
Clinical Characteristics and Durations of Hospitalized Patients with COVID-19 in Beijing:A Retrospective Cohort Study
2021-10-22 08:04:58WenZhaoXiangyiZhaNingWangDongzengLiAixinLiandShikaiYu
Wen Zhao,Xiangyi Zha,Ning Wang,Dongzeng Li,Aixin Li and Shikai Yu
1 Department of Obstetrics,Beijing YouAn Hospital,Capital Medical University,100069 Beijing,China
2 Hangzhou Dianzi University,Hangzhou,310018 Zhejiang,China
3 Medical Examination Center,Affiliated Hangzhou First People’s Hospital,Zhejiang University School of Medicine,Hangzhou,310006 Zhejiang,China
4 Department ofinfection Diseases,Beijing YouAn Hospital,Capital Medical University,100069 Beijing,China
5 Department of Cardiology,Shanghai Tenth People’s Hospital,Tongji University School of Medicine,200072 Shanghai,China
Abstract Objective:To provide information on clinical characteristics and different durations of COVID-19 and to identify the potential risk factors for longer hospitalization of patients with COVID-19.Methods:In this retrospective study,we enrolled 77 patients(age 52 ± 20 years;44.2% males)with laboratoryconfirmed COVID-19 admitted to Beijing YouAn Hospital between January 21 and February 8,2020.Epidemiological,clinical,and radiological data on admission were collected;complications and outcomes were followed up until February 26,2020.The end point of the study was discharge alive within 2 weeks.Cox proportional-hazards regression was performed to identify risk factors for longer hospitalization.Results:Of 77 patients,there were 34 males(44.2%),24(31.2%)with comorbidities,22(28.6%)with lymphopenia,20(26.0%)with severe COVID-19,and 28(36.4%)with complications.By the end of follow-up,64 patients(83.1%)were discharged home,eight remained in hospital,and five had died.Thirty-six patients(46.8%)were discharged within 14 days and thus reached the study end point,including 34 of the 57 patients with nonsevere COVID-19(59.6%)and two of the 20 patients with severe COVID-19(10%).The overall cumulative probability of the end point was 48.3%.Hospital length of stay and the duration from exposure to discharge for the 64 discharged patients were 13(10–16.5)days and 23(18–24.5)days,respectively.A multivariable stepwise Cox regression model showed that bilateral pneumonia on CT scan,shorter time from illness onset to admission,severity of disease,and lymphopenia were independently associated with longer hospitalization.Conclusions:COVID-19 has a shorter duration of disease and hospital length of stay than severe acute respiratory syndrome.Bilateral pneumonia on CT scan,shorter period from illness onset to admission,lymphopenia,and severity of disease are the risk factors for longer hospitalization of patients with COVID-19.
Keywords:COVID-19;SARS-CoV-2;Duration of disease
Introduction
Since it started in December 2019,the outbreak of severe acute respiratory syndrome coronavirus 2(SARS-CoV-2)infection has attracted the attention of the whole world.Although the outbreak is nearly restrained after enormous efforts made and pains taken by mankind,however,the virus has never gone far away and is ready to bounce back at any time.Undoubtedly,preparedness for the impact of the virus is necessary and critically important,especially for those countries at high risk but with relatively weak public health systems.Under these circumstances,the experience of containment in peer countries and territories and comprehensive research on COVID-19 would undoubtedly help.Many studies have generally reported the epidemiological features,clinical characteristics,and virology of SARSCoV-2 infection[1–7].However,the features and characteristics of the disease may be different at different locations and over time[8],since the pathogen,SARS-CoV-2,may evolve after transmission[9].It is thus important to closely follow these changes for better containment and management of COVID-19.In addition,the durations of COVID-19(e.g.,the average time from exposure to recovery and hospitalization duration),which are important for understanding this disease and useful for preparedness and correct response to COVID-19,were not reported,mainly because most patients included in previous studies remained in hospital as the study was being done.Here we present the clinical data of 77 hospitalized patients with COVID-19 in YouAn Hospital(Beijing,China)with the aim of providing information on the clinical characteristics and different durations of COVID-19:incubation period,illness onset to first hospital admission,illness onset to discharge,exposure to discharge,and hospitalization duration.Additionally,we aim to identify the potential risk factors for longer hospitalization of patients with COVID-19.
Methods
Data Sources and Collection
We collected and retrospectively reviewed the medical records of compiled data on all 77 hospitalized patients with laboratory-confirmed COVID-19 in Beijing YouAn Hospital,Beijing,China,between January 21 and February 8,2020.COVID-19 was diagnosed in accordance with the interim guidance from the World Health Organization[10].A confirmed case of COVID-19 was defined as a positive result on real-time reverse transcriptase polymerase chain reaction assay of nasopharyngeal swab samples.The local ethics review board of the hospital approved this study and waived the requirement ofinformed consent from each patient,considering the retrospective nature of this study.
