
In-Hospital Cardiac Arrest after Emotional Stress in a Patient Hospitalized with Gastrointestinal Symptoms and Chronic Anxiety Disorder
2021-10-22 08:05:00ToTuJingLiZhenfeiFngXinqunHuJinjunTngYnshuZhoLingTngndShenghuZhou
To Tu,Jing Li,Zhenfei Fng,Xinqun Hu,Jinjun Tng,Ynshu Zho,Ling Tng nd Shenghu Zhou
Department of Cardiovascular Medicine,The Second Xiangya Hospital of Central South University,No.139 Middle Renmin Road,Changsha City,410011 Hunan,China
Abstract Background:We report an acute emotional stress–induced in-hospital cardiac arrest in a patient admitted with gastrointestinal symptoms after experiencing chronic anxiety disorder.Case Presentation:The patient was admitted to the Second Xiangya Hospital,Central South University,with gastrointestinal symptoms and chronic anxiety disorder,and experienced cardiac arrest during hospitalization after acute emotional stress.Malignant ventricular tachycardia and cardiogenic shock were evidenced in this patient after the acute emotional stress.Severe and extensive coronary spasm was confirmed by emergency coronary angiography,and coronary spasm was relieved by intracoronary injection of nitroglycerin.The patient recovered from myocardial infarction with nonobstructive coronary arteries.However,the patient developed acute kidney dysfunction and severe pulmonary infection and eventually died of respiratory circulatory failure on the ninth day after the successful rescue.Conclusions:Acute emotional stress on top of chronic anxiety disorder in patients hospitalized for noncardiovascular reasons might lead to the development of life-threatening cardiovascular diseases,including coronary artery spasm and myocardial infarction with nonobstructive coronary arteries.Psychological management is of importance to improve the outcome of these patients.
Keywords:Myocardial infarction with nonobstructive coronary arteries;coronary artery spasm;psycho-emotional disorders;cardiac arrest
Introduction
Emotional stress can enhance sympathetic activity,leading to endothelial dysfunction and vascular smooth muscle hyperreactivity,and can sometimes even induce acute coronary artery spasm(CAS)[1].CAS may be the underlying mechanism in up to 10% of cases of sudden cardiac death in patients with acute coronary syndrome(ACS)[2].Psychoemotional disorders and CAS are the common pathological causes of myocardial infarction with nonobstructive coronary arteries(MINOCA)[3].Intervention for psycho-emotional disorders was shown to be the medical target for both prevention and recovery in some patients with MINOCA[4].
Gastrointestinal dysfunction is a common concomitant symptom in patients with chronic emotional disorders[5].However,the cardiovascular risk is often overlooked in these hospitalized patients because of gastrointestinal symptoms,accompanied by psychological problems.Herein,we report a relevant case of a middle-aged patient with chronic anxiety disorder hospitalized with gastrointestinal symptoms who experienced cardiac arrest during hospitalization after acute emotional stress.
Case Presentation
A 53-year-old man was admitted to the Department of Gastroenterology of our hospital with a 6-month history ofintermittent black stool and fatigue,aggravated for 3 days.He had also experienced generalized anxiety disorder,hypertension,and intermittent chest pain for 7 months before admission.He had a suspected diagnosis of coronary heart disease and had been treated with rosuvastatin and trimetazidine for 7 mouths.He had no history of diabetes,hyperlipemia,or any other cardiovascular risk factor.He was a long-term smoker(around 30 years)and had quit smoking 7 months before hospitalization.He had no cocaine consumption history and no family history of sudden cardiac death.The patient had received no antianxiety drugs for personal reasons.
On admission,his blood pressure was 116/72 mmHg and his heart rate was 72 beats per minute.His heart,lung,and abdomen physical examination results were normal.His liver function test results,renal function test results,electrolyte levels(serum potassium 4.55 mmol/L,serum magnesium 0.93mmol/L,serum sodium 137.6 mmol/L,and serum calcium 2.11 mmol/L),myocardial enzyme level,and troponin T level at admission were normal.His hemoglobin level was reduced(87 g/L),and an occult blood test was positive.Standard 12-lead electrocardiogram(ECG)demonstrated borderline T wave changes in lateral leads(V5,V6,I,aVL),with no features of ST-segment elevation myocardial infarction(Figure 1A).
