
Junctional Pacemaker May Replace the Sinoatrial Node
2021-10-22 08:05:00MinLinMDYuqinXiongMDYipinLinMDYuhuaLiMDandLijuanZhangMD
Min Lin,MD,Yuqin Xiong,MD,Yipin Lin,MD,Yuhua Li,MD and Lijuan Zhang,MD
1 Department of Electro-Cardiographic Information,First Affiliated Hospital of Xiamen University,School of Medicine,Xiamen University,and Xiamen Key Laboratory of Cardiac Electrophysiology,Xiamen,361003,China
Abstract Junctional rhythm is usually seen in the clinic with different causes.We report a case of bicuspid aortic valve accompanied by sinoatrial node dysfunction.The junctional escape beat could accelerate with physiological needs and provided for the normal needs of daily life when dysfunction of the sinoatrial node occurred,which provides a new way for the treatment of sinoatrial node dysfunction.Our findings could be potentially significant for identifying causes and choosing appropriate treatment strategies by using ECG monitoring in the clinic in the future.
Keywords:Junctional rhythm;bicuspid aortic valve;electrocardiogram;sinoatrial node dysfunction
Case Presentation
The patient is a 23-year-old woman with a history of congenital bicuspid aortic valve and congenital vaginal atresia.Arrhythmia was observed without any symptoms during an orientation health check.A dynamic ECG was performed in our hospital for further treatment(Figure 1).