Epidemiological,clinical,laboratory,and radiographic data and outcome data were extracted from electronic medical records.In detail,the following information was collected:demographics,exposure and medical history,coexisting diseases,symptoms and signs,laboratory and CT scan findings on admission,complications,and outcome data during follow-up.Complications and clinical outcome were followed up until February 26,2020.Each case was categorized as nonsevere(mild and common types)or severe(severe and critical types)at the time of admission according to the National Health Commission of China guideline[11],which categorizes patients according to four types of severity(mild,common,severe,and critical).Acute respiratory distress syndrome was defined according to the guidance from the World Health Organization for COVID-19[10],and acute kidney injury was defined according to the Kidney Disease:Improving Global Outcomes definition[12].The durations from illness onset to first hospital admission and from illness onset to discharge were calculated,as was the hospitalization duration(hospital length of stay).The durations from exposure to illness onset and from exposure to discharge were calculated in those who had a single point of exposure history and could provide a specific date.
Study Outcomes
The normal length of hospital stay for patients with COVID-19 discharged home alive is currently unclear.Retrospectively,the median hospital length of stay of the 64 discharged patients in our study was 13 days.Thus,we set discharge within 2 weeks(14 days)as the end point of our study and accordingly divided the study patients into two groups:with end point(shorter hospitalization)and without end point(longer hospitalization).Fitness for discharge was based on abatement of fever for at least 3 days,with improved evidence on chest radiography and at least two consecutive negative polymerase chain reaction assay results more than 24 hours apart[11].
Statistical Analysis
Continuous variables were expressed as the mean± standard deviation for normally distributed data or the median with the interquartile range(IQR)for skewed data.Correspondingly,the two-samplettest and the Mann-WhitneyUtest were used to detect differences between groups.Categorical variables were described as the number and percentage and compared by theχ2test or Fisher’s exact test as appropriate.The Kaplan-Meier method was used to estimate the cumulative probability of the end point.A Cox proportional-hazards regression model was conducted to determine the potential risk factors associated with the end point.Statistical significance was defined as P <0.05.All analyses were done with SAS software,version 9.4.
