
Preoperative traction is a risk factor for osteonecrosis of femoral head in patients with stable femoral neck fractures
2021-11-12 08:35:46XinJuChengYuanYangXinLinSuJunLin
Life Research 2021年4期
Xin Ju,Cheng-Yuan Yang,Xin-Lin Su,Jun Lin
1Department of Orthopaedic Surgery,The First Affiliated Hospital of Soochow University,Suzhou,China.
Abstract To explore the relationship between preoperative traction and osteonecrosis of femoral head(ONFH)in patients with stable femoral neck fractures.Data from medical charts for 115 patients admitted to our institution with Garden II femoral neck fracture operated from January 2012 to December 2013 were extracted.Seven-year retrospective comparative study in the first affiliated hospital of Soochow University.Patients were divided into two groups by preoperative treatment:a preoperative traction group(group I)and a T-shaped shoe fixation group(group II).There were 14 patients lost to follow-up.101 patients with Garden II femoral neck fracture followed until July 2016 were available for complete analysis.Intervention:patients received skeletal traction or T-shaped shoe fixation preoperatively.All patients accepted internal fixation with multiple annulated screws.Main outcome measurements:the incidence of osteonecrosis of femoral head was analyzed based on preoperative traction,gender and implant removal.The average follow-up of these patients was 35 months(range,24-48 months).There was no implant failure or nonunion in our study.Nine patients(8.91%)had avascular necrosis.8(15.38%)patients in group I had osteonecrosis of femoral head,whereas only onepatient(2.04%)in group II had osteonecrosis of femoral head.Patients with preoperative traction had significantly higher incidence of osteonecrosis of femoral head compared with Tshaped shoe fixation(P = 0.032).No significant difference was found between the incidence of osteonecrosis of femoral head based on gender,age,injury-to-surgery interval time,implant removal or weight-bearing time.In patients with femoral neck fracture,preoperative traction may increase the incidence of osteonecrosis.Preoperative traction may not benefit patients with Garden II femoral neck fracture.The weight of traction may be a risk factor to osteonecrosis of femoral head.
Keywords:femoral neck fractures;preoperative traction;femoral head necrosis;incidence
Introduction
Femoral neck fractures are one of the most common fractures associated in adults with a high rate of mortality and disability[1-4].As a major complication,osteonecrosis severely affects the prognosis with an incidence as high as 20%-40%[5].The etiology of ipsilateral osteonecrosis of femoral head(ONFH)after femoral neck fractures is multifactorial.Femoral head ischemia is deemed to be the primary cause[6,7].Ischemia of the femoral head may be caused by multiple factors,such as disruption of the blood supply to the femoral head,obstruction of veins,and disturbance of microcirculation[8].Preoperative traction is widely used for pain relief and anatomical reduction in femoral neck fractures.It also does contributions to the correction in vascular anatomy[9].However,preoperative traction may not prevent further vascular damage,inversely,it could impair the blood perfusion to the femoral head,such as the medial circumflex femoral artery system[8,10].
The occurrence rate of segmental collapse due to osteonecrosis in displaced femoral neck fracture is about 16% to 30%,and the risk is half in non-displaced fracture[5].In 1961,Garden found that the incidence of avascular osteonecrosis increased with the amount of displacement of the femoral head[11].The Garden classification is widely utilized in proximal femoral fractures,and it is useful to predict the development of ONFH.The Garden classification includes four stages:① Stage I:incomplete stable fracture with impaction in valgus;② Stage II:complete,but non-displaced fracture;③ Stage III:completely displaced with varus with all three trabeculae disturbance;④ Stage IV:completely displaced with no contact between the fracture fragments.In the present cognition,Garden I and II femoral neck fractures are stable fractures and can be treated with internal fixation.Preoperative traction is widely used in femoral neck fractures.However,studies have shown that preoperative traction can,reduce blood supply of the femoral head[8].Garden II femoral neck fracture are stable femoral neck fractures with low incidence of ONFH.In Garden II femoral neck fractures,the impact of traction on blood supply would become more obvious.
