
Lipid lowering in patients 75 years and older
2021-11-02 08:55:42UmidakhonMakhmudovaChristianSchulzeHarryDavisOliverWeingrtner
World Journal of Cardiology 2021年10期
Umidakhon Makhmudova,P Christian Schulze,Harry R Davis,Oliver Weingärtner
Umidakhon Makhmudova,P Christian Schulze,Oliver Weingärtner,Klinik für Innere Medizin I,Universitätsklinikum Jena,Jena 07747,Germany
Harry R Davis,Synergy Partners RD Solutions,Synergy Partners RD Solutions,Gaithersburg,MD 20850,United States
Abstract More than twenty years ago,knowledge about the importance of cholesterol absorption and the potential therapeutic effect of its inhibition led to the discovery and clinical application of the first and only cholesterol absorption inhibitor to date - ezetimibe.Since then,ezetimibe has become a well-recognized player in lipid-lowering therapy.Recent findings of IMPROVE-IT and EWTOPIA 75 imply that elderly patients over the age of 75 years in particular benefit from ezetimibe.This review summarizes the evidence,discusses the possible underlying pathophysiological mechanisms and calls for a change in future dyslipidemia guidelines.
Key Words:Cholesterol;Cholesterol absorption;Cholesterol synthesis;Ezetimibe;Elderly
INTRODUCTION
Aging is a risk factor for cardiovascular morbidity,as the prevalence of atherosclerosis,myocardial infarction,and stroke increases with age[1].Among all the physiological alterations that occur during the lifespan of a human being,changes in cholesterol metabolism are among the most important.Total cholesterol levels increase beginning from age 18-19 in men and age 20-21 in women and reach their climax at 50-51 and 56-57 years of age,respectively[2].Although the concentration of endogenously synthesized cholesterol exceeds the amount of exogenous dietary cholesterol in the bloodstream,the inhibition of cholesterol absorption by ezetimibe reduces both low density lipoprotein (LDL)-c levels and the occurrence of cardiovascular events[3-5].The particular benefit of ezetimibe treatment in regard to hard cardiovascular outcomes in patient populations over 75 years of age was only recently demonstrated in large cardiovascular outcome trials,such as IMPROVE-IT[6] (secondary prevention)and EWTOPIA 75[7] (primary prevention).
CHOLESTEROL METABOLISM
Cholesterol is one of the key components of the cell membrane and a precursor of steroid hormones,bile acids and vitamin D.Plasma cholesterol levels are regulated by three factors:Dietary absorption,endogenous biosynthesis in the liver and bile acids that are reabsorbed in the small intestine.Endogenous cholesterol synthesis begins with the 18-step formation of mevalonate through its conversion by HMG (3-hydroxy-3-methyl-glutaryl-) CoA reductase,which is a target of statin therapy,and ends with the 19-step synthesis of cholesterol from lanosterol.This cascade of reactions occurs in all nucleated cells and is catalyzed by a diversity of enzymes.Late precursors of cholesterol,such as squalene,cholestanol,desmosterol and lathosterol,are traditionally used as cholesterol synthesis markers.Due to its structure,cholesterol cannot be easily transported to tissues.Therefore,it is transported by lipoproteins,which contain triglycerides and cholesterol in their cores and apolipoproteins on their surface.Very low-density lipoprotein is synthesized in the liver and hydrolyzed to LDL in two steps.LDL is the major transporter of cholesterol in the plasma.
In addition to be endogenously synthesized,cholesterol is absorbed from the diet.In the small intestine,esterified cholesterol is converted to free cholesterol,which is absorbedviatransport and endocytosis by NPC1L1 (Niemann-Pick C1-Like 1).In enterocytes,chylomicrons are formed from cholesterol,phospholipids,and triacylglycerol by apoprotein B48.Chylomicrons are transportedviathe lymphatic system to the bloodstream,where they deliver fatty acids to peripheral tissues and are eventually degraded by the liver.Moreover,nonesterified plant sterols and “excess cholesterol” are excreted back into the small intestineviathe ATP-binding cassette transporter (ABCG5/G8) heterodimer.This results in large differences between cholesterol and plant sterol concentrations in the bloodstream,with plasma cholesterol levels being approximately 1000-fold higher than plant sterol levels.
PATHOPHYSIOLOGIC ASPECTS OF CHOLESTEROL METABOLISM IN AGING
The increase in LDL-c levels with age can be explained by several factors:A decrease in LDL receptor levels,an increase in the levels of apoB-100 in the liver and serum[8],an increase in cholesterol absorption,and a decrease in bile acid synthesis[9].