Results
Epidemiological and Clinical Characteristics
The epidemiological and clinical characteristics of the study patients are shown in Table 1.The patients in this study had a very wide age span(1–94 years),with a mean age of 52 years,and there were 34 males(44.2%).A history of exposure to Wuhan was found in most patients(70.1%),especially in the initial stage of COVID-19 spreading in Beijing,as shown in Figure 1.No patients had a history of exposure to the Huanan Seafood Wholesale Market and/or wild animals.There were 33 patients with family clusters ofinfections(42.9%)and two patients who were health care workers(2.6%).Fever was the most common symptom at the onset ofillness,followed by cough and fatigue;digestive symptoms such as diarrhea were rare.Two patients were asymptomatic on admission.Twenty-four patients(31.2%)presented with coexisting disorders,including hypertension(20.8%),cardiovascular disease(11.7%),and diabetes(7.8%).
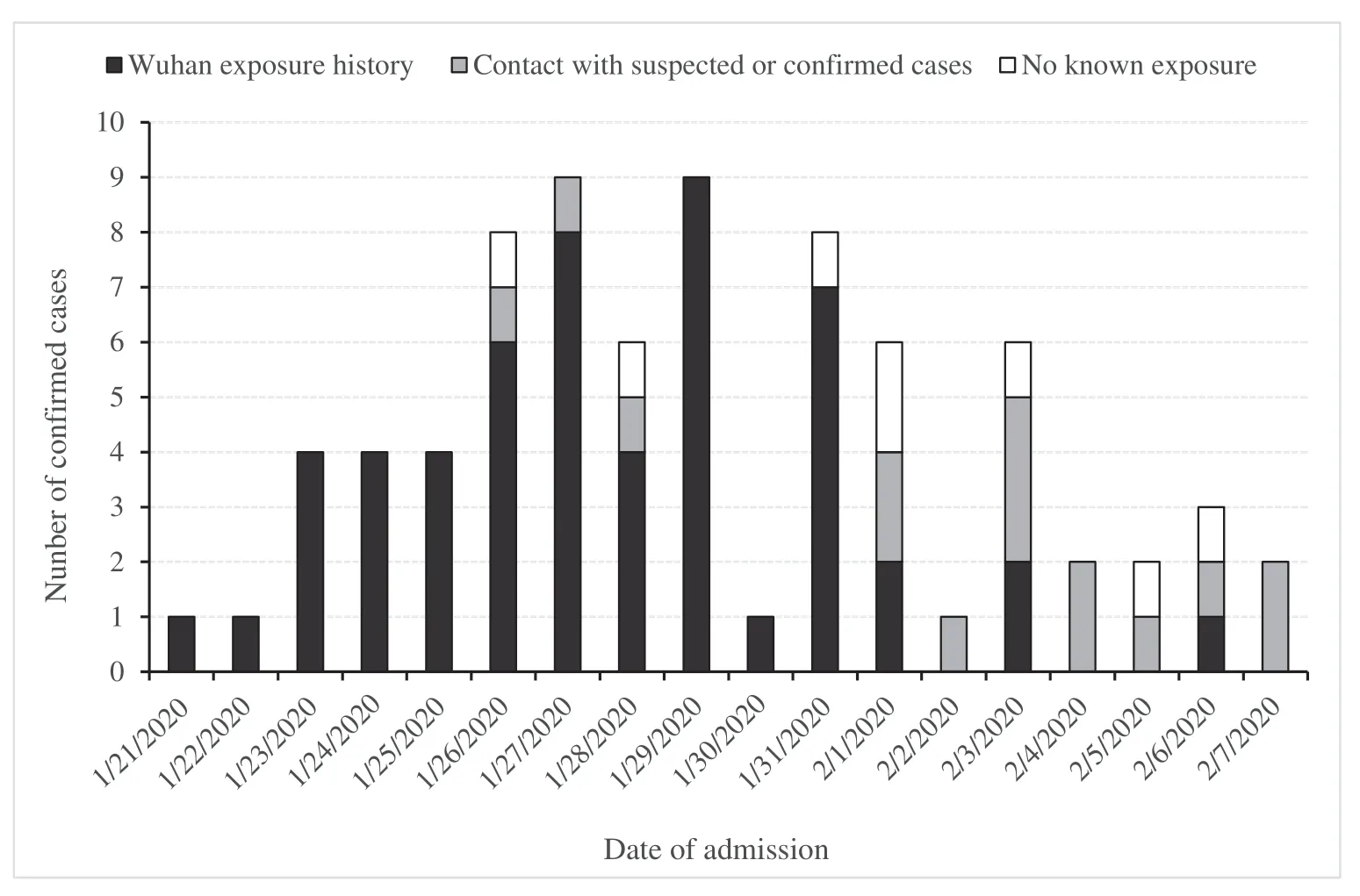
Figure 1 Date of Admission and Exposure Histories of the 77 Study Patients with COVID-19.
Fifty-seven patients(74.0%)were categorized as having nonsevere COVID-19 and 20 patients(26.0%)were categorized as having severe COVID-19.Twenty-eight patients(36.4)developed at least one complication,with liver dysfunction(32.5%)being the most common one,and other complications were rare.Compared with patients with nonsevere COVID-19,patients with severe COVID-19 were older,more likely to present with shortness of breath,and have greater occurrence of hypertension and cardiovascular disease in terms of coexisting diseases.
Laboratory and Radiographic Findings
The laboratory and radiographic findings on admission are presented in Table 2.White blood cell count and neutrophil and lymphocyte proportions were decreased in 35 patients(45.5%),18 patients(23.4%),and 22 patients(28.6%),respectively.Elevations of the count/proportion of these blood cells were also observed in some patients.A significant increase of C-reactive protein level was observed in most patients(64.9%).Of the 73 patients with chest CT scans at the time of admission,71(97.3%)had abnormal results,including three(4.1%)with unilateral pneumonia and 68(93.2%)with bilateral pneumonia.In contrast to patients with nonsevere COVID-19,patients with severe COVID-19 showed significantly higher levels of white blood cells and neutrophils,but lower levels oflymphocytes,monocytes,C-reactive protein,lactate,procalcitonin,creatine kinase MB,myoglobin,and high-sensitivity troponin I.