In this research,we aimed to explore the relationship between preoperative traction and ONFH in patients with a stable femoral neck fracture.We carried out a four-year retrospective study to evaluate the influence of preoperative traction on the incidence of OFNH in patients with Garden II femoral neck fracture.
Materials and methods
Patients and treatments
Inclusion criteria.1)Patients admitted to our institution with Garden II femoral neck fracture.All the fractures were Garden II stage,according to the Garden classification[11].All patients were stabilized in situ.2)Patients treated with three cannulated screws.3)The follow-up duration was greater than 24 months.
Exclusion criteria.Non-surgical cases,cases treated with arthroplasty,cases with incomplete radiographic data sets,pathological fractures,previous hip fracture(same side or contralateral side),and rheumatoid arthritis.
Data from medical charts for 115 patients admitted to our institution with Garden II femoral neck fracture operated from January 2012 to December 2013 were extracted(Figure 1).There were 14 patients lost to follow-up.101 patients(51 males and 50 females)were available for complete analysis.The average age was 54 years(14-85 years).All patients got unilateral femoral neck fracture(56 in left,45 in right).Patients with femoral neck fractures were randomly divided into two groups:a preoperative traction group(group I)and a T-shaped shoe fixation group(group II).This study was permitted by the ethics committee of the First Affiliated Hospital of Soochow University(SDFYY252).
Preoperational treatment
Patients in group I accepted preoperative tibial tuberosity skeletal traction immediately after admission.The traction weight was less than 1/8 of the individual weight(Figure 2).The weight and duration of traction were counted.Skeletal traction was removed within 30 minutes before surgery in the operation room.Patients in group II accepted preoperative T-shaped shoe fixation immediately after admission.The T-shaped shoe was also removed within 30 minutes before surgery in the operation room.
Operational treatment
All patients accepted closed reduction by using minimal traction together with internal rotation.In our operations,the first needle is parallel to the neck shaft angle and close to the femoral distance in the positive X-ray,and at the center of the femoral neck in the lateral X-ray.The last two guide needles are 1.0-2.0 cm above the first needle,parallel to the first guide needle in the positive X-ray.These needle entrances are distributed as an equilateral triangle,and they are all located in the femoral neck.Cannulated screws were used for purpose of strong internal fixation.16 patients underwent implant removal due to their preference.However,the other 85 patients maintained their implants.
Evaluation
Clinical and radiographic evaluation was performed in 1,3,6,12 months postoperatively and then annually.Two independent observers(X.J.&X.W.)analyzed all clinical and radiographic evaluations.Necrosis of the femoral head was preliminarily estimated by clinical symptom such as hip pain,range of motion,and it was diagnosed by the plain film(X-ray)and magnetic resonance image[14,15].X-ray showed that there were density differences,calcification zones,cystic changes,and collapse of femoral head(Figure 3).Magnetic resonance image signal changes include subchondral band-like lesions(T1),or typical double-line signs(T2)(Figure 4).Figure 5 shows representative cases in these two groups.