The ECG at night(Figure 1A)showed slow sinus beats(arrows)of about 21 per minute during the whole day and junctional escape beats(stars)at a slightly faster frequency of about 29–33 per minute.Also tens of thousands of premature atrial conductions and escape beats were observed in the dynamic ECG.As the daily activity changed,the heart rates were dynamically observed to become faster(51 bpm;Figure 1B)and stable(Figure 1C)in some periods of the whole day.The fastest heart rate during the whole day was 63 bpm(Figure 1D),and all the beats were accelerated junctional rhythm.The disappearance of the sinus P wave might be caused by sinus arrest or sinus bradycardia.Echocardiography confirmed the presence of bicuspid aortic valve malformation and that the valve activity was good(Figure 2).
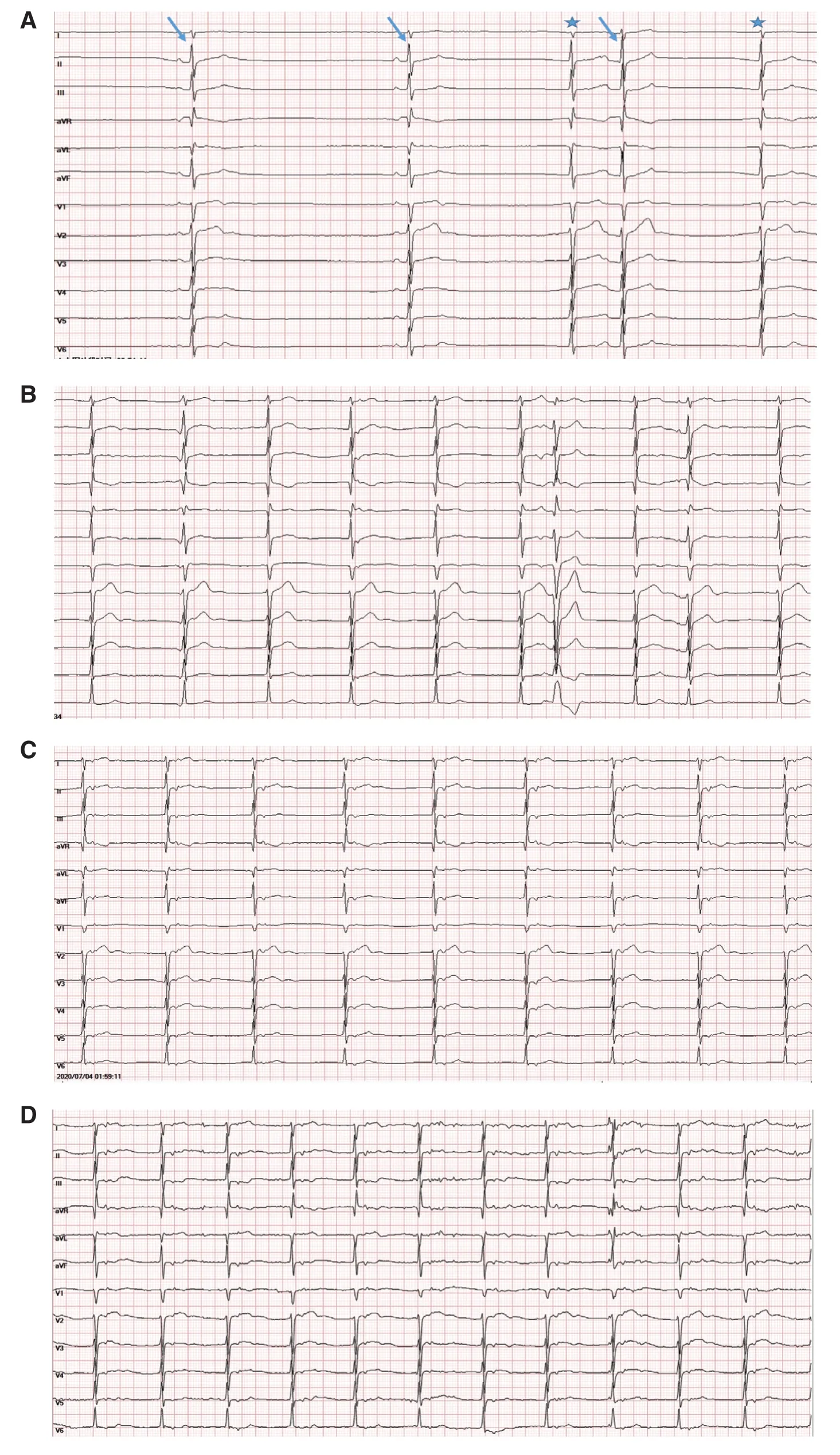
Figure 1 (A)The Lowest Heart Rate with Junctional Escape Beats(29–33 bpm)in the Dynamic ECG.(B)The Junctional Escape Beats Became Faster(51 bpm)Combined wth Atrial or Sinus Seizures in the Dynamic ECG.(C)The Junctional Rhythm Became Stable(45 bpm)in Some Periods of the Dynamic ECG.(D)The Fastest Heart Rate as Junctional Rhythm(63 bpm)in the Dynamic ECG.
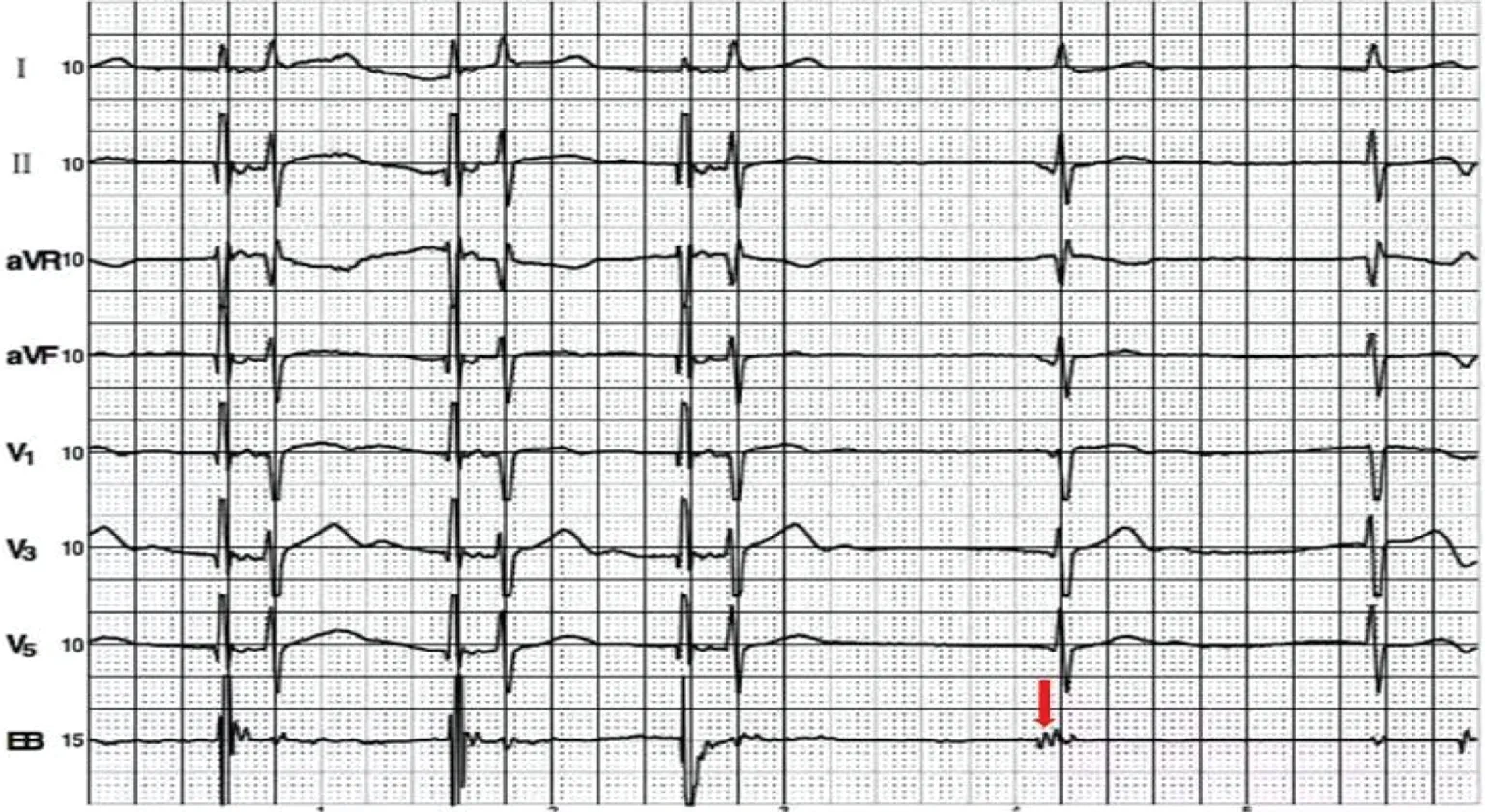