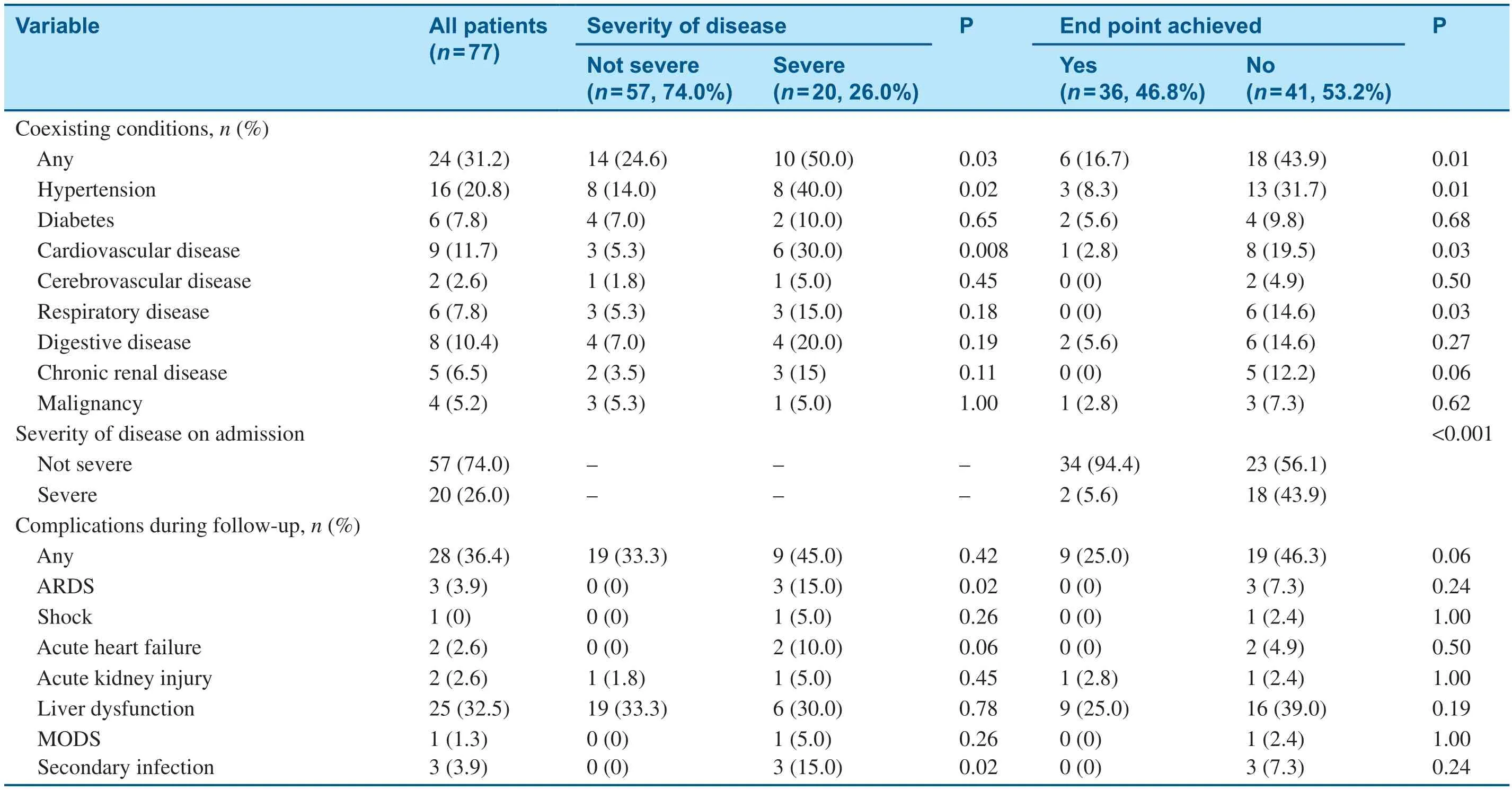
Table 1 (continued)

Table 1 Characteristics of 77 Patients with COVID-19 in Beijing,China.
Durations of Hospitalized Patients with COVID-19
Of the 77 patients,23(29.9%)had a single episode of exposure and could provide the specific date.As shown in Table 3,the median incubation period and the IQR for those patients were 4 days and 3–7 days,respectively.For all patients,the times from illness onset to admission and the hospitalization duration were 5(3–6)days and 13(10–18)days,respectively.For discharged patients,the times from illness onset to discharge and from exposure to discharge(available in 21 patients)were 18.5(15–22)days and 23(17–25)days,respectively.In contrast to patients with severe COVID-19,patients with nonsevere COVID-19 had shorter hospitalization(12[10–16]days vs.18.5[15–21]days)and shorter times from illness onset to discharge(18[15–21]days vs.24.5[22–27]days)and from exposure to discharge(19[16.5–22]days vs.24[24.5–28]days).
Outcomes and Risk Factors for Longer Hospitalization of Patients with COVID-19
All 77 patients were followed up.By the end of followup,64 patients had been discharged,eight remained in hospital,and five had died.Of the five deaths,three were caused directly by COVID-19.Thirtysix patients(46.8%)were discharged within 14 days and thus reached the study end point,including 34 of the patients with nonsevere COVID-19(59.6%)and two of the 20 patients with severe COVID-19(10%).Overall,the cumulative probability of the end point was 48.3%.For patients with nonsevere COVID-19 and patients with severe COVID-19,the cumulative probabilities were 59.7% and 11.8%,respectively(Figure 2).Several variables with a significant difference between patients with and without the end point were selected for the univariable Cox proportional-hazards regression model,as shown in Figure 3.Then all statistically significant risk factors were further included in the multivariable stepwise Cox regression model,and only bilateral pneumonia on CT scan,time from illness onset to admission,severity of disease,and lymphopenia finally remained(Table 4).

Table 4 Risk Factors Independently Associated with the Study End Point by Multivariable Stepwise Cox Proportional-Hazards Regression.