Animal studies have demonstrated that the cholesterol absorption rate increases with age[10,11].According to Duanet al[11],cholesterol absorption in older mice(measured by the plasma dual isotope ratio method) is higher than that in younger mice,which is mechanistically explained by an increase in NPC1L1 mRNA expression with aging.Interestingly,the expression of ABCG5/G8,a transporter that pumps plant sterols back into the intestinal lumen and thus decreases plant sterol concentrations in the plasma,is negatively correlated with aging[11].
Another important age-related alteration is a reduction in CYP7A1 expression,an enzyme involved in bile acid synthesis.This leads to a decrease in bile acid synthesis,which in turn results in a lower cholesterol utilization rate[9].
Unfortunately,the number of human studies in this context is very limited.One study reported a positive correlation between cholesterol synthesis marker levels and aging in a Northern Italian population.In that study,cholesterol absorption marker levels were also elevated in elderly individuals but not in patients with gallstones[12](Figure 1).
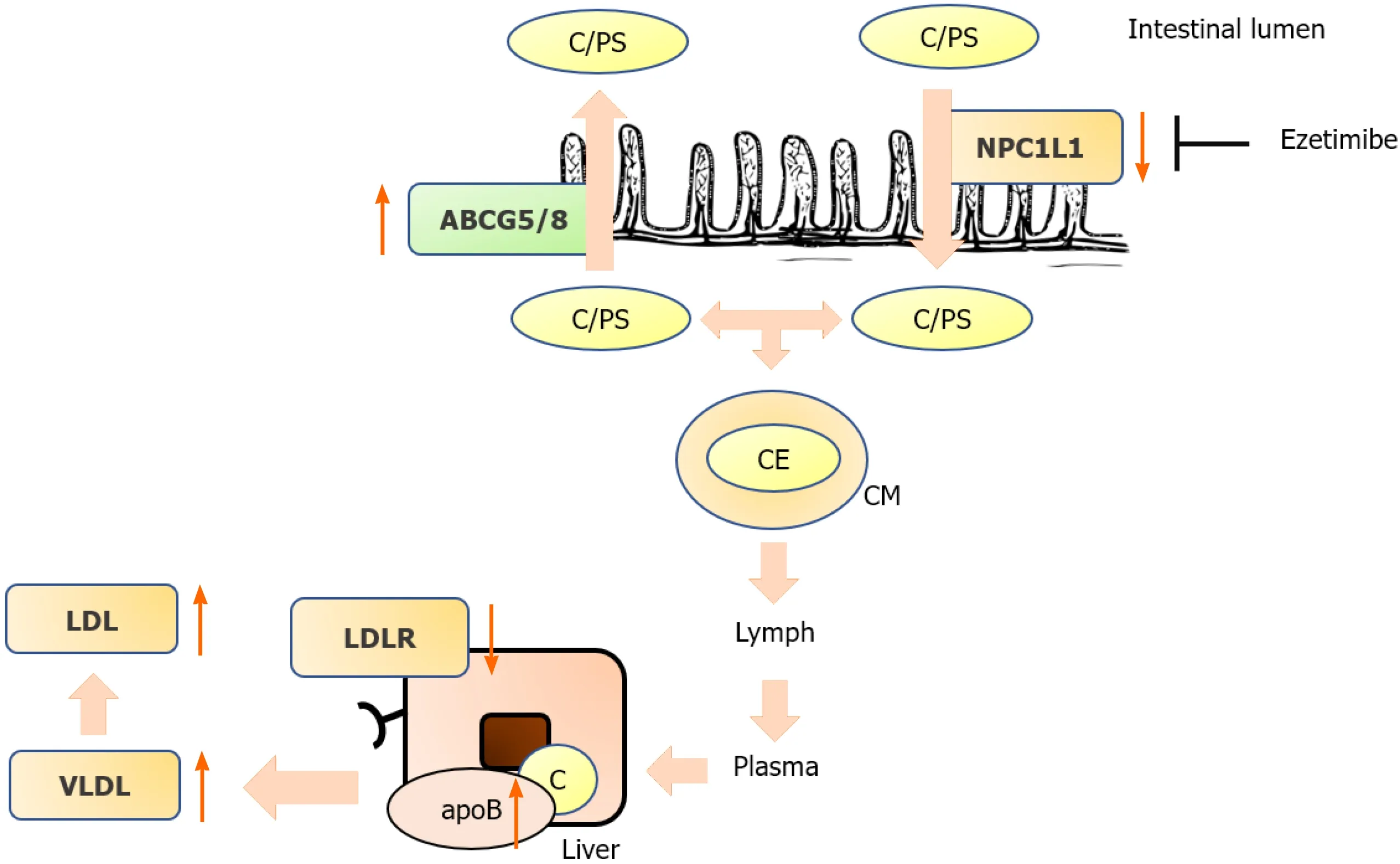
Figure 1 Alteration of cholesterol metabolism during lifetime.
