
Association of marital status with takotsubo syndrome (broken heart syndrome) among adults in the United States
2021-09-06 05:19DukeAppiahRachelFariasDenaHeloLindaAppiahOlugbengaOlokedeChikeNwabuoNandiniNair
World Journal of Cardiology 2021年8期
Duke Appiah,Rachel Farias,Dena Helo,Linda Appiah,Olugbenga A Olokede,Chike C Nwabuo,Nandini Nair
Duke Appiah,Rachel Farias,Dena Helo,Olugbenga A Olokede,Department of Public Health,Texas Tech University Health Sciences Center,Lubbock,TX 79430,United States
Linda Appiah,College of Education,Texas Tech University,Lubbock,TX 79409,United States
Chike C Nwabuo,Division of Cardiology,Johns Hopkins University,Baltimore,MD 21218,United States
Nandini Nair,School of Medicine,Texas Tech University Health Sciences Center,Lubbock,TX 79430,United States
Abstract BACKGROUND The pathophysiology of takotsubo syndrome (TTS) is not well understood,however,it is often precipitated by psychological or physical stress.Marital status is related to emotional stress,but its associations with TTS are limited.AIM To explored the potential association between marital status and TTS.METHODS We conducted a case-control study using data on patients aged ≥ 40 years with marital status data in the National Hospital Discharge Survey (2006-2010).The International Classification of Diseases Ninth Revision codes were used to identify cases with TTS and other comorbid conditions.Each case was matched to 5 controls by age,sex,year of TTS diagnosis and bed size of hospital.Two sets of controls were selected:Acute myocardial infarction (AMI) controls and noncardiovascular disease (CVD) controls.Conditional logistic regression was used to estimate odds ratios (OR) and 95% confidence intervals (CI) for the association of marital status with TTS.RESULTS The 59 patients with TTS who had information on marital status were matched to 295 controls with AMI and 295 non-CVD controls,resulting in a sample of 649 patients.The average age of cases was 69.7±11 years with 90% being women and 88% reporting White race.In multivariable-adjusted models,compared to singles,patients who were married had lower odds of TTS (OR=0.86,95%CI:0.79-0.93)while those who were widowed (OR=1.14,95%CI:1.05-1.23) or divorced/separated (OR=1.32,95%CI:1.21-1.45) had elevated odds for TTS when compared to non-CVD controls.Similar results were observed when cases were compared to controls with AMI.CONCLUSION In this study,being married was associated with lower odds for TTS while being divorced/separated or widowed was related to elevated odds for TTS.These novel findings that underscore the potential importance of social factors like marital status in the development of TTS need confirmation in larger studies.
Key Words:Stress-induced cardiomyopathy;Takotsubo syndrome;Marital status;Epidemiology;Case-control;Marriage
INTRODUCTION
Takotsubo syndrome (TTS),also known as “broken heart syndrome” is a transient dysfunction of the left ventricle (LV)[1].Its initial presentations are similar to acute coronary syndrome,and it is characterized by varying combinations of chest pain,ischemic electrocardiographic changes pertaining to ST-segment elevation and/or Twave inversion,and moderate elevations in cardiac biomarkers such as troponin[2].Almost 80% of all cases occur in older women[1,3].In the United States,the incidence of TTS has been increasing over the years.During the period of 2007 to 2012,the incidence of TTS increased by more than 300% from 52 per 1000000 discharges to 178 per 1000000 discharges[4].Although the pathophysiology is not well understood,it is often precipitated by psychological or physical stress[5],as well as acute neurologic and psychiatric diseases[6].
While the prognosis is favorable with recovery of LV function in some patients,growing evidence suggests that TTS is associated with severe morbidity and mortality[7].Patients with TTS are at high risk for recurrence after the first events[6].Emerging evidence suggest that more than half of patients with TTS develop severe complications,and that TTS-related mortality is comparable to those amongst patients with myocardial infarction or acute coronary syndrome[8,9].
Due to the observed stress triggers,it has been suggested that TTS may be related to some social and emotional factors that influence psychological wellbeing.Marital status is related to emotional stress[10].However,investigations into the relation of marital status with TTS are limited,with most of these being case reports[11,12].
We aimed to explore the association of marital status with TTS in a national sample of hospitalized adults from the United States.