Figure 3 A Faster Artificial Atrial Stimulation at 60 bpm Captured the Heart and Restrained the Junctional Pacemaker on Esophageal Electrophysiologic Examination.An atrial potential was obvious in the esophageal ECG(arrow).
Then esophageal electrophysiologic examination was performed for further diagnosis(Figure 3).A faster artificial atrial stimulation at 60 bpm was applied to capture the heart and to restrain the junctional pacemaker.We observed the appearance of atrial potential on the EB lead.It might be a sinus P wave,but it was still too slow to conduct to the ventricle compared with the junctional escape beat.The results indicated that the autonomy of the junctional pacemaker is significantly higher than that of the sinoatrial node.Then we monitored her ECG during exercise(Figure 4).Before exercise,the ECG showed escape beats and atrial capture beats(Figure 4A).Then the heart rate of junctional rhythm accelerated to 103 bpm to accommodate the body’s needs during exercise,paralleled with premature atrial contractions.Her increased heart rate came from the junctional area during physical activity,which showed that the autonomic heart rate of the junctional area had sufficient emergency capacity.
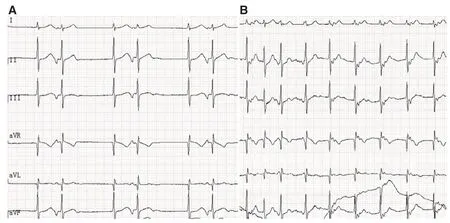
Figure 4 (A)The ECG Before Exercise.(B)The Heart Rate Accelerated to 103 bpm During Exercise.
