
Quality of life of infertile couples in the Gaza Strip, Palestine
2021-12-08 11:08:44SuhaBaloushahSamiraBarjastehAymenElsousAliAldirawiSohaAbuEidAtefMasad
Suha Baloushah , Samira Barjasteh, Aymen Elsous, Ali Aldirawi, Soha Abu Eid, Atef Masad
1Department of Reproductive Health, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
2Department of Midwifery, Faculty of Nursing, Islamic University - Gaza, Gaza Strip, Palestine
3Faculty of Medical Sciences, Israa University - Gaza, Gaza Strip, Palestine
4Unit of Planning and Institutional Performance Development, Ministry of Health, Gaza Strip, Palestine
5Shifa Medical Complex, Ministry of Health, Gaza Strip, Palestine
6Faculty of Medical Sciences, Israa University - Gaza, Gaza Strip, Palestine
ABSTRACT
Objective: To investigate the quality of life of infertile couples who seek in vitro fertilizations (IVFs) by gender in the Gaza Strip,Palestine.
Methods: A cross-sectional study was conducted, from February 2019 to November 2019, among 383 infertile couples selected through convenient sampling. A valid and reliable Arabic version of the fertility quality of life questionnaire (FertiQoL) was used in data collection. One way analysis of variance and independent t-test were applied to compare between males and females.
Results: The mean age of males and females was (34.54±8.54)years and (29.28±6.71) years, respectively. More than half of them had university degree (64% and 60%, respectively). The mean duration of infertility was (5.66±3.54) years. The mean males’scores of FertiQoL and its subscales (emotion, mind/body, social,core, tolerability, and treatment) were significantly higher than females’ scores (P<0.05).
Conclusions: Males have higher scores of FertiQoL and its subscales than females. The mean score of FertiQoL increases with better education, but decreases with increase of age, duration of marriage, duration of infertility and number of IVF attempts.Routine psychological assessment and counseling are necessary for infertile women taking into considerations factors affecting their quality of life.
KEYWORDS: Quality of life; Infertility; Couples; Gender;Palestine; FertiQoL; IVF
1. Introduction
Quality of life is one of the most important components of health.The concept of quality of life is defined in different ways, however,it can be interpreted in three ways: firstly the welfare aspects of a person’s life, secondly the economic, social and physical abilities and thirdly symptoms of a disease. Measurement of quality of life makes it possible to understand the needs of clients and thus contributes to improvement of quality of services[1,2]. Different factors affect the quality of life of individuals. Infertility is one of the most difficult and effective conditions for quality of life as well as a common problem in today’s world[3].
Significance
It is well known that infertile couples are exposed to some psychological distresses which affect their quality of life, and females as a vulnerable groups are at much higher risks than males. This study adds to the existing body of knowledge about quality of life of couples who failed to have offspring,in undiscovered area in this world. Moreover, contributing factors were also determined. At the end, comprehensive care,including psycho-social, is significant to improve the quality of infertile couples’ life.
According to the World health Organization (WHO), infertility is as an important problem in reproductive health, which is not a disease but it can cause significant emotional disturbances and cause social and psychological consequences[4]. In a study, 12% of infertile women had low quality of life, while more than half had a decent quality of life. Family and community pressure on infertile women had a significant negative impact on their quality of life[5].Infertile women are more vulnerable to undesirable quality of life than men, and thus supporting measures for both sexes, especially women, are essential[6]. The incidence increased by 50% over the past decades, whereas the prevalence of infertility is about 10%-15%, giving that it varies among ethnic groups and races[7-9].
In dealing with spiritual issues, couples’ participation can be a good solution because there is a positive result in each issue of common life between couples[10]. According to the results of the research conducted in comparison with the stressful events of life, infertility is in the fourth place after the death of the mother, the death of the father and betrayal of the spouse[11]. One cause of women infertility can be physical disease such as the polycystic ovary syndrome,which accounts for 5% to 10%[12].
