theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[7], the curative efficacy in this study was assessed.
Cured: Symptoms disappeared, muscle strength was normal, neck and upper-limb functions returned to normal, and the patient was able to participate in normal labor and work.
Markedly effective: The symptoms were significantly improved. The neck, shoulder, and back pain was relieved. The neck and upper-limb functions were significantly improved and the patient could basically work normally.
Effective: Symptoms were reduced, and the neck,shoulder, and back pain was less, but the symptoms,signs, and dysfunction partially remained, which affected the patient’s daily life and work.
Invalid: There was no change in the symptoms or signs after treatment, or even worse.
3.3 Results
3.3.1 Comparison of the clinical efficacy
The total effective rate was 97.1% in the observation group and 88.6% in the control group. The difference between the two groups was statistically significant(P<0.05), indicating that the efficacy of the observation group was superior to that of the control group (Table 2).
3.3.2 Comparison of the VAS score
There was no significant difference in the VAS score between the two groups before treatment (P>0.05).After treatment, the VAS scores in both groups decreased, and the intra-group differences were statistically significant (P<0.001). There was no statistical difference in the VAS score between the two groups after treatment (P>0.05), but the difference in the change of the VAS score between the two groups was statistically significant (P<0.01), indicating that the observation group was better than the control group in relieving pain(Table 3).

Table 2. Comparison of the clinical efficacy between the two groups (case)

Table 3. Comparison of the VAS score between the two groups before and after treatment [M (min, max), point]
4 Discussion
There are three main theories about the pathogenesis of cervical radiculopathy in modern medicine:mechanical compression theory[8-9], chemical inflammatory stimulation theory[10-11], and autoimmune response theory[12-13]. Mechanical compression directly affects the nerve root, resulting in the abnormal release of local neurotransmitters and inflammatory responses,which is the main cause of root irritation. Besides, the fibrous scars formed after the inflammatory reaction in the nerve root will aggravate the symptoms of nerve root compression. Continuous inflammatory responses and chemical stimulation can cause immune response;neuropeptides are released through immune responses,aggravating nerve root irritation and aseptic inflammation[4].
At present, there are few studies on the mechanism of acupuncture and Tuina (Chinese therapeutic massage) in the treatment of cervical radiculopathy[14-15], and there is no breakthrough. The action principle of warm needling moxibustion in treating cervical radiculopathy still needs to be analyzed from the mechanism of acupuncture itself.Many studies have confirmed that acupuncture can achieve the effects of analgesia[16], anti-inflammatory[17],and immune regulation[18]; moxibustion can regulate the synthesis of inflammatory cytokines by increasing the levels of adrenergic hormones through the hypothalamic-pituitary-adrenal (HPA) axis, and even exert analgesic and anti-inflammatory immune effects simultaneously[19]. Applying moxibustion during acupuncture can relieve muscle spasm, improve local blood circulation, increase blood supply to tissues,promote the absorption of local exudates, reduce edema of protrusions, and reduce nerve compression[20].
Spine subtle adjusting manipulation is to adjust the cervical spine based on soft-tissue relief manipulation. It can correct the displacement and instability of the cervical sagittal plane, improve and restore the cervical physiological radian and cervical spinal curvature, thus redistributing the stresses of the anterior and posterior columns of the affected segment, and reducing the compression load of the anterior column. Therefore, it can reduce the herniation of the cervical intervertebral disc, rebuild the static balance of the cervical spine and improve the root compression[6]. Meanwhile, due to the reconstruction of the balance between dynamic and static forces of the cervical spine, the blood supply around the nerve root is improved, which is beneficial to the absorption of inflammatory factors and produces anti-inflammatory and analgesic effects.
According to the clinical symptoms and disease outcome of cervical radiculopathy, traditional Chinese medicine classifies it into the category of Bi-Impediment syndrome. Wind, cold, and dampness blocking the meridians and collaterals are the main pathological factors leading to this disease, and are also the core to the effective treatment of this disease with warm needling moxibustion. Through the combination of acupuncture and moxibustion, warm needling moxibustion can retain the needles and perform moxibustion at the same time, making the burning heat reach the deep part of the acupoint by the needle body to achieve the effects of warming meridians for dispelling cold and wind, removing dampness, unblocking collaterals, and relieving pain.
The results of this study suggested that warm needling moxibustion plus spine subtle adjusting manipulation can effectively treat cervical radiculopathy and relieve pain. The main mechanism may be the following three aspects. One is to improve the internal environment around the nerve roots and reduce the symptoms of mechanical compression to the cervical nerve roots. The second is the anti-inflammatory, analgesic, and immune regulation effects. The third is the warming effect of moxibustion during warm needling moxibustion, which is deeper and more penetrating and can better play the role of dispelling pathogenic wind and cold and removing dampness. Supplemented by relaxation manipulations,it can better relax tendons and unblock collaterals.
In summary, warm needling moxibustion plus spine subtle adjusting manipulation can treat both symptoms and root causes of cervical radiculopathy. Its curative effect is better than that of warm needling moxibustion alone, and thus it is worthy of clinical promotion.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by Traditional Chinese Medicine Clinical Characteristics and Advantages Brand Project of Shanghai Pudong New Area Health Commission(上海市浦东新区卫生健康委员会中医临床特色优势品牌项目, No. PDZY-2018-0203); Shanghai Sailing Program(上海市青年科技英才扬帆计划项目, No.20YF1443200); Talent Program of Fudan University Pudong Medical Center (复旦大学附属浦东医院院级人才项目, No. PX202008); Clinical Traditional Chinese Medicine Characteristic Discipline Construction Project of Shanghai Pudong New Area Health Commission (上海市浦东新区卫生健康委员会临床中医特色学科建设项目,No. PDZY-2018-0611).
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 13 December 2020/Accepted: 1 February 2021
猜你喜欢
小学生优秀作文(高年级)(2023年9期)2023-10-12 00:42:56
中国毕业后医学教育(2022年1期)2022-08-19 02:52:06
教育教学论坛(2021年26期)2021-08-03 09:34:25
中国医院(2021年4期)2021-04-03 10:17:02
犯罪研究(2019年3期)2019-11-27 19:28:54
时代英语·高一(2019年5期)2019-09-03 02:09:34
武汉理工大学学报(交通科学与工程版)(2019年3期)2019-07-02 06:36:22
小主人报(2018年6期)2018-04-25 09:29:16
西藏研究(2016年6期)2016-02-28 20:53:09
大经贸(2009年5期)2009-08-06 10:03:00
 Journal of Acupuncture and Tuina Science2021年6期
Journal of Acupuncture and Tuina Science2021年6期
- Journal of Acupuncture and Tuina Science的其它文章
- Effects of sinew-regulating bone-setting manipulations on chondrocytes, IL-1β and NO in rabbits with knee osteoarthritis
- Efficacy observation of auricular point sticking in combination with a healthy diet for simple obesity in children
- Clinical efficacy of sticking-needle acupuncture plus tendon-regulating manipulation in the treatment of acute ankle sprain
- Evaluation of the clinical efficacy of muscle regions of meridians needling method for refractory facial paralysis based on infrared thermal imaging technology
- Clinical study on Tuina plus umbilical therapy for senile functional constipation
- Effect of acupuncture on serum PYY and nesfatin-1 in obese patients with insulin resistance