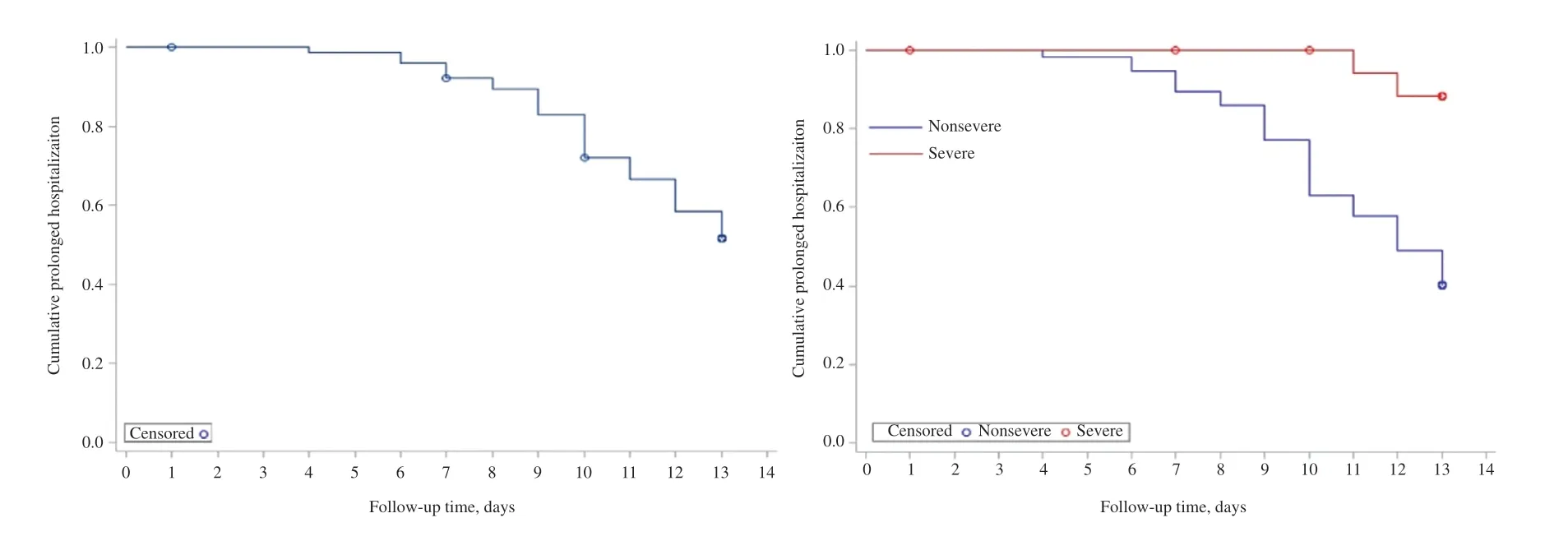
Figure 2 Kaplan-Meier Curves of Cumulative Prolonged Hospitalization for the Overall Population(Left Panel)and Subgroups by Severity of COVID-19(Right Panel).
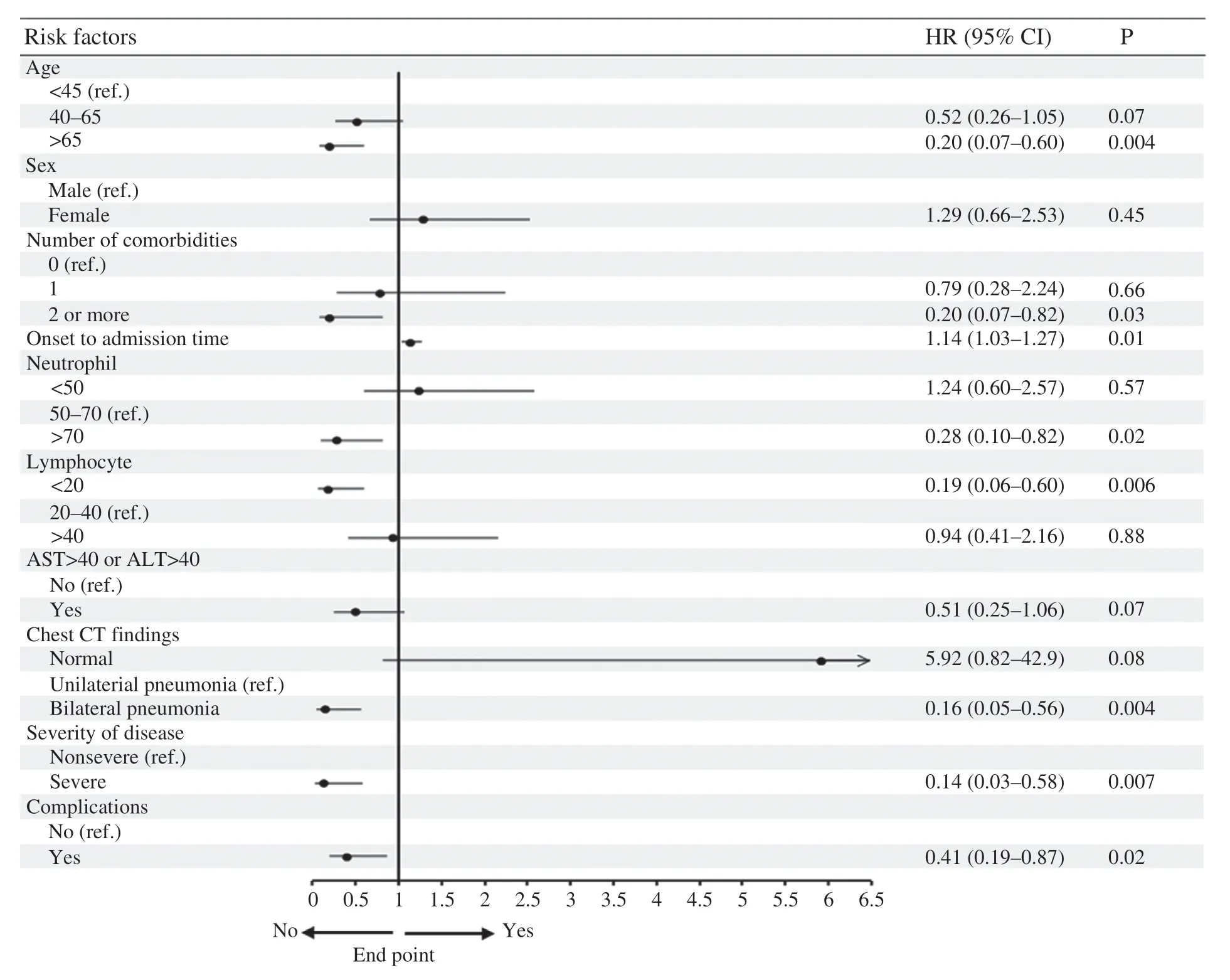
Figure 3 Risk Factors for the Study End Point by Univariable Cox Proportional-Hazards Regression.