MATERIALS AND METHODS
The National Hospital Discharge Survey (NHDS) which is administered by the National Center for Health Statistics is a continuous survey of inpatient utilization of short-stay (<30 d) hospitals in the United States.The NHDS which was conducted from 1965-2010 used a multistage cluster sampling technique to provide nationally representative data.All procedures were approved by the institutional review board of the National Center for Health Statistics with all patients providing written informed consent for their information to be included in this database.All data from the NHDS are publicly available through the Centers for Disease Control and Prevention:https://www.cdc.gov/nchs/nhds/index.htm.Because the NHDS data is deidentified and publicly available,the Texas Tech University Health Sciences Center Institutional Review Board determined that this current study did not require a review
We conducted a case-control study using discharge records from 2006 to 2010.Patients who were aged ≥ 40 years with no missing data on marital status and did not have a diagnosis of myocarditis or pheochromocytoma were eligible for this study.Marital status information which was obtained from the National Center for Health Statistics was classified as single,married,divorced,separated or widowed.Similar to other reports from national samples[2,4,13],the International Classification of Diseases Ninth Revision codes were used to identify cases with TTS (ICD-9-CM:429.83) and other comorbid conditions.Acute myocardial infarction (AMI) was identified using ICD-9 codes:410 while stroke was defined with ICD-9 codes 430 to 438.
Cases were defined as patients with TTS who underwent diagnostic coronary angiography and did not receive any percutaneous coronary interventions or revascularizations.A control was defined as any patient without TTS diagnosis during hospitalization.Each case was matched to 5 controls by age,sex,year of TTS diagnosis and bed size of hospital.Hospital bed size,defined as the number of beds per hospital,was used as a measure of hospital volume.The greedy matching strategy with a fixed number of controls per case was used[14].Matched controls were selected from among all patients’ who met the eligibility criteria listed above.Two sets of controls were selected for each case.Thus,for each case,5 controls with AMI were selected (considered as AMI controls) and also 5 non-cardiovascular disease (CVD) controls were selected (considered as non-CVD controls).Patients with AMI or stroke were considered eligible for CVD controls.
Means and percentages were used to describe the characteristics of patients.Conditional logistic regression incorporating sampling weights was used to estimate odds ratios (OR) and 95% confidence intervals (CI) for the association of marital status with TTS.Besides the matching variables of age,sex,year of TTS diagnosis and bed size of hospital,adjustments were made for race,type of health insurance,smoking status,obesity,hypertension,dyslipidemia,diabetes and chronic obstructive pulmonary disease.Additional analyses were performed with further adjustment for neurological and psychiatric disorders.A 2-tailed p value less than 0.05 was used to determine statistical significance,and all analyses were performed with SAS version 9.4 (SAS Institute Inc).
RESULTS
The 59 patients with TTS who had information on marital status were matched to 295 controls with AMI and 295 non-CVD controls,resulting in a sample of 649 patients.Characteristics of the 649 participants included in the study are presented in Table 1.The average age of cases was 69.7±11 years with 90% being women and 88%reporting White race.Overall,a greater proportion of participants were from the southern region of the United States with about two-thirds of participants having Medicare as their principal expected source of payment.Approximately 39% of cases were married,17% were single,and 27% were widowed.There were significant differences in race/ethnicity between cases and AMI controls or non-CVD controls.Although AMI controls and non-CVD controls had higher prevalence of neurologic and psychiatric disorders than patients with TTS,these differences did not meet statistical significance (P>0.05).
A significant association was observed between marital status and TTS (Table 2) in multivariable models.Compared with singles,patients who were married had lower odds for TTS (OR=0.86,95%CI:0.79-0.93) while those who were widowed or divorced/separated had 14% (OR=1.14,95%CI:1.05-1.23) and 32% (OR=1.32,95%CI:1.21-1.45) elevated odds for TTS,respectively,when compared to non-CVD controls.Similar results were observed when cases were compared with controls with AMI.Compared to patients who were currently married,non-married patients (single,widowed or divorced/separated) were at elevated risk for TTS,whether compared to AMI controls (OR=1.66,95%CI:1.58-1.75) or non-CVD controls (OR=1.40;95%CI:1.34-1.46).These associations remained largely the same when additional adjustments were made for neurological and psychiatric disorders (Table 3).