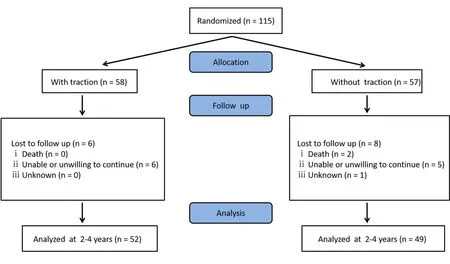
Figure 1.The workflow diagrams
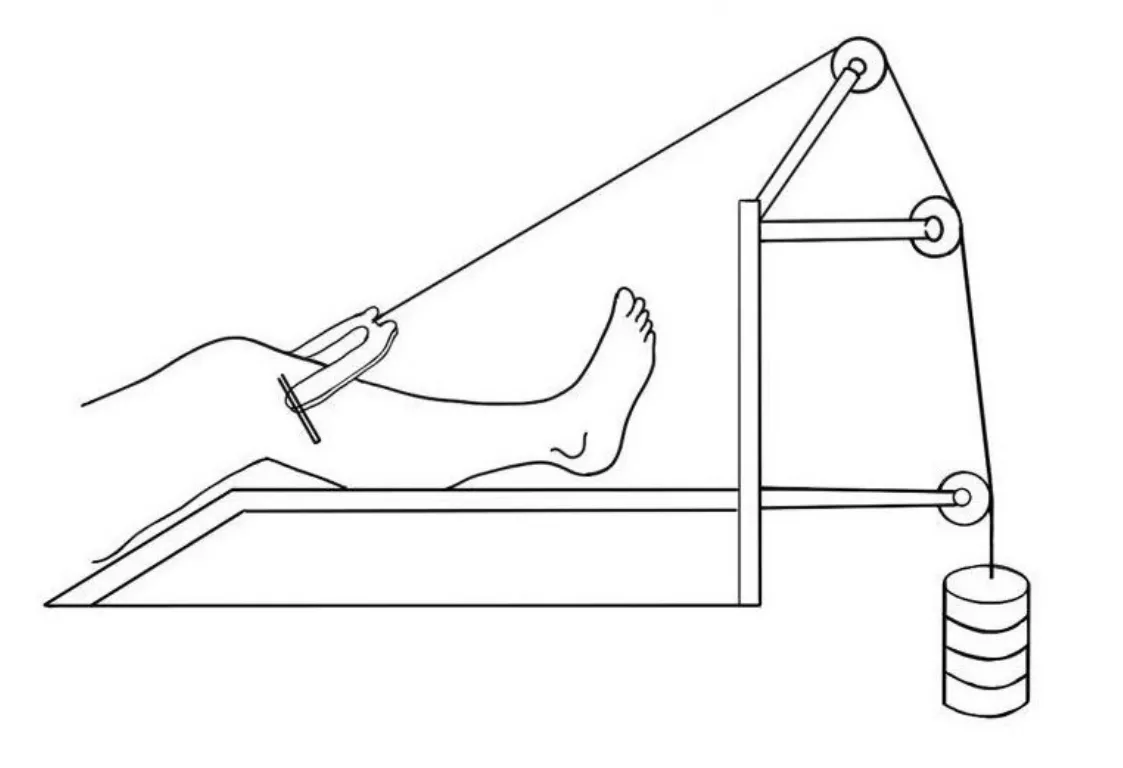
Figure 2.Schematic diagram of tibial tuberosity traction
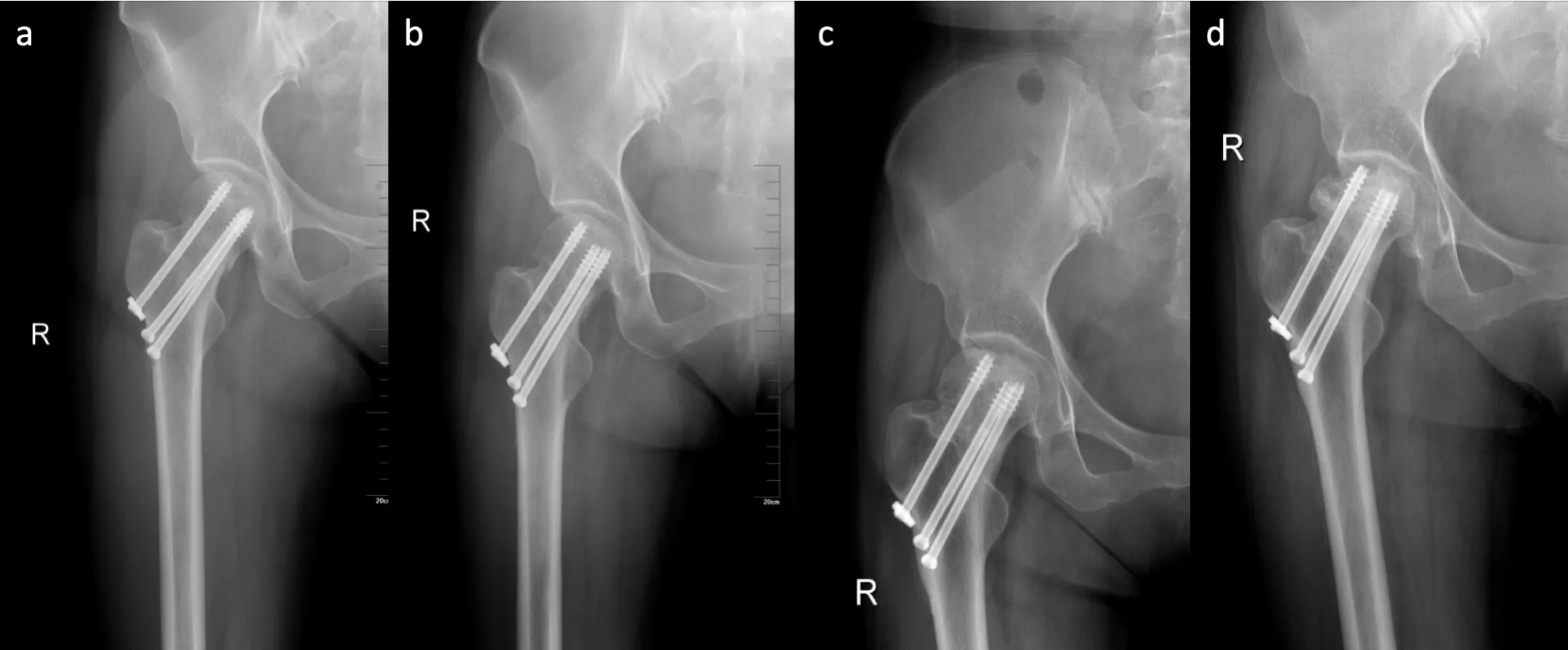
Figure 3.Typical X-ray images of femoral neck fracture.a)X-ray image at one day after surgery showed that the femoral neck fracture was well reduced and fixed.b)X-ray at 6 months after surgery showed good fracture healing.c)X-ray image at 1 year after surgery showed collapses of the top.d)X-ray image at 18 months after operations showed femoral head necrosis,accompanied by deformation and collapse of the femoral head.
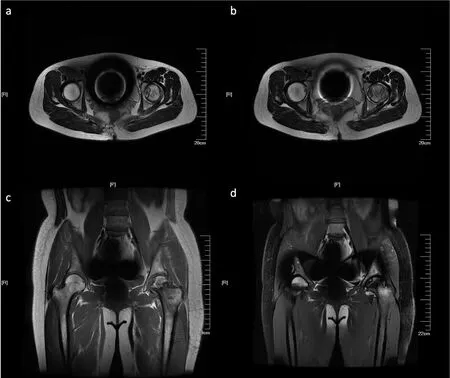
Figure 4.Typical magnetic resonance image signal changes of T1-weighted and T2-weighted images
Statistical Analysis
In date analysis,we used SPSS 18.0(SPSS,Inc,Chicago,Illinois).Statistical methods include chi-square test,and multivariate logistic regression analysis.In the group I,Fisher and Logistic regression analysis were used to test the towing weight and the towing time.AP-value of less than 0.05 is considered significant.