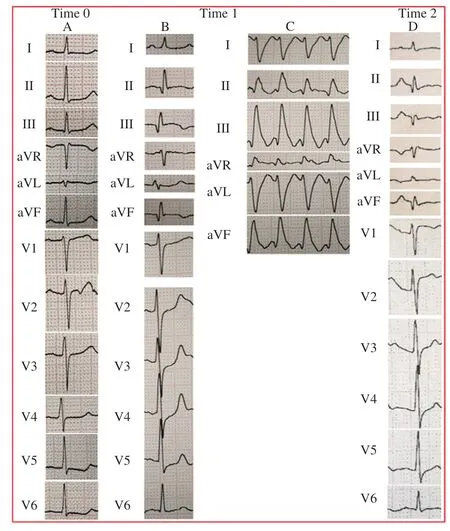
Figure 1 Electrocardiogram(ECG).
He was treated initially with pantoprazole,sucralfate,and nifedipine.Continuous bleeding of the digestive tract was controlled on the next morning after admission.After breakfast,he suddenly experienced very strong emotional stress owing to some trivial family matters.He asked the physician in charge of his medication to “ attenuate” his discomfort,including severe chest pain and shortness of breath.Emergency management was immediately initiated,and the ECG showed ST elevations in inferior leads(II,III,aVF),depression in anterior leads(V2–V5),and an abnormal Q wave in inferior leads(II,III,aVF);see Figure 1B.His symptoms could not be relieved by oxygen therapy and nitroglycerin.A few minutes later,the patient became unconsciousness,his blood pressure dropped to shock status,and ECG monitoring evidenced ventricular fibrillation following transient ventricular tachycardia(Figure 1C).During the 90-minute cardiopulmonary resuscitation period,the patient received unsynchronized cardioversion five times,mechanical ventilation,large doses of vasoactive agents,and continuous intravenous norepinephrine infusion(0.5 μ g/kg · min).The patient’s vital signs were finally restored,and his blood pressure and heart rate recovered to 101/70 mmHg and 97 beats per minute,respectively.The high-sensitivity troponin T value was 2,518 pg/mL(0.01–14.00 pg/mL is the normal reference range for troponin instrument detection)immediately after recovery.Coronary angiography was performed immediately after resuscitation and evidenced diffuse arterial narrowing in three coronary arteries:the left anterior descending coronary artery(95% stenosis,TIMI grade 1),the left circumf lex artery(95% stenosis,TIMI grade 2),and the right coronary artery(95% stenosis,TIMI grade 1);see Figure 2.Ventriculography showed global left ventricular hypokinesia,and wall motion abnormality was more significant in the mid wall(Figure 3A;left ventricular ejection fraction[LVEF]33%).After intracoronary injection of nitroglycerin,spasm of all the coronary arteries was resolved completely with TIMI grade 2–3(Figure 2).Bedside transthoracic echocardiography revealed severe reduced left ventricular function(LVEF 33.4%;Figure 3B).After the successful rescue,symptomatic and supportive treatment was continued.Norepinephrine was used to stabilize blood pressure,nitroglycerin to reduce vasospasm,metoprolol and amiodarone to control ventricular arrhythmia,piperacillin/tazobactam and meropenem to prevent infection,esomeprazole to inhibit gastric acid,and hemodialysis for acute kidney failure.Despite use of a series of treatment methods and the left ventricular motion being slightly improved 7 days later(LVEF 39.7%;Figure 3B),the patient failed to regain consciousness.Ultimately,the patient died of respiratory circulatory failure 9 days later due to cardiac arrest caused by acute kidney failure and severe pulmonary infection.