METHODS OF CHOLESTEROL ABSORPTION MEASUREMENT
Methods to quantify cholesterol absorption were established as early as 1960[13,14].Almost all of the early methods were based on isotope labeling of plasma and fecal probes:Cholesterol balance,single-dose isotopic feeding,dual isotope plasma ratio,continuous isotope feeding,and intestinal perfusion[13].Another validated method that does not require isotope feeding is the measurement of the ratio of plant sterol levels (campesterol and sitosterol) and cholestanol levels (metabolite of cholesterol),which is performed mainlyviahigh-performance liquid chromatography.Plant sterol concentrations have been shown in several studies to be markers of cholesterol absorption[15].
INHIBITION OF CHOLESTEROL ABSORPTION IN ELDERLY INDIVIDUALS
Early studies
A landmark study addressing the importance of cholesterol metabolism in elderly patients was the DEBATE-Study[16].Strandberg and colleagues conducted a prospective cohort study of home-dwelling elderly individuals to assess the prognostic value of markers of cholesterol metabolism (absorptionvssynthesis).They found that low cholesterol absorption in individuals older than 75 years of age was associated with fewer cardiovascular events and better survival.In that study,the levels of markers of cholesterol synthesis were negatively associated with cardiovascular outcomes[16].Strandberg and colleagues speculated that lower cholesterol absorption was associated with better prognosis since these individuals had a lower cholesterol burden during their lifespan.On the other hand,the worse prognosis may have also been due to increased plant sterol absorption.Similar results were reported by our group in elderly patients with aortic stenosis and patients with diabetes mellitus[17,18].
Statins
Statins inhibit 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase in the liver,thus preventing the formation of mevalonate,which determines the rate of endogenous cholesterol synthesis[19].Statins reduce LDL-c levels by up to 60%depending on the specific drug and dose (rosuvastatin is the most potent statin,as 40 mg of rosuvastatin reduces LDL-c levels by 55%)[20].Although statins are the cornerstone of lipid-lowering therapy,target goal attainment with statin monotherapy is often unsatisfactory.In JUPITER (Justification for the Use of Statin in Prevention:An Intervention Trial Evaluating Rosuvastatin),approximately 10% of the patients showed no change in LDL-c levels,and over 40% had a LDL-c level reduction below 50%[21].Several loci were identified by genome-wide association studies to be responsible for “nonresponsiveness” to statin therapy[21,22].On the other hand,ezetimibe treatment is particularly effective in these patients since low endogenous synthesis is associated with high cholesterol absorption[23,24].
The secondary analysis of ALLHAT-LTT demonstrated that statins (pravastatin)conveyed no benefit in a primary prevention setting.Moreover,there was a nonsignificant trend toward increased all-cause mortality in the pravastatin group vs.the placebo group.PROSPER (PROspective Study of Pravastatin in the Elderly at Risk)evaluated hard cardiovascular outcomes in pravastatin-vsplacebo-treated patients.Pravastatin reduced primary endpoints (a composite of coronary death,nonfatal myocardial infarction,and nonfatal stroke occurrence) after 3 years of follow-up.The subgroup analysis in the study revealed that this effect was stronger among those with established cardiovascular disease than among those without cardiovascular diseases,implying that statins are less effective in a primary prevention setting.However,no significant difference was observed in the interaction test between groups.Moreover,in pravastatin-treated patients,the incidence of newly diagnosed cancer was 25%higher than in the placebo group,although a meta-analysis did not show any significant association with cancer[25].
Ezetimibe
Ezetimibe targets NPC1L1 in the small intestine,resulting in the inhibition of cholesterol and plant sterol absorption.In humans,ezetimibe also inhibits hepatic NPC1L1 to prevent reabsorption of cholesterol and plant sterols from the bile and increases their excretion.Ezetimibe is metabolized to ezetimibe-glucuronide,which is also a potent inhibitor of NPC1L1.The maximal concentration is reached 1-2 h after oral administration,and it has a terminal half-life of 22 h[3].Ezetimibe lowers LDL-c levels by approximately 20%[3,4].PRECISE-IVUS demonstrated that ezetimibe in combination with atorvastatin resulted in greater coronary plaque regression than atorvastatin monotherapy in patients with coronary artery disease[26].The SHARP trial demonstrated that the combination of statins and ezetimibe reduced LDL-c levels and cardiovascular outcomes in patients with chronic kidney disease[27].According to the current ESC/EAS guidelines,ezetimibe is recommended as an adjuvant to statin therapy when LDL-c goals cannot be achieved by statin monotherapy[28].