Discussion
Congenital bicuspid aortic valve,one of the most common congenital cardiac malformations,is associated with valvular abnormalities and aortopathies.It increases the risk of thoracic aortic aneurysm and dissection,infective endocarditis,and sudden cardiac death[1].However,sinoatrial node dysfunction was not previously seen in patients with congenital bicuspid aortic valve.To the best of our knowledge,herein we have for the first time reported a case of congenital bicuspid aortic valve accompanied by sinoatrial node dysfunction;however,there is no direct or definite relationship between them.Furthermore,this patient also has a congenital absence of the vagina and a reverse position of the upper abdominal viscera according to computerized tomography.So both sinoatrial node dysfunction and cardiac malformations caused by congenital dysplasia should be considered.Congenital sick sinus syndrome without an apparent cause may be related to genetic mutations[2].
Intriguingly,in this case,the autonomous junctional rhythm could increase with physiological needs,and seemed to replace the sinoatrial node to meet the needs of daily life.Junctional escape rhythm is often caused by increased vagal tone,slowing of the sinoatrial node,atrioventricular(AV)or sinoatrial node block,or acceleration of a subsidiary pacemaker[3].Kishimoto et al.[3]reported a 19-year-old woman who had a junctional rhythm with a slow heart rate caused by slowing of the primary pacemaker.The AV node pacemaker cells accelerated after local anesthesia because of the increased sympathetic activity due to adrenaline.In our case,the slow junctional rhythm at rest was caused by the slowing of the sinoatrial node and the accelerated AV node junctional pacemaker.The accelerated junctional rhythm during exercise or daily activity was caused by increased automaticity of AV junctional cells that is mediated by sympathetic excitation.
Significant sinus bradycardia and prolonged sinus arrest are clear indications for the installation of a permanent cardiac pacemaker.The present case provided new insights for indications for pacemaker installation.From her dynamic and exercise ECG,we thought her own ectopic pacemaker might replace the sinus node to meet the needs of daily life.Especially for young people and those whose sinus bradycardia stem from congenital dysplasia,the junctional pacemaker had been sufficiently“ exercised” to maintain this state relatively steadily over time.Also it might have no need to intervene the junctional rhythm with bradycardia during the night as the patient was asymptomatic.Further follow-up is needed for long-term prognosis.For other sinus bradycardia caused by acute injuries or degenerative changes in old age,pacemaker therapy is still necessary.
In conclusion,we described a case of sinoatrial node dysfunction with congenital bicuspid aortic valve where the AV node junctional pacemaker could accelerate in sympathetic activity as the sinoatrial node.Our findings could be potentially significant for identifying causes and choosing appropriate treatment strategies by using ECG monitoring in the clinic in the future.
Funding
This study was supported by a grant from the Guidance Project of the Xiamen Medical and Health Program(3502Z20199007).
Declaration ofinterest
None.
Ethics
The study was performed in accordance with the Declaration of Helsinki and was approved by the Research Ethics Commission of Xiamen Medical University.Given the retrospective review of this study,informed consent was waived.
Author contributions
Min Lin:Conceptualization,funding acquisition,formal analysis,writing original draft,and project administration.
Yuqin Xiong and Yipin Lin:Investigation,formal analysis,and review and editing.
Yuhua Li:Supervision,investigation,and data curation.
Lijuan Zhang:Conceptualization,resources,and review and editing.
 Cardiovascular Innovations and Applications2021年3期
Cardiovascular Innovations and Applications2021年3期
- Cardiovascular Innovations and Applications的其它文章
- Running with Face Masks or Respirators Can Be Detrimental to the Respiratory and Cardiovascular Systems
- CTO(Chronic Total Occlusion)
- In-Hospital Cardiac Arrest after Emotional Stress in a Patient Hospitalized with Gastrointestinal Symptoms and Chronic Anxiety Disorder
- A Patient with Atezolizumab-Induced Autoimmune Diabetes Mellitus Presenting with Diabetic Ketoacidosis
- Clinical Characteristics and Durations of Hospitalized Patients with COVID-19 in Beijing:A Retrospective Cohort Study
- Similarities and Differences of CT Features between COVID-19 Pneumonia and Heart Failure