Infertility predisposes individuals to depression and anxiety. The emotional disturbances of infertile couples and secondary symptoms of infertility create a defective cycle that reduces the likelihood of treatment of infertility[13]. On the other hand, infertility treatments cause harmful effects on the physical, economic, and psychosocial aspects and result in reducing self-confidence and disrupting masculinity in men and femininity in women[14]. That is why infertility is considered as defeat in the view point of couples and having a baby is one of the best events that happen for a couple.Also, in the reverse condition, infertility affects the same amount of couple lives[15]. Infertility can be one of the reasons for divorce[16].Also, nearly half of infertile women do not have marital adjustment and experienced problems in their relationship with their spouses.Lower sexual satisfaction in infertile couples than fertile couples was reported. As the treatment progresses, the stress level increases significantly and marital satisfaction decreases[17].
By and large, different researchers have different opinions about the effect of infertility on couples’ relationships. Some researchers believe that tolerating diagnosis and treatment of infertility causes couples to be more intimate, and they will feel closer to each other[18], while many researchers reported declining of couples’performance as a result of infertility. They have emphasized the increase in marital conflicts among infertile couples[19]. As mentioned, quality of life of infertile couples can be varied by ethnic,culture and geographical aspects including Palestine. There is lack of studies on this topic in the geographical area of Palestine, and thus this study aimed to investigate the quality of life (QoL) of infertile couples who seek IVF in the Gaza Strip, Palestine.
2. Materials and methods
2.1. Study design and setting
This study was a cross-sectional survey, conducted on 383 infertile couples who seek IVFs services at Al-Hello, Al-Bassma and Al-Hindawy infertility clinics in the Gaza city, Palestine.
2.2. Data collection and measurement
Data were collected for nine months from February 19th, 2019 to November 2019 by three trained midwifes worked in the selected infertility clinics. Eligible couples met the inclusion criteria: primary or secondary infertility, over 18 years of age, and willingness for participation in the study. The couples were asked to fill the fertility quality of life questionnaire (FertiQoL), while waiting for medical appointment, following face to face interview-based technique.The questionnaire had two parts: firstly, the socio-demographic and clinical characteristics (age, living place, education level, duration of marriage, number of deliveries and abortions, duration of infertility,et al), and secondly the FertiQoL questionnaire, developed by Boivin, Takefman, and Braverman in 2011, consisted of 34 questions and QoL was measured on two sections: core (24 questions) and treatment (10 questions), in addition to two questions asked about personal health and general satisfaction with QoL[20]. The internal consistency, measured by the Cronbach alpha coefficient, of the Core and Treatment FertiQoL (and subscales) was good to excellent and ranged between 0.72 and 0.92[21]. Each item of the FertiQoL was scored from 0 to 4 and the whole subscale score ranged between 0 to 100, giving that higher score means better quality of life.We used the Arabic version available at: http://sites.cardiff.ac.uk/fertiqol/files/2015/02/fertiqol-Arabic.pdf. Average time to fill the questionnaire was 25 minutes.
2.3. Sample and sampling
A convenience sampling of 390 couples was approached. Three women and two men refused to participate and two women provided incomplete questionnaire and the missing values were more than 5%, and thus, 383 couples participated in the study. Sample size was calculated according to traditional formula of the cross-sectional design[21].
2.4. Statistical analysis
Prior analysis, data were checked for completeness, outliers and errors. Data were analyzed using the IBM SPSS 22 (SPSS Inc.,Chicago, Ⅲ). Continuous variables (age, marital years, number of deliveries, etc) were presented as mean and standard deviation (mean±SD). Categorical variables (gender, level of education, menstruation pattern, etc) were presented as frequency and percentage. Mean score of FertiQoL and its subscales, with regard to independent variables,were compared between males and females by using one way analysis of variance and independent t-test. P-value less than 0.05 was considered as statistical significance.
2.5. Ethical statement
Couples were provided with explanation about the purpose of the study and confidentiality of information was ensured. Participation was voluntary-based and couples were asked to give consent prior starting the data collection. Permission was obtained from the administration of the involved infertility clinics and from the Ministry of Health, Department of Research (PHRC/HC/277/19).Data are kept with the first author in private closet and will be discarded once publication is achieved.