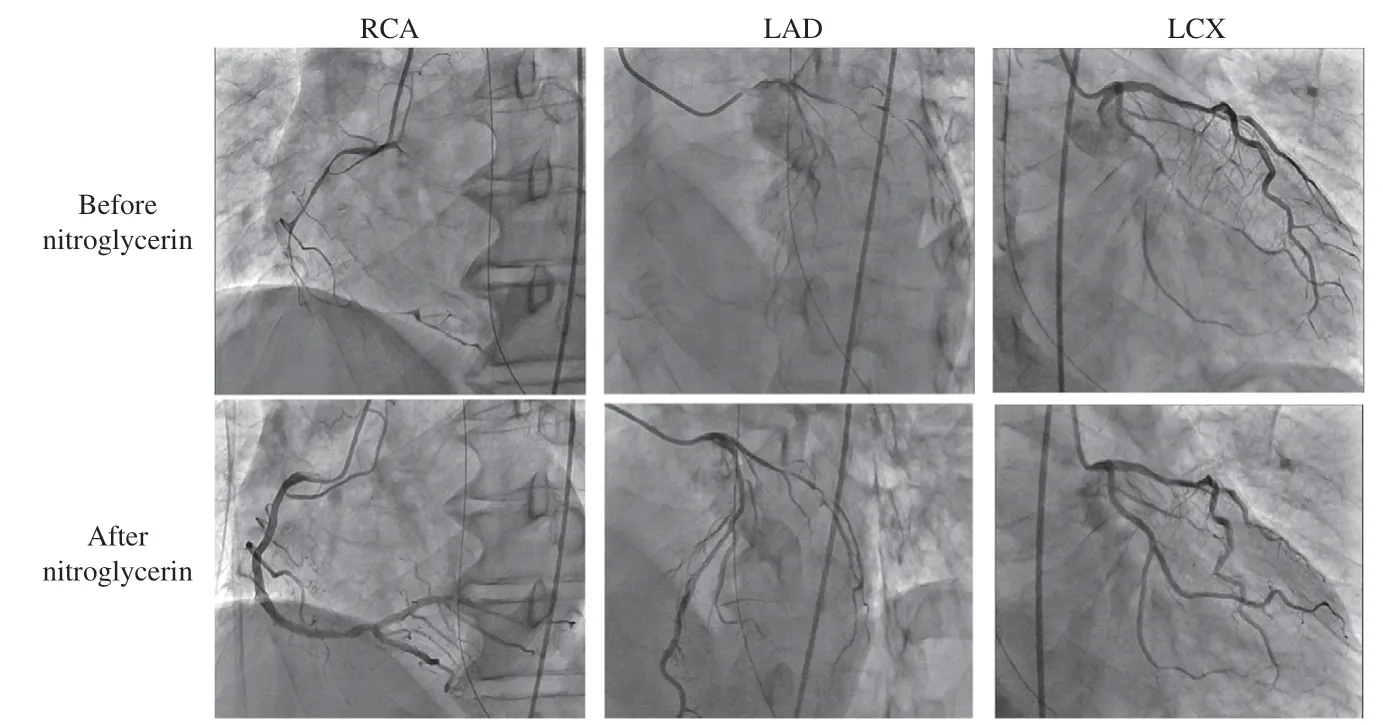
Figure 2 Coronary Angiography.
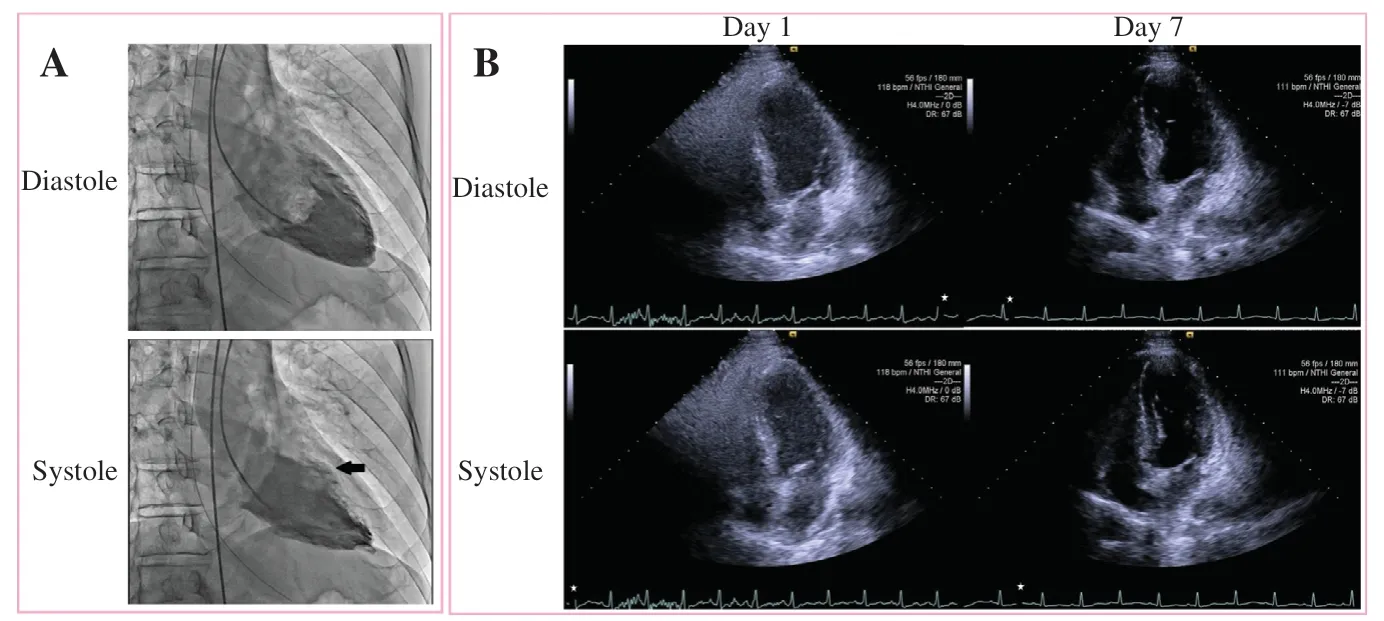
Figure 3 Ventriculography and Bedside Transthoracic Echocardiography.
