
Open globe injuries in geriatric population in lran:characteristics and outcomes
2021-08-16 09:55MaryamZamaniSeyedAliTabatabaeiAkbarFotouhiMortezaNaderanMohammadSoleimani
Maryam Zamani, Seyed Ali Tabatabaei, Akbar Fotouhi, Morteza Naderan, Mohammad Soleimani
1Ocular Trauma and Emergency Department, Eye Research Center, Farabi Eye Hospital, Tehran University of Medical Sciences, Tehran 1336616351, Iran
2Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran 1336616351, Iran
Abstract
INTRODUCTION
In the era of preventive medicine, ocular trauma is worth special attention[1]. Globally, eye trauma is the leading cause of monocular blindness[2-3]. The effects of trauma,and especially, open globe injury on the health resources and individual demands should be emphasized[4-5]. This is especially important in elderly people who may need a relatively stable visual function to continue an independent life.
According to United Nations reports, the elderly population(aged 60y or over) has increased from eight percent in 1950 to twelve percent in 2013 and it is estimated that the geriatric population will reach 21 percent in 2050[6]. The inevitable aging process causes numerous limitations in the personal and social life that do not spare visual function. Indeed, elder patients may already have declined vision due to undiagnosed cataract or age-related macular degeneration which predispose them to more trauma even during simple daily activities.Unfortunately, if the trauma endangers visual function, a vicious cycle may occur which leads to greater vulnerability and severe dependence for daily activities.
Despite the importance of the issue (as mentioned above),the majority of studies concerning open globe injury have focused on populations other than the geriatric population[7-13].
Only a few articles specifically reviewed open globe injuries among elderly patients[14-17]. In the current study, we describe the characteristics of open globe injuries in geriatrics and emphasize the prognostic indicators among them.
SUBJECTS AND METHODS
Ethical ApprovalThe present study was conducted under the principles of the Declaration of Helsinki. It was approved by the Ethics Committee of Farabi Eye Hospital. Written informed consents were signed by the patients for publication of any information pertaining to their health data.
We retrospectively reviewed medical records of all patients aged 60y and older who presented to the Emergency Department of Farabi Eye Hospital (Tehran, Iran) with the diagnosis of open globe injury. The study records spanned 10y from 2006 to 2016.
We documented demographic features, type, and mechanism of open globe injury, ocular trauma score (OTS), visual acuity before and after treatment, the zone of injuries, and the associated injuries found at the presentation or thereafter. The OTS predicts the visual outcome in the population with ocular trauma according to the initial visual acuity, type of injury and associated findings. It was calculated based on the data available at the presentation when possible as described by Kuhnet al[18]. Raw OTS would categorize into specific classes:class 1: 0-44 points, class 2: 45-65 points, class 3: 66-80 points, class 4: 81-91, and class 5: 92-100 points. The higher the OTS class, the better the visual acuity. Wound location was defined as zone I if the injury was limited to the cornea and limbus. Zone II injuries is related to the anterior 5 mm of the sclera (not extending into the retina). Zone III injuries indicated full-thickness scleral defects more posterior than 5 mm from the limbus.
Statistical AnalysisData analysis was performed using SPSS version 25. All the percentages were reported without considering the missing data. One-samplet-test, independentsamplest-test and Mann-WhitneyUtest were used to compare means. The relationship between quantitative variables was assessed using bivariate correlation. For evaluating the association between two categorical variables, we used the Chi-square test, the two-tailed Fisher exact test and Fisher-Freeman-Halton test (labeled as Fisher exact test in SPSS with a slight difference in method). Multiple Logistic regression analyses were done to analyze the independent predictors that mostly influence the dependent variable. Αny predictor whose univariate test resulted inP‐value of ≤0.2 was a candidate for the multivariable model; all variables of known clinical importance were also considered. We reported the indicators of final visual acuity with a significantPvalue of less than 0.05.
RESULTS
This study included 248 eyes from 248 patients. The mean age was 69.2±5.8y (range: 60-90y). Men outnumbered women by a factor of 3.06. Twenty-three percent of patients had a history of previous intraocular surgery, frequently including cataract surgery and penetrating keratoplasty. Approximately 13.7 and 25.4 percent of patients had a history of diabetes and hypertension, respectively.
The three most common mechanisms of an open globe injury were falling (25.2%), sharp objects (18.9%), and tree branches(13.9%). Penetrating injury accounted for most of the geriatric ocular trauma (50.4%), followed by globe rupture (40.3%),intraocular foreign body (IOFB; 7.3%), and perforating injury(2.0%). The mean raw OTS was 60.5. The injuries in the zone I were most frequent (48.5%) followed by zone II (30.0%), and zone III (21.5%). Right, and left eyes were involved in 134 and 114 patients respectively. The visual acuity at presentation was 20/200 or less in 215 patients (87.8%) at presentation (mean logMAR was 2.43). The time between the occurrence of the injury and primary repair was within 24h in 116 cases (60.1%).Due to the delay in the presentation or patients’ factors for undergoing operation under general anesthesia, the remaining underwent primary repair later than 24h. The frequency distribution of associated signs is shown in Table 1. The three most frequent associated signs were hyphema (73.0%), uveal tissue prolapse (58.9%), and traumatic cataract (23.8%) in order.