3. Results
3.1. Characteristics of respondent couples
The mean age of females and males was (29.28±6.71) years and (34.54±8.54) years, respectively. More than half of them had university degree and more (60% and 64%, respectively). Majority of females were housewives (77.2%), whereas, 75.7% of males had job. The mean duration of marriage was (7.94±2.32) years. More than one third of women had previously delivered a baby and 40% of them had at least delivered one child. The mean duration of infertility of couples was (5.66±3.54) years and 71.1% had experienced at most two IVFs (Table 1).
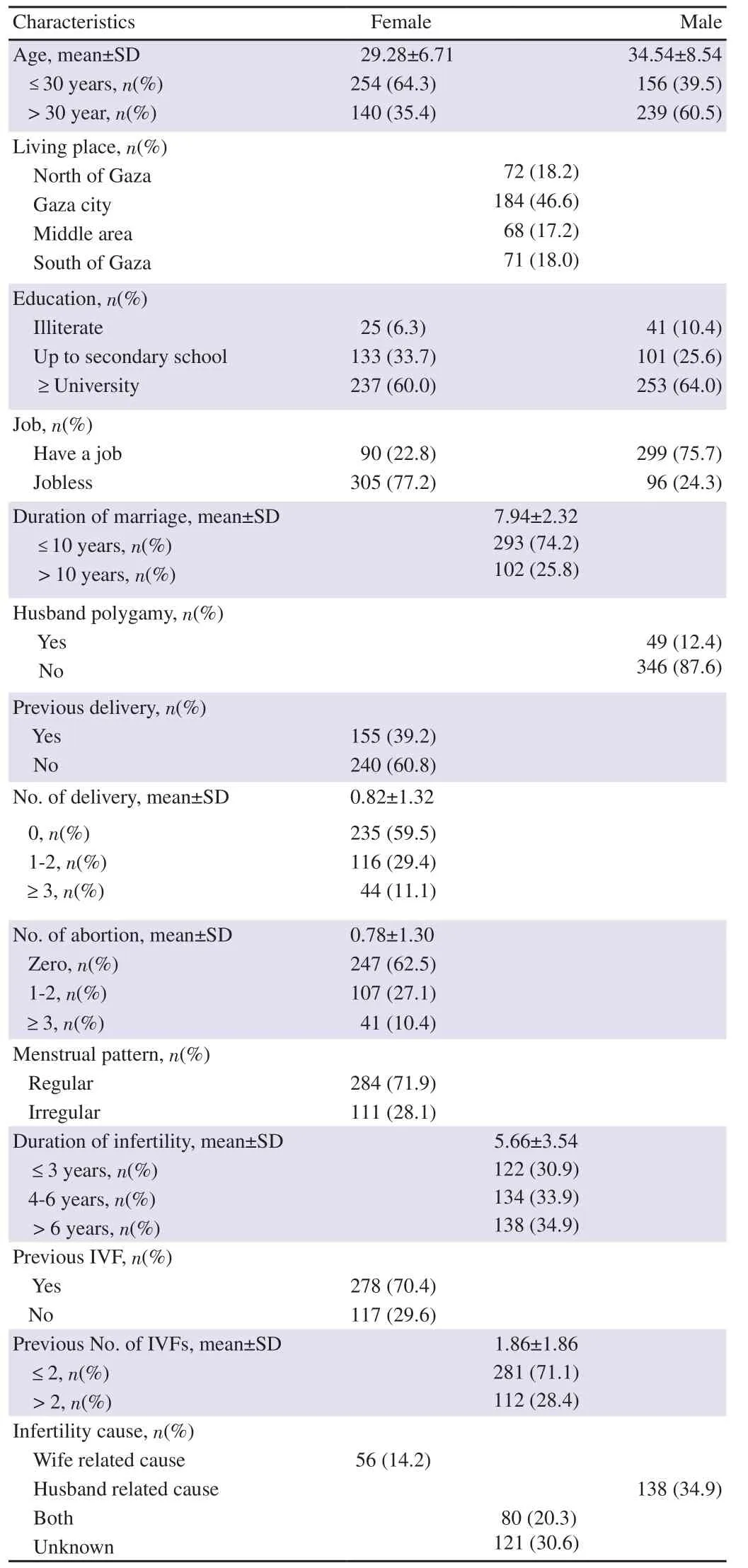
Table 1. Characteristics of participating women and men.