Table 1.Analysis of incidence of ONFH
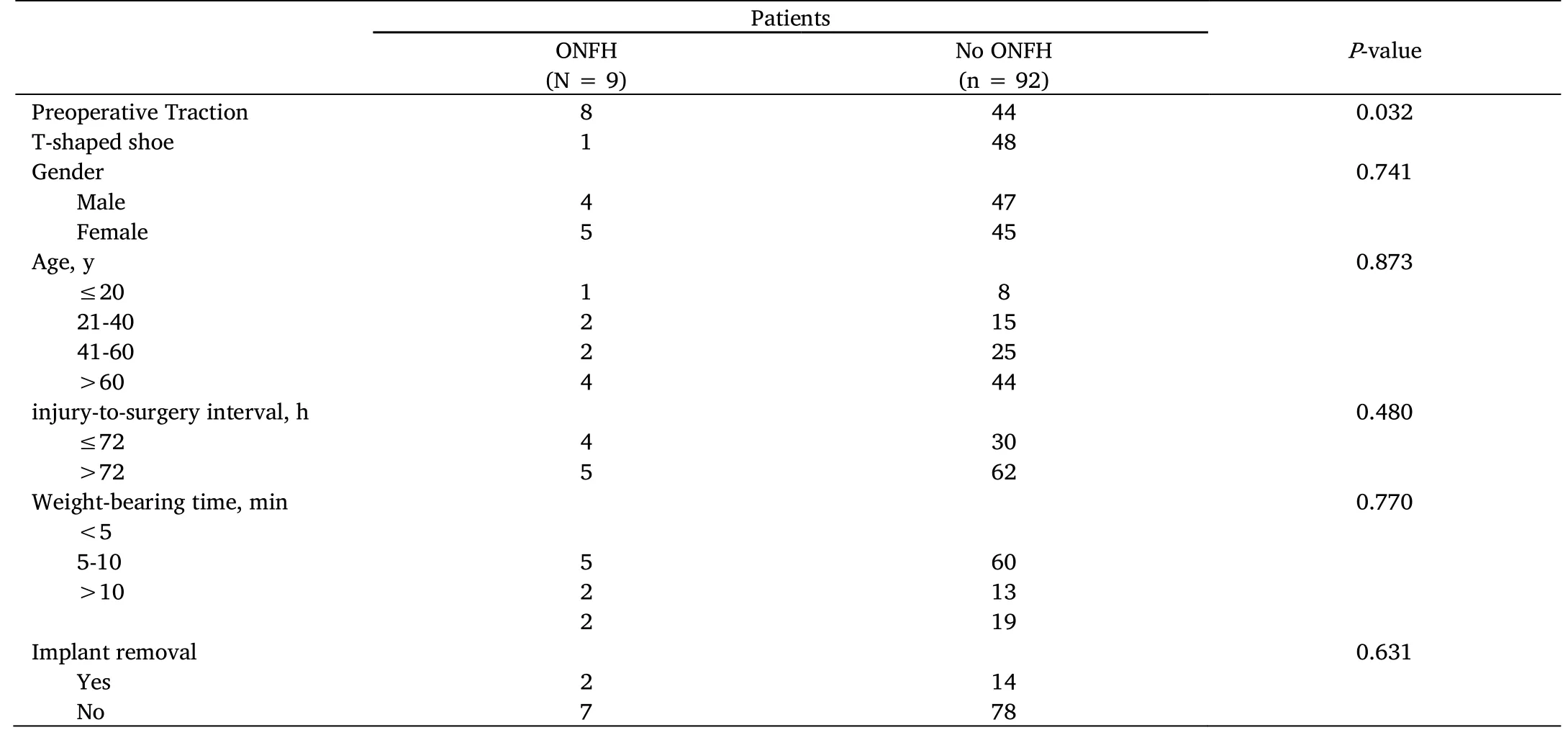
ONFH,osteonecrosis of femoral head.

Table 2.Incidence of ONFH in Patients with traction

Table 3.Multivariate analysis of incidence of ONFH in patients with traction
Results
The mean follow-up of these 101 patients was 35 months(24-48 months).No fractures of screws or implants were found.There was no nonunion in our study.A total of 9(8.91%)patients had avascular necrosis.8(15.38%)patients in group I had ONFH,whereas only one(2.04%)patient in group II had ONFH.At the final follow-up,only one patient with ONFH accepted total hip arthroplasty.No significant difference was found between the incidence of ONFH based on gender(P= 0.741),age(P= 0.873),injuryto-surgery interval(P= 0.480),weight-bearing time(P= 0.770)or implant removal(P= 0.631)in Table 1.Preoperative traction significantly increased the incidence of ONFH compared with T-shaped shoe fixation(P= 0.032).
In group I,the fisher test indicated that the weight(P= 0.043)of traction were significant effect factors of the incidence of ONFH(Table 2).However,the duration(P= 0.695)of traction may be less important.We use 72 hours as a cut-off point due to lack of precise date.Multivariate logistic regression analysis indicated the same result conformed with the Fisher test(Table 3).