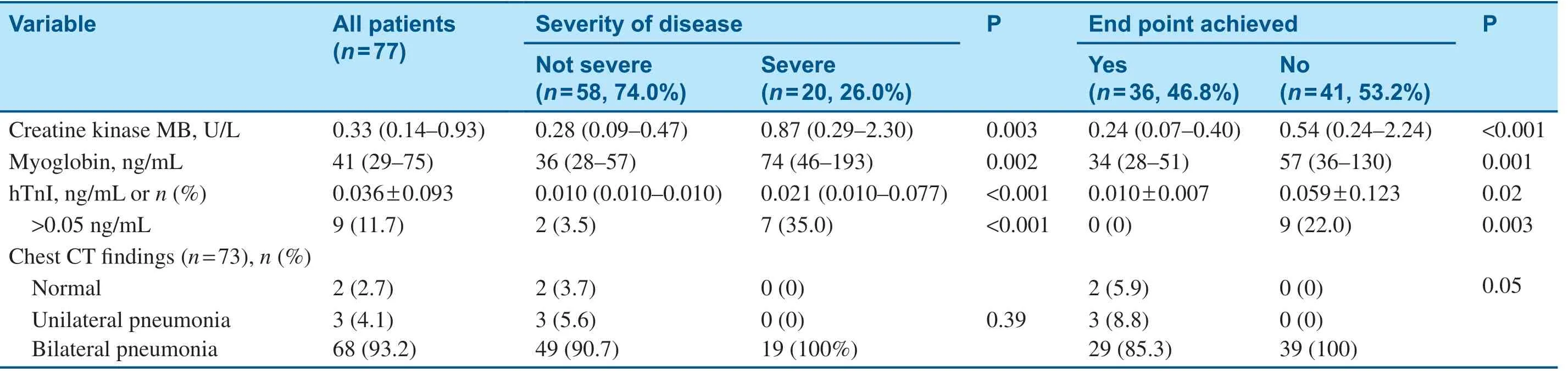
Table 2 (continued)
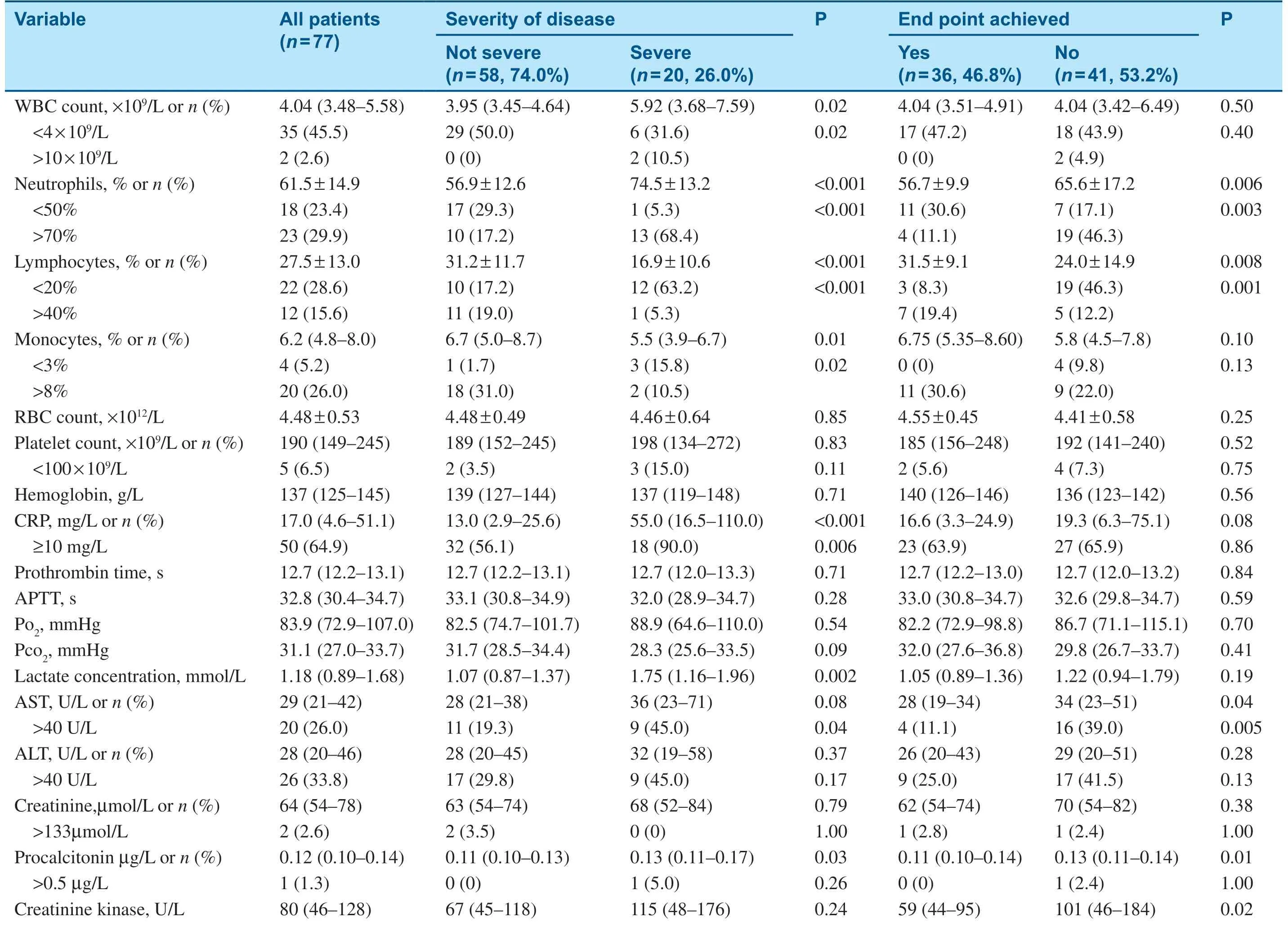
Table 2 Laboratory and Radiographic Findings.

Table 3 Time Courses of Study Patients Grouped by Clinical Outcomes.
Discussion
In the present study,we report retrospective data for 77 hospitalized patients with COVID-19 in Beijing,China,with 64(83.1%)discharged home alive by the end of follow-up.Among the small number of patients,there was a wide age span from 1 to 94 years,suggesting that individuals of all ages are susceptible to SARS-CoV-2 infection.Intriguingly,more females(55.8%)were identifiedin our study,in contrast to previous studies,where males were reported to constitute a higher proportion of patients[1–3,5],revealing that males had a higher expression level of the ACE2 receptor and thus were more susceptible to SARS-CoV-2 infection[13].The data from the Chinese Center for Disease Control and Prevention with a total of 44,672 COVID-19 patients indicated a relativelyeven sex distribution(51.4% males vs.48.6%females)[14].These findings suggest that the sex differences found in the early stage of the outbreak might be a coincidence,such as the exposure difference between sexes.In our study,most of the patients had a history of exposure to Wuhan,especially in the initial stage of the spreading in Beijing,and the number of those patients reduced over time along with the number of all patients.This suggests the effectiveness of quarantine of Wuhan for the control and containment of