3.2. Perception about health and quality of life
Males’ responses to the question about health in general revealed that one fifth (19.7%) rated their health as poor or very poor and 71.1% perceived their health as good or very good. In turn, 23%of females rated their health as poor and very poor, while 67.3%rated their health as good and very good. With regard to satisfaction about quality of life, one fifth and 67.3% of males were dissatisfied(dissatisfied, very dissatisfied) and satisfied (satisfied, very satisfied),respectively. For females, 20% and 65.4% were dissatisfied and satisfied with their quality of life, respectively.
3.3. Comparison of mean scales of FertiQoL subscales between males and females
The mean males’ scores of FertiQoL and its subscales (emotion,mind/body, social, core, tolerability and treatment) were significantly higher than females’ scores (P<0.05). The quality of life of infertile men is better than in women (Table 2).

Table 2. Differences of women and men scores of the subscale of FertiQoL.
3.4. Relationship between couples’ characteristics and FertiQoL subscales
A significant differences were noticed between women’ duration of marriage, number of deliveries, number of IVFs performed and emotion score. For men, husband polygamy received highest emotion score. Females had lower scores (>50%) than males for the emotion subscale.
Younger males (below 30 years) had significant higher mind/boby and social score than their counterpart females (P<0.05).Males scored higher than females for mind/body and significant differences were seen with regard to age groups, education level and duration of marriage (all P<0.05). Whereas, differences of females’scores for mind/body were observed in the duration of fertility,number of previous deliveries and IFVs (all P<0.05). For women,there was a significant difference between age and the relational,social and core scores (Table 3).

Table 3. Relationship between infertile women’s and men’s characteristics and the subscale of emotion, mind/body, relational, social, and core.
Females who experienced at least three attempts of IVF had lower score for the core dimensions and its subscales. However,differences were significant in core subscale and FertiQoL as a whole. Males and females below 30 years old reported higher scores for the treatment subscales and significance was noticed in the treatment domain and its subscales, and the FertiQoL as a whole (all P<0.05). Similar findings were reported for duration of marriage and number of previous deliveries (P<0.05) (Table 4).

Table 4. Relationship between infertile women’s and men’s characteristics and the subscale of tolerability, environment, treatment and total FertiQoL.
With regard to treatment dimensions, including environment and tolerability subscales, the variables age, duration of marriage,and number of women deliveries were statistically significant for both males and females (all P<0.05). Similar observation was noticed with education level, however, it was not significant in the tolerability subscale for females (P>0.05) (Table 4).
4. Discussion
The current study aimed to explore QoL and associated factors of infertile couples, who seek IVF, from a dyadic or two perspectives.The results of our study showed that husbands’ QoL (in terms of emotion, mind/body, social, core, tolerability and treatment) was more positively affected than their counterparts’ women, which is similar to a conclusion drawn by Goker et al[22]. Infertility is a stressful status, affecting individual’s health including emotions,especially in women. The traditional social pressure in Palestinian society enhances husbands to have a large number of children,especially when infertility is women factor. Infertile Women feel inferior and disappointed[23,24]. Infertility could be life-long and interventions including medical treatments are subjected to failure,and thus psychological, social and economic effects are expected.Emotional support, therapeutic and psychological counseling are vital contributing features for improving quality of life for infertile women[25-27].
Our findings indicated differences in the relation between QoL and age. Youngers have better QoL than infertile individuals above 30 years old, similar to findings of Khayata et al[28]. Significant differences were seen in the score between infertile men and women in the core QoL, treatment QoL and overall FertiQoL. This is against findings of the studies of Goker et al[22], Karabulut et al[26]and Bolsoy et al[29]. Social and psychological support including counseling, to adults, are necessary to infertile couples and raise awareness of society toward infertility as a health issue not a defect or a deficiency.
It is acknowledged that education level has a significant impact on infertile QoL. Infertile individuals of lower education are more prone to social stigma and thus are under much stress[30]. In our study, high education level was a positive influencing factor, similar to previous study of Karabulut et al[26]. As the education level of infertile individuals increases, the QoL improves. Better education contributes to coping and adaptation to stressful experiences.In contrast, lower education level might increase depression of infertile couples and make dyadic adjustment and coping to anxious situation inadequate and difficult[30]. In this study, females with higher education obtained better scores in the core, social, relational and treatment subscales. Previous studies reported no relationship between the women’s educational level and FertiQoL subscale scores[31]. Differences of findings could be attributed to using of various instruments and variations in the socio-demographic background of participated subjects.