A post hoc analysis of the Scandinavian Simvastatin Survival Study (4S) suggested that patients with high cholesterol absorption and low cholesterol synthesis did not benefit from statins in terms of cardiovascular event reduction[29].HIJ-Proper,on the other hand,demonstrated that patients with high cholesterol absorption benefited from the addition of ezetimibe in terms of cardiovascular event reduction,whereas patients with low cholesterol absorption did not[30].
IMPROVE-IT secondary analysis–addition of ezetimibe to a statin in elderly patients after acute coronary syndrome
IMPROVE-IT demonstrated for the first time that ezetimibe,a nonstatin drug,reduces LDL-c levels and hard cardiovascular outcomes[5].In a recent secondary analysis,the outcomes of IMPROVE-IT were analyzed according to age.Interestingly,in patients older than 75 years of age,ezetimibe treatment was much more effective in reducing cardiovascular events.In patients over 75 years of age,the number “needed to treat”was 11,whereas it was 125 in patients younger than 75 years of age[6].These findings illustrate the preventive capacity of adding a cholesterol absorption inhibitor in elderly individuals over 75 years of age[31].
EWTOPIA 75–ezetimibe in the primary prevention of cardiovascular disease in elderly individuals
The EWTOPIA 75 study is a prospective,double-blind,placebo-controlled randomized trial that was conducted in Japan and demonstrated the benefit of ezetimibe in elderly patients without a history of coronary artery disease[7].In this primary prevention trial,ezetimibe reduced both LDL-C levels and hard cardiovascular outcomes.This further adds to the notion that individuals over 75 years of age with elevated cholesterol levels benefit in particular from ezetimibe treatment[32].This is of particular interest since all statin trials of primary prevention in patients over 75 years of age failed to reduce cardiovascular events[25,33].
Possible role of plant sterols
In a recently published large-scale genetic analysis of over 1 million individuals with and without cardiovascular diseases,Helgadottir and colleagues reported genetic variants of ABCG5/G8 and NPC1L1 that increase plasma plant sterol levels,and plasma cholesterol levels have a greater impact on cardiovascular risk than the levels of other lipid genes that increase only serum cholesterol levels (LDL-c receptor,HMGCoA-reductase,apoB,etc.).Genes that increased non-HDL cholesterol levels by 1 mmol/L and also increased serum plant sterol levels increased cardiovascular risk 2.0-fold.However,genes that increased serum non-HDL cholesterol levels by 1 mmol/L but had no impact on serum plant sterol levels increased cardiovascular risk only 1.5-fold[34].These findings are important since they demonstrate that plant sterols “per se” are atherogenic.On the basis of these findings,determination of the levels of markers of cholesterol metabolism,such as campesterol,sitosterol and lathosterol,should play a more important role in future cardiovascular risk stratification and a more personalized and individualized treatment approach for hyperlipidemia[24,35].As early as 2016,we suggested evaluating the ratio of cholesterol synthesis and absorption in IMPROVE-IT[36].This analysis is under way,as assured by the TIMI Study group,and will provide important mechanistic insights[37].
CONCLUSION
Evidence from animal studies and human trials indicates that cholesterol and plant sterol absorption increase with age.Findings from large-scale prospective,randomized trials on primary and secondary prevention demonstrate that patients over 75 years of age benefit in particular from the addition of a cholesterol absorption inhibitor,such as ezetimibe.Therefore,ezetimibe should be the lipid-lowering drug of choice in patients 75 years and older.
 World Journal of Cardiology2021年10期
World Journal of Cardiology2021年10期
- World Journal of Cardiology的其它文章
- Cardiac involvement in hydrocarbon inhalant toxicity—role of cardiac magnetic resonance imaging:A case report
- Cardiovascular efficacy and safety of dipeptidyl peptidase-4 inhibitors:A meta-analysis of cardiovascular outcome trials
- Patent hemostasis of radial artery:Comparison of two methods
- Elderly patients with non-cardiac admissions and elevated highsensitivity troponin:the prognostic value of renal function
- Coronavirus and cardiovascular manifestations- getting to the heart of the matter
- Artificial intelligence and machine learning in cardiovascular computed tomography