
Macular density alterations in myopic choroidal neovascularization and the effect of anti-VEGF on it
2021-08-16 09:56:24JianBoMaoYiRunShaoJiaFengYuXinYiDengChenYiLiuYiQiChenYunZhangZhaoKaiXuSuLanWuLiJunShen
Jian-Bo Mao, Yi-Run Shao, Jia-Feng Yu, Xin-Yi Deng, Chen-Yi Liu, Yi-Qi Chen,Yun Zhang, Zhao-Kai Xu, Su-Lan Wu, Li-Jun Shen
1Department of Retina Centre, Affiliated Eye Hospital of Wenzhou Medical University, Hangzhou 310000, Zhejiang Province, China
2Department of Ophthalmology, Hangzhou Traditional Chinese Medicine Hospital Affiliated to Zhejiang Chinese Medical University, Hangzhou 310000, Zhejiang Province, China
3Chicago College of Optometry, Midwestern University,Downers Grove, Illinois 60515, USA
Abstract
INTRODUCTION
Myopic choroidal neovascularization (mCNV) is defined as choroidal neovascularization (CNV) secondary to pathologic myopia [refractive error <-6 D or axial length(AL) >26 mm, associated with complications of the posterior segment secondary to excessive elongation of AL], which has great impairment in vision and may cause legal blindness[1].Individuals (5.2%-11.3%) with pathologic myopia may develop mCNV, and approximately 15% of patients have bilateral CNV lesions[2].
Fundus fluorescein angiography (FFA) is the standard examination and is most commonly used to evaluate mCNV;however, it’s an invasive and time-consuming examination that has some risks for patients, such as anaphylactic shock[3].Optical coherence tomography angiography (OCTA) performs scans of areas of retinal tissue and constructs microvascular flow maps to evaluate the flow in various layers of the retina free of an injected dye[4]. Various studies compared OCTA and FFA and reported the potential of OCTA to diagnose and evaluate mCNV[5-7].
Anti-vascular endothelial growth factor (anti-VEGF) therapy is an effective therapy for mCNV. Αs a non‐invasive and fast technique, OCTA is commonly applied during the followup after anti-VEGF therapy. Several studies assessed the anti-VEGF therapy for mCNV by OCTA. Chenget al[8]demonstrated that the size of the CNV area and flow area decreased after the intravitreal administration of ranibizumab for 1wk and 1mo in 13 eyes. Cennamoet al[9]followed up 20 eyes and found that the neovascular area but not the vessel density by OCTA was decreased after ranibizumab therapy for 6mo. All these studies proved the reduction in CNV lesion after treatment.
OCTΑ can measure the vessel density of different retina layers.Previous studies found macular vessel density decreasing in high myopia (HM) eyes compared with normal eyes on OCTA[10-12]. However, whether the macular vessel density may alternate in HM eyes with secondary CNV and whether anti-VEGF treatment will impact the vessel density in mCNV eyes,few researches had been reported.
Our study is designed to follow-up before and until 1, 2, 3,and 6mo after anti-VEGF treatment and compare mCNV eyes before treatment with HM eyes and normal eyes on OCTA to know the variation tendency of CNV lesions and retinal vessel density.
SUBJECTS AND METHODS
Ethical ApprovalThis study followed the tenets of the Declaration of Helsinki and was approved by the Ethical Committee of Eye Hospital of Wenzhou Medical University(Grant No.2019-179-K-162). Informed consent was obtained from each patient before the study.
This study reviewed 41 patients (41 eyes) diagnosed with mCNV who received intravitreal anti-VEGF therapy from January 2016 to October 2018 at the Hangzhou Branch of Eye Hospital of Wenzhou Medical University. The same number of HM patients without other eye diseases whose age, sex and dioptre were matched with mCNV group were also included and defined as HM group. The same number of age‐matched normal persons were included and defined as normal group.
Criteria for mCNV group inclusion were: 1) refraction of myopia <-6 D or AL>26 mm; 2) hyperfluorescence in early phases and fluorescent leakage in the late phases on FFA(Spectralis, Heidelberg, Germany) and a hyperintense vascular anastomotic network on OCTA; 3) receive anti-VEGF therapy to treat mCNV; 4) follow‐up at least 6mo after first injection.Criteria for exclusion were: 1) idiopathic CNV or secondary CNV to other diseases; 2) accompanied with other eye diseases, such as age-related macular degeneration (AMD),central serous chorioretinopathy (CSC), polypoidal choroidal vasculopathy, glaucoma or ocular trauma; 3) treated by laser photocoagulation, photodynamic therapy or vitreoretinal surgery.
Anti-VEGF treatment regimen: intravitreal ranibizumab or conbercept 0.5 mg, a single injection followed by the treatment givenpro re nata(1+PRN). Retreatment criteria included any of the following findings during follow-up: 1) macular edema or subretinal fluid or serous retinal detachment in the optical coherence tomography (OCT) images; 2) CNV leakage on FFA; 3) new subretinal hemorrhage from the mCNV; 4)significant loss of visual acuity (VA).