COVID-19 in Beijing and other cities and countries as demonstrated by a more recent study[15].Many patients(42.9%)were infected by family clustering,which emphasizes the importance of self-isolation ofindividuals with confirmed or suspected cases,as well as the importance of public awareness campaigns and education.
The effect SARS-CoV-2 infection on the cardiovascular system is of great interest for clinicians and researchers.In our study,we found that hypertension and cardiovascular disease were significantly associated with the severity of COVID-19 and prolonged hospitalization of patients with COVID-19.We also observed a higher level of high-sensitivity troponin I in patients with severe COVID-19,as well as in patients with COVID-19 with prolonged hospitalization.These findings suggest an interaction between SARS-CoV-2 infection and the cardiovascular system,but further investigations are warranted to explore the underlying mechanisms.
The incubation time of SARS-CoV-2 infection has been reported by many previous studies.Li et al.[2]studied the first 425 patients in Wuhan,China,and reported that the incubation period was 5.2 days,with a 95% conf idence interval of 4.1–7 days.Based on a national dataset of 1099 patients,Guan et al.[5]reported a similar period,4 days,with an IQR of 2–7 days.We obtained consistent results,a median duration of 4 days with an IQR of 3–7 days.The longest incubation period in our study was 14 days,which further supports the 14-day isolation for suspected cases.