Table 1 Characteristics of participants according to case-control status,National Hospital Discharge Survey 2006-2010

Table 2 Adjusted estimates for the association of marital status with takotsubo syndrome by acute myocardial infarction and noncardiovascular disease controls,National Hospital Discharge Survey 2006-20101
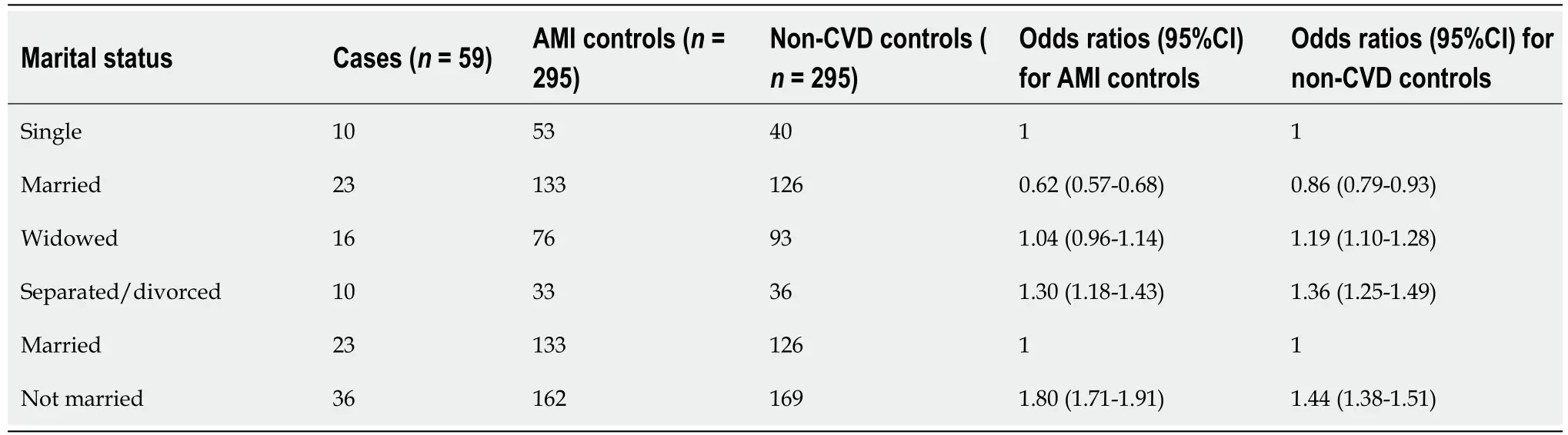
Table 3 Estimates from fully adjusted models for the association of marital status with takotsubo syndrome by acute myocardial infarction and non-cardiovascular disease controls,National Hospital Discharge Survey 2006-20101
DISCUSSION
In this case-control study using a nationally representative sample,being married was associated with lower odds for TTS while being divorced/separated or widowed was associated with elevated odds for TTS.These novel findings corroborate previous reports of marriage being related to good cardiovascular health while being single or encountering marital disruptions such as divorce/separation or widowhood is associated with poor overall and cardiovascular health outcomes[10].
To our knowledge,this is the first observational study to evaluate the association of marital status with TTS.Although the relationship of family or social history with TTS have not been extensively investigated,previous case reports and case series have observed TTS among elderly women who were recently widowed[11,12] or had loss of a close family member[15].Emotional stresses such grief,interpersonal conflicts,fear,panic,anxiety and anger have been frequently observed in women with TTS compared to physical stressful event[16].Among the few studies on TTS that obtained marital status information,TTS was more common among patients who were not married compared to those who were currently married[3],results that are similar to findings of the current study.
There are several plausible explanations for these observations.Marriage offers certain behavioral,social and psychological benefits that may help in the prevention of TTS.Many married couples tend to have better CVD risk profiles namely healthier meals,physical activity,adequate sleep and better financial benefits that often lead to less stress than singles,divorced/separated or widowed persons[10,17].Married couples often have larger social networks and support,and are known to report greater happiness and life satisfaction as well as higher compliance with medical screenings and uptake of medications[10].The protective benefits of marriage for TTS and other CVD may also simply reflect the fact that healthy individuals usually select other healthy individuals for marriage[17].
Marital disruptions (i.e.,divorce/separation or widowhood) typically have deleterious effects on health.Acute events like widowhood,especially if unexpected,can lead to sudden heightened psychological stress,depression and loss of some social support[10].Persons in troubled marriages which often end in divorce/separation may also experience these conditions.Some studies have observed high levels of catecholamines especially epinephrine in individuals experiencing marital conflicts[17].Evidence from animal studies and histologic findings suggest that a surge in circulating epinephrine may induce transient LV dysfunction due to their toxicity on myocardial cells resulting from a rise in cyclic AMP-mediated calcium overload of cardiocytes[12,18].This calcium overload of cardiocytes triggers the formation of free oxygen radicals,expression of stress response genes,and also the induction of apoptosis in a subset of myocardial cells[12].However,with the full resumption of LV function weeks after the occurrence of TTS in some patients,it holds to reason that this cascade of molecular activities leading to apoptosis in some cardiomyocytes may not fully explain the role of catecholamines in the development of TTS[12,19].