Table 1 Frequency distribution of signs associated with open globe injuries n (%)
Two hundred and forty‐five cases (98.8%) underwent primary repair and 144 patients (58.8% of previously repaired) required secondary operations. Posttraumatic endophthalmitis was found in 8 patients (3.2%). Enucleation was accomplished in 4 cases (1.6%) whose eyes were so disorganized that the globe could not be saved. The final visual acuity results were recorded from the latest medical documents of the patients(mean: 14.8mo, range: 5 to 71mo after final surgery) and were divided into two groups: >20/200 and ≤20/200. The characteristics of open globe injuries in these two groups are shown in Tables 2 and 3. The average logMΑR in ≤20/200 group was significantly worse than the other (2.62vs1.84,P˂0.001). The mean raw OTS was 55.8 in ≤20/200 group and 74.8 in >20/200 group (P<0.001).
There was an association between three variables (the type of open globe injury, initial visual acuity and OTS classes)and final visual acuity (P=0.001, <0.001, and <0.001 in order). We analyzed the effects of age, gender, mechanismof injury, initial visual acuity, injury subtype, the zone of damage, time until repair, and OTS on the final visual acuity.The multivariate Logistic regression model was statistically significant (χ2=54.984,P<0.001). The model explained 29.8%(NagelkerkeR2) of the variance in final visual acuity and correctly classified 80.0% of cases. The model showed that the OTS class was the only factor associated with final visual acuity (P<0.001). The lower the OTS class, the worse the visual acuity (Table 4).

Table 2 Characteristics of open globe injuries among patients (quantitative indicators)
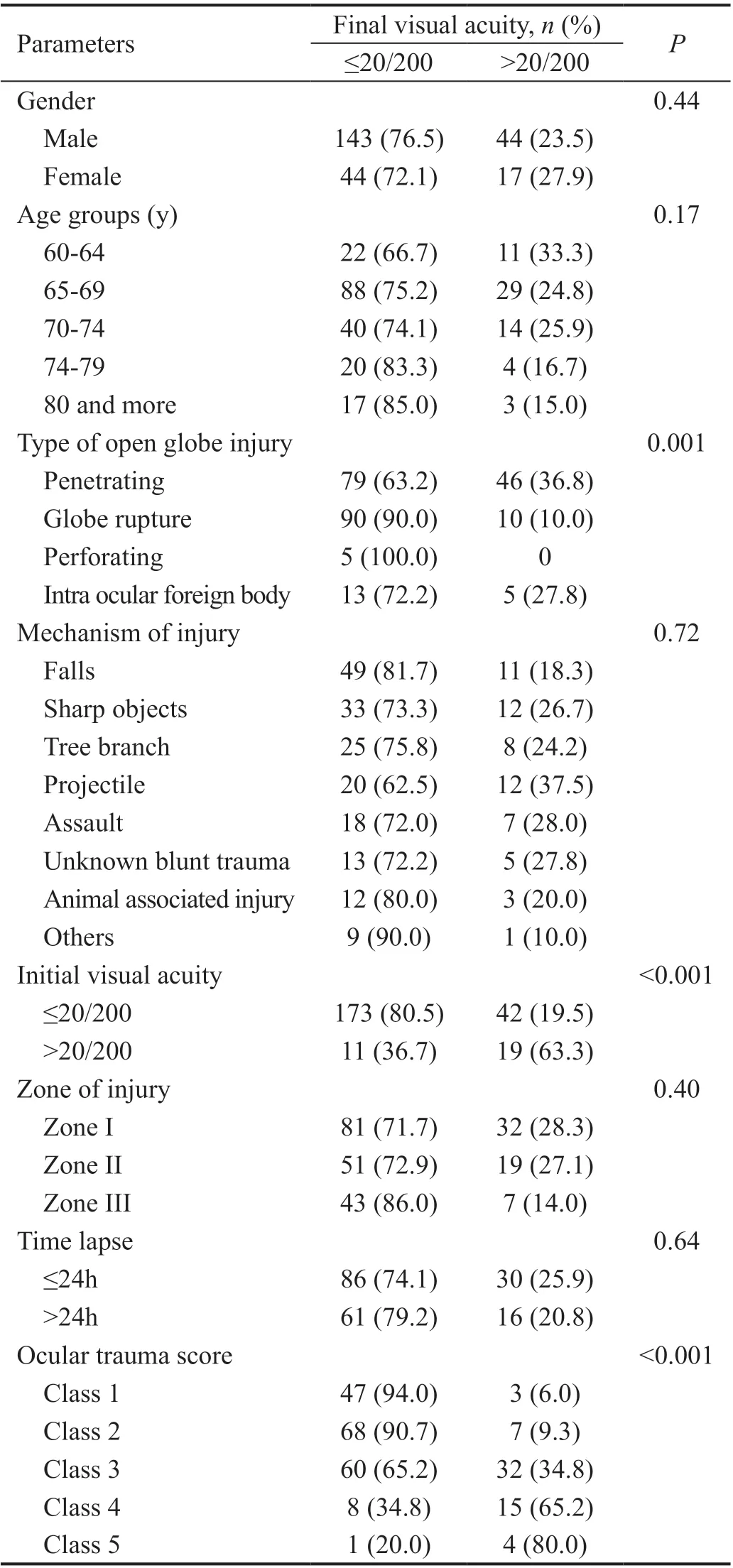
Table 3 Characteristics of open globe injuries among patients(categorical indicators)

Table 4 Final Logistic regression model
DISCUSSION
Published data on open globe injury in geriatric patients are limited. We tried to determine the pattern of ocular trauma and the prognostic factors for predicting the visual outcome in this population.