Discussion
As is well-known,femoral neck fracture is a common cause of ONFH.The incidence of osteonecrosis is marked varied in numerous reports.The destruction of the blood supply with displaced fracture of the femoral neck could increase the incidence of ONFH,as high as 84%[16].After all,displacement of femoral neck fracture may be of great importance to the development of ONFH.Our study only included Garden II femoral neck fractures to minimize the influence of fracture displacement.
Femoral head ischemia is the basis of ONFH.Both disruption of arterial blood supply and the obstruction of venous drainage could result in femoral head ischemia.The blood supply and venous drainage could be damaged by the trauma that led to the femoral neck fracture.The displacement of femoral neck fracture will lead to direct injury to the superior retinacular vessel in the femoral head,and the superior retinacular vessel occupies about 1/2 to 2/3 of the blood supply of the femoral head[17].The blood supply from the junior retinacular vessel,the obturator artery,and the ligamentum teres artery is also affected.Besides the decreased blood supply in the femoral head,the tamponade effect of soft tissue may be another cause of ONFH[18,19].Increased intra-articular pressure caused by hemarthrosis has an influence on local blood circulation.Selective digital subtraction angiography indicated that the femoral neck fracture led to the injury of local blood circulation,including arterial blood supply,venous drainage,fewer vessel branches,inadequate perfusion.Moreover,the circulation time will be prolonged[8].
As one kind of traditional therapy for femoral neck fracture,skeletal traction is widely accepted.Strange-Vognsen[20]and Esenyel[21]have reported that traction was safe and effective in hip trauma as preoperative treatment.Following a femoral neck fracture,preoperative traction is usually applied to the injured limb for pain relief.It may be in effect in anatomical reduction,as well as the correction of blood circulation.However,some authors believe that the routine use of preoperative traction for hip fractures does not appear to have any benefit[22,23].There were very few reports about the disadvantages of traction in the femoral neck fraction.Xiao J[8]in 2012 demonstrated that,when traction is used in patients,the number of supporting arteries in the femoral head is significantly reduced.
Our research showed traction could increase the occurrence of ONFH.The author analyzed the reason into three aspects:1)blood perfusion is impaired;2)the intra-articular volume decreased and the capsule became tense with the internal rotation and extension of the injured limb,it leads to high intracapsular pressure;3)the shocks during the application of the traction are also taken into consideration,as most skeletal tractions in our country are hand-operated.
Our study aimed at Garden II femoral neck fractures.As a stable fraction,it minimized the influence of fracture displacement and reduced quality on the incidence of ONFH.In our study,patients with preoperative traction had a higher incidence of ONFH compared with the T-shaped shoe fixation group after Garden II femoral neck fracture.The weight of traction also had an influence on the incidence of ONFH.
In addition,the incidence of ONFH in the T-shaped shoes group was lower.T-shaped shoe fixation can stabilize the injured limb and relieve pain.Due to insufficient traction,T-shaped shoes have little effect on the blood perfusion of the femoral head and cannot play an anatomical reduction role.In Garden II femoral neck fractures without displacement,T-shaped shoes may be a more suitable preoperative treatment than traction
Conclusion
Following Garden II femoral neck fractures,patients with preoperative traction had a higher incidence of ONFH compared with patients with Tshaped shoe fixation.Preoperative traction may increase the incidence of ONFH after femoral neck fracture.Even though in our study,the duration of traction was not a significant risk factor,the influence of it could not be excluded.It is deserved to be chosen carefully as well as the weight of traction.T-shaped shoes fixation may be a more appropriate choice in Garden II femoral neck fractures.
- Life Research的其它文章
- The impact of the COVID-19 outbreak on Australia’s public health and medical industry in 2020
- Coronary heart disease-related fatigue:risk factors,assessment and treatments
- The mechanism of DDR genes in tumor progression
- Microbiota-gut-brain axis and major depressive disorder:implications for fecal microbiota transplantation therapy
- The therapeutic potential of stem cell therapy for myocardial infraction
- ZMYND10 downregulates cyclins B1 and D1 to arrest cell cycle by trimethylating lysine 9 on histone 3