Discussion
The present case highlights the important clinical impact on cardiovascular outcome of psychological stress in a hospitalized patient with noncardiovascular symptoms.
Coronary angiography after resuscitation in this patient revealed typical signs of MINOCA,characterized by CAS[6,7].In line with a literature report,the underlying reason for CAS was the sudden emotional stress,and CAS could be relieved by intracoronary injection of nitroglycerin[8].However,the acute emotional stress in our patient occurred on top of chronic psychological disorder.The joint effects of chronic and acute emotional stress might be the potential mechanism for the disease progress and poor outcome(malignant ventricular tachycardia and extensive and reversible CAS,followed by death due to respiratory circulatory failure 9 days after successful resuscitation).The mechanism by which emotional problems lead to cardiac events is possibly related to burst release of stress hormones,including catecholamine.
Although the LVEfincreased slightly from 33.4% to 39.7% after resuscitation after reversible CAS,the patient died of respiratory circulatory failure 9 days later in the presence of new-onset acute kidney failure and severe pulmonary infection.The present patient was admitted to the Department of Gastroenterology because of digestive symptoms.By reviewing the case afterwards,we found that the psychological problems and the potential risk of cardiovascular burden were not given enough attention by the managing medical professionals,despite the existing cardiovascular risk factors,including the long-term smoking history of the patient.
Psycho-emotional disorders are closely related to the risk of CAS and MINOCA[8].The mechanism by which CAS develops in patients with a history of anxiety or depression seems multifactorial.Endothelial dysfunction and elevated levels of proinf lammatory cytokines have been suggested in patients with psychological problems and patients with CAS[8].Autonomic dysfunction with disruption of the neuroendocrine axis and inf lammation/oxidative stress may jointly lead to a state of altered smooth muscle reactivity that predisposes to CAS[8].Meanwhile,another study indicated that the presence of psychiatric illnesses was higher in patients with MINOCA than in patients with myocardial infarction with obstructive coronary arteries.Such a relationship remained after the exclusion of takotsubo cardiomyopathy[3].These findings can be explained by the effects of emotions on adrenergic regulation and its relationship with endothelium function[9].For our patient,7 months of anxiety formed the basis of CAS,and the acute emotional stress became the last straw to break the camel’s back.
Conclusion
In conclusion,this case report highlights the importance of managing chronic and acute anxiety disorders in a patient hospitalized for noncardiovascular reasons,especially for patients with potential cardiovascular risks,to prevent the development of CAS and MINOCA.
Acknowledgement
None.
Conf licts ofinterest
The authors declare that they have no conf licts ofinterest.
Financial Support
None to declare.
 Cardiovascular Innovations and Applications2021年3期
Cardiovascular Innovations and Applications2021年3期
- Cardiovascular Innovations and Applications的其它文章
- Running with Face Masks or Respirators Can Be Detrimental to the Respiratory and Cardiovascular Systems
- CTO(Chronic Total Occlusion)
- Junctional Pacemaker May Replace the Sinoatrial Node
- A Patient with Atezolizumab-Induced Autoimmune Diabetes Mellitus Presenting with Diabetic Ketoacidosis
- Clinical Characteristics and Durations of Hospitalized Patients with COVID-19 in Beijing:A Retrospective Cohort Study
- Similarities and Differences of CT Features between COVID-19 Pneumonia and Heart Failure