This study demonstrated a different pattern of open globe injury in geriatric patients than in other articles, as discussed further. Compared with other studies, males comprised most of our patients with the main type of injury being a penetrating injury[15-16]. Also, most of our patients were in their 60s and the number of injuries reduced in the 70s and 80s subgroups. Although one cannot say for sure, this mirrors the general hypoactive lifestyle of most people as they become progressively more elderly. One of the inclusion criteria of our study was 5y younger than Andreoliet al’s study[15], but even if we omit the population aged 60-64y, the mean age would be 70.3 and compared with Andreoliet al[15], our patients were significantly younger (P<0.001). Males were more frequently involved (77%vs42%). In addition, more patients in our study had injuries in the zone I despite zones II, III in that study. The mean raw OTS of our study was significantly higher than the Andreoliet al’s study[15](60.5vs47,P<0.001). Penetrating injuries comprise a large number of ocular traumas in our study. These indicate that many patterns of ocular trauma in our study are like younger patients as opposed to Andreoliet al’s study[15]. It may be related to an extended period of activity and being in work in our country.
The most common mechanism of injury was falling; however,the rate of sharp objects, projectile particles, and incidental tree branch stroke were notably high. Since the risk factors for falling such as aging, reduced vision, balance impairment, and cognitive disability accumulate in the elderly, it’s not a surprise to see a high frequency of falls among them[19-21].
It is invaluable for the physician to be able to predict the visual outcome and inform patients regarding a realistic expectation for rehabilitation. In our study, we evaluated the prognostic factors including age, type of open globe injury, time-lapse,initial visual acuity, the zone of injury, OTS (both raw and class values). The only prognostic factor that showed a statistically significant association with final visual acuity was the OTS class. The lower the OTS class, the worse the visual acuity. Since there was no reduction in final visual acuity for patients who underwent primary repair after 24h, we are encouraged that late presentations or delayed repairs in the elderly may obtain vision that is not statistically different from those who present immediately or are repaired more rapidly. It may be related to intact conjunctiva in rupture cases or ocular trauma in a less infectious situation in geriatrics.
This study was limited by its retrospective nature. Since Farabi Eye Hospital is a referral center with admissions from all over the country, many patients are followed by their primary care ophthalmologists outside our center. This restricted our follow up data on final visual acuity. Our follow‐up duration in this paper varies from 5 to 71mo.
We endeavored to determine the pattern of geriatric ocular trauma and the prognostic factors for predicting the outcome.The most common type of open globe injury in our country was penetrating injuries but falling remained the main cause.
The OTS classification is considered an important predictor of final visual acuity.
ACKNOWLEDGEMENTS
Conflicts of Interest: Zamani M,None;Tabatabaei SA,None;Fotouhi A,None;Naderan M,None;Soleimani M,None.
 International Journal of Ophthalmology2021年8期
International Journal of Ophthalmology2021年8期
- International Journal of Ophthalmology的其它文章
- Macular density alterations in myopic choroidal neovascularization and the effect of anti-VEGF on it
- ldentification and validation of tumor microenvironmentrelated lncRNA prognostic signature for uveal melanoma
- Factors associated with axial length elongation in high myopia in adults
- Visualizing the intellectual structure and recent research trends of diabetic retinopathy
- Therapeutic effect of Keap1-Nrf2-ARE pathway-related drugs on age-related eye diseases through anti-oxidative stress
- Newly-found functions of metformin for the prevention and treatment of age-related macular degeneration