The duration from illness onset to hospital admission is an important factor in the spreading of viral infection.The sooner patients are hospitalized and treated,the less spreading there will be.Previous studies reported that the duration from illness onset to hospital admission in the early stage of this outbreak was 7–12.5 days[1,2,4].In the present study,the time from symptom onset to hospital admission was significantly shorter(5 days,IQR 3–6 days),which is attributed to increased awareness of the public regarding the epidemic and the daily public educational campaigns on precautionary measures against exposure to SARS-CoV-2.It is equivocal whether a longer duration between symptom onset and hospital admission is associated with the clinical outcome of patients.Huang et al.[1]did not find a difference in this duration between ICU and non-ICU patients;however,Wang et al.[4]investigated more patients and found that patients admitted to the ICU had a longer duration(8 days vs.6 days,P=0.009).In the present study,we also observed a longer duration in patients with severe COVID-19 versus patients with nonsevere COVID-19.This may be because a longer prehospital duration may delay treatment and thus lead to unfavorable outcomes.
Currently,few studies have reported the average hospital length of stay of discharged patients with COVID-19.In the present study,we report the median hospital length of stay was 13 days(IQR 10–16.5 days)for patients with COVID-19,which is 3 days longer than reported by Wang et al.[4]on the basis of 38 discharged patients from Wuhan.However,in their study,the patients’incubation period was 2 days longer than in our study.Nevertheless,the length of hospital stay of patients with COVID-19 is significantly shorter(almost 1 month)than that of patients with severe acute respiratory syndrome(SARS)in 2003[16].Because of the small sample size of our study,we were not able to estimate the mortality rate associated with COVID-19,but previous studies reported a lower mortality rate for COVID-19 than for SARS[5,14].Taken together,these data indicated milder severity of COVID-19 than SARS in 2003.
We also found that the cumulative probability of patients with COVID-19 being discharged within 2 weeks was 59.7% for patients with nonsevere COVID-19 and 11.8% for patients with severe COVID-19,which means that nearly 60%of patients with nonsevere COVID-19 will be discharged within 2 weeks.Since the length of hospital stay is related to the duration from illness onset to hospital admission,the duration from illness onset to discharge may better represent the clinical course of COVID-19.If the incubation time is taken into consideration,the whole duration of COVID-19,from exposure to recovery,is 23 days.To the best of our knowledge,this might be the first description of the whole duration of COVID-19.However,only a small number of patients from a single center were included(n=20),and further studies with a large sample size from multiple centers are warranted to confirm this finding.
Longer duration of disease/hospitalization means greater medical burden,especially when facing an exponentially increasing need within a short period produced by transmissible diseases such as COVID-19.One of the most challenging situations during the outbreak of a transmissible disease might be the rapidly increasing number of patients that excessively exceeds health care capacities.Although the outbreak of COVID-19 has been well controlled in China,many other countries are still facing a serious outbreak.The information reported in the present study,especially the duration of COVID-19 and the corresponding risk factors for longer hospitalization,could help those countries to prepare well and redistribute their medical resources so as to f latten the curve and thus delay the epidemic peak.
This study has several limitations.First,a relatively small number of patients from a single center in Beijing were included.Obviously,the length of hospital stay differs across hospitals,cities,and countries.It would be more valuable to determine the corresponding durations and to identify the risk factors on the basis of a dataset at city or national scale.Second,we could not provide useful information on the average duration from illness onset to death because of limited data in our study.Third,treatment is a pivotal determinant of the duration of disease,however,we currently have no detailed data on treatment of patients with COVID-19 and cannot determine the influence of treatment on the durations of COVID-19.However,we will continue this work in the future.Fourth,because of the nature of the outbreak of this disease and the retrospective nature of this study,we were not able to calculate the power of this study,which should be noted when one is interpreting the results of this study.
In conclusion,the median hospital length of stay was 13 days for discharged patients with COVID-19,and the median time of the clinical course was 23 days.Both are significantly shorter than for SARS.Bilateral pneumonia on CT scan,shorter period from illness onset to admission,lymphopenia,and severity of disease are the risk factors for longer hospitalization of patients with COVID-19.There findings might be useful for countries or territories facing the threat of COVID-19 to prepare well and rebalance their medical resources.
Acknowledgments
We thank all patients,researchers,physicians,and nurses involved in this study.
Conf licts ofinterest
We declare no competing interests.
 Cardiovascular Innovations and Applications2021年3期
Cardiovascular Innovations and Applications2021年3期
- Cardiovascular Innovations and Applications的其它文章
- Running with Face Masks or Respirators Can Be Detrimental to the Respiratory and Cardiovascular Systems
- CTO(Chronic Total Occlusion)
- In-Hospital Cardiac Arrest after Emotional Stress in a Patient Hospitalized with Gastrointestinal Symptoms and Chronic Anxiety Disorder
- Junctional Pacemaker May Replace the Sinoatrial Node
- A Patient with Atezolizumab-Induced Autoimmune Diabetes Mellitus Presenting with Diabetic Ketoacidosis
- Similarities and Differences of CT Features between COVID-19 Pneumonia and Heart Failure