Other factors such as neurologic and psychiatric disorders at the time of admission have been reported to be significantly associated with in-hospital complications among patients with TTS[6,20].Some studies have reported higher prevalence of neurologic and psychiatric disorders in patients with TTS compared to controls;however,results for the association of these disorders with TTS have been mixed[21].In the current study,there was no significant difference between patients with TTS and AMI controls or non-CVD controls,and additional adjustment for neurologic and psychiatric disorders did not appreciably change the reported estimates between marital status and TTS.The discrepancy in findings between the current study and some prior studies may,in part,be explained by differences in sample size and study designs.Patients with TTS often have recurrent events,with the risk of reoccurrence being higher among patients with pre-admission psychiatric disorders[22].With about 39% of patients with TTS reporting a neurological disease and 50% of patients with TTS reporting at least one mental disorder about 17.5 mo from their index event[23],future studies are warranted to investigate the potential role of therapeutics in preventing the incidence or reoccurrence of TTS in patients with neurologic and psychiatric disorders.
A strength of this study is the usage of a population representative sample that enhance the generalizability of the findings.Limitations of this study include the small sample of TTS cases due to exclusion of patients without data on marital status,and the inability to study the quality of marriage or sex differences on the relation of marital status with TTS.Also,data on the severity of the acute disease between cases and controls were not available.Finally,ICD codes which are susceptible to error during the coding process were used to identify diseases and comorbid conditions.However,the use of ICD codes is the standard procedure for identifying TTS cases in national samples from the United States[2,4,13].For TTS,information for confirming the diagnosis such as cardiac enzymes as well as echocardiographic or electrocardiographic readings were not available.Therefore,patients with conditions like coronary spastic angina could not be excluded.Finally,even though we controlled for several potential confounders,the possibility of residual confounding influencing these results cannot be entirely ruled out.
CONCLUSION
In conclusion,these novel findings show that being married is associated with lower odds for TTS,whereas the occurrence of divorce/separation,or widowhood is associated with higher odds of TTS.These results have substantial clinical and public health importance.Given that growing evidence suggests that TTS is associated with severe morbidity and mortality[7],understanding the specific pathophysiologic pathways that may be involved in the association of social stress factors and TTS holds promise in providing avenues to prevent this disease.Therefore,confirmation of these observed associations from prospective studies are warranted to better understand the relation of marital status with TTS and elucidate specific pathophysiologic pathways that are involved in the association between marital status and TTS.
ARTICLE HIGHLIGHTS
Research background
The incidence of takotsubo syndrome (TTS) is increasing in the United States.However,the pathophysiology of TTS is not well understood,although,it is often precipitated by psychological or physical stress.
Research motivation
Marital status is related to emotional stress.However,not many studies have been conducted to evaluate the association of family relationships or social history with TTS.
Research objectives
The objective of this study was to evaluate the association of marital status namely being single,married,widowed or divorced/separated with TTS in an elderly population.
Research methods
A case-control study was performed using data on 649 patients from the United States National Hospital Discharge Survey.
Research results
Findings from this study showed that being married was associated with lower odds for TTS while being divorced/separated or widowed was associated with elevated odds for TTS.
Research conclusions
With marital status associated with TTS,understanding the underlying mechanisms for this association is of substantial clinical and public health importance.
Research perspectives
Confirmation of these observed associations from prospective studies are warranted to better understand the relation of marital status with TTS.
 World Journal of Cardiology2021年8期
World Journal of Cardiology2021年8期
- World Journal of Cardiology的其它文章
- ISCHEMIA trial:How to apply the results to clinical practice
- Shortened dual antiplatelet therapy in contemporary percutaneous coronary intervention era
- Multimodality imaging in the diagnosis and management of prosthetic valve endocarditis:A contemporary narrative review
- Potential role of an athlete-focused echocardiogram in sports eligibility
- In-depth review of cardiopulmonary support in COVID-19 patients with heart failure
- Surgical strategies for severely atherosclerotic (porcelain) aorta during coronary artery bypass grafting