Significant relationship is noticed between duration of marriage and QoL. Married men for less than 10 years have higher QoL than their counterparts’ women[32]. However, females’ QoL was only higher for relational subscale. Similar findings were reported from Chachamovich et al[33] and Keramat et al[34]. A possible explanation with regard to Arabic context is that partners are under family pressure, especially from mothers-in-law to see their grandchildren.In Islamic rules, men have chances to get married to other wives if the marriage is failed to bring children. In return, women remain anxious and feared as infertility time increases. They fear from their husbands to get a second wife or to reach menopause time with no backbone support or being a mother. Women prefer to have boys because they are the support in front of families and social pressures.One study found no significant effect between QoL and duration of marriage[35].
QoL of infertile women in all FertiQoL subscales decreased with increased number of IVFs attempts, in contrast to their counterparts’men. This is reasonable and acceptable because interventions to treat infertility, including injections, aspiration, intra-cytoplasmic injection, IVFs and medical treatments, are mostly applied to women and thus they may be exposed to physical and psychological complications resulting from interventions. Moreover, increased failures of IVFs attempts could lead to emotional disturbances,frustration and anxiety. Similar finding was reported by Pasch et al[36].A significant relationship was found between QoL and the duration of infertility among men. Infertile men for less than 3 years have a significant better QoL[35]. Previous studies reported decrease in the QoL as the infertility duration increases[22,35,37,38]. As a source of speculation, infertile men who live in a society, like that in the Gaza Strip, are in hurry to have children very earlier to satisfy themselves and their families and to overcome social pressure and stigma. However, as the infertility duration increases, men accept and accommodate to situation over the time. We found females’QoL depends on duration of infertility[39]. This is inconsistent with findings of Baghiani Moghadam et al[40].
This study had some limitations. Firstly, many independent factors which may affect QoL of infertile couples were not studied.Hereafter, further studies are recommended to exclude potential confounding factors. Secondly, we did not have the control group from fertile couples to compare the results. To better understand such effects, doing case control study with large sample size is recommended. Thirdly, the nature of cross-sectional design limits the causal relationship.
In conclusion, infertility affects the QoL of infertile Palestinian couples. Males’ total scores of FertiQoL and its subscales (emotion,mind/body, social, core, tolerability, and treatment) are higher than females’ scores. The mean score of total FertiQoL increases with better education, but decreases with increase of age, duration of marriage, duration of infertility and number of IVF attempts.
Conflict of interest statement
The research has no conflict of interest.
Acknowledgements
The authors are grateful to the head of infertility clinics for their permission to conduct the study. We are also thankful to women who agreed to participate. Many thanks for the midwifes who collected the data and to Mr. Mohammed Al Toul, from Palestine, for his cooperation and contribution in editing this manuscript.
Authors’ contributions
Suha Baloushah and Aymen Elsous designed the study. Aymen Elsous, Atef Masad and Ali Al-Derawi wrote the first draft. Suha Baloushah, Samira Barjasteh, and Soha Abou Eid participated in writing the manuscript. Atef Masad and Soha Abou Eid edited the manuscript before submission. Data analyzing was performed by Aymen Elsous. All authors read and approved the final version.
 Asian Pacific Journal of Reproduction2021年6期
Asian Pacific Journal of Reproduction2021年6期
- Asian Pacific Journal of Reproduction的其它文章
- Folic acid protects against fluoride-induced oxidative stress and testicular damage in rats
- Neutrophil-lymphocyte ratio in pregnancy-associated maternal complications:A review
- Protective effects of honey compound syrup on busulfan-induced azoospermia in male rats
- Association between eNOS gene promoter polymorphism (-786T>C) and idiopathic recurrent pregnancy loss in Iranian women
- Effects of L-arginine on preeclampsia risks and maternal and neonatal outcomes:A systematic review and meta-analysis