The best-corrected VA (BCVA) was evaluated by standard logarithmic VA chart and was converted into logMAR for statistical analysis. The central macular thickness (CMT) was assessed by an ophthalmologist using the manual measurement of the distance between the inner limiting membrane and retinal pigment epithelium (RPE) at the fovea on OCT.Superficial vessel density, deep vessel density, foveal avascular zone (FAZ) area, A-circularity index (AI, perimeter/standard circle perimeter with equal area) and vessel density around the 300‐μm width of the FΑZ region density (FD), the area of CNV lesion were measured on 3×3 mm2OCTA images. The superficial vessel density and deep vessel density of retina and the area of the FAZ were assessed by OCTA. FAZ area was corrected for AL according to Lindermanet al’s[13]study, the formula was FAZ corrected (mm2)=FAZ (mm2)×(AL/ALM)2,ALM=23.95 mm. Superficial retinal vascular plexuses are defined as 3 μm underneath the internal limiting membrane to 15 μm underneath inner plexiform layer. Deep retinal vascular plexuses are defined as 15 μm to 70 μm underneath outer plexiform layer. Outer retina was defined as 70 μm underneath inner plexiform layer to 30 μm underneath RPE.Vessel density was automatically calculated by the software when segmentation was defined. In rare cases, automatically segmentation occurring error, manually segmentation was used to correct. The area of CNV was measured by the software when manually selecting the boundary of the lesion on outer retina. The scan quality was no less than 6. The reduction ratio of CNV lesions was the percentage of reduced area in pretreatment area. Data were compared of three groups, and of mCNV group before treatment and at each follow-up. The relationship between reduction ratio of CNV lesions and VA were also analysed.

Table 1 Demographic data of three groups
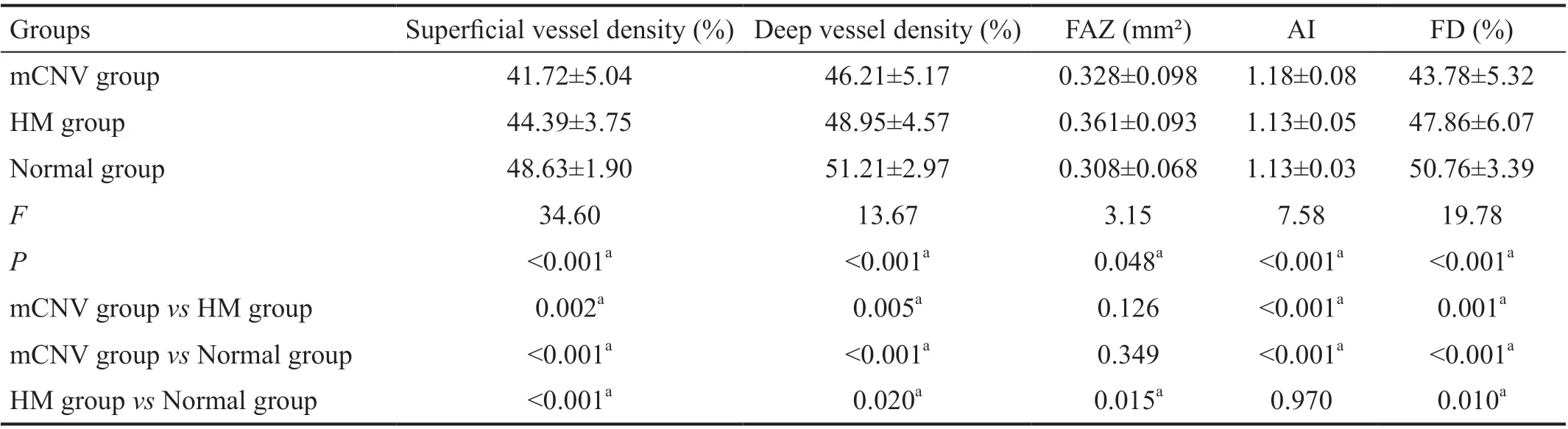
Table 2 OCTA parameters comparison of three groups
Statistical AnalysisStatistical analyses were performed using SPSS version 19.0 (SPSS 19.0, Inc., Chicago, IL, USA).All data were expressed as mean±standard deviation. The comparisons of mCNV group, HM group, and normal group,serial changes in logMAR BCVA, superficial vessel density,deep vessel density, CMT, the area of FAZ, the area and the flow area of CNV lesion, and CMT of mCNV group were analysed by one-way ANOVA. LSD-ttest was used in pairwise comparison. The relationship between different parameters was evaluated using Pearson’s correlation. Comparison of two groups (CNV area before treatment >0.5 mm2and ≤0.5 mm2)was used independentt-test. AP-value of less than 0.05 was considered statistically significant.
RESULTS
A total of 123 subjects were included in this study,including mCNV group (41 patients, 41 eyes), HM group (41 patients, 41 eyes), and normal group (41 patients, 41 eyes).Demographic data were showed in Table 1. There was no significant difference in age and sex among three groups(P>0.05). The mean diopter was -11.75±3.25, -11.66±2.85, and 0.07±0.89 D in mCNV group, HM group, and normal group respectively. The mean AL was 28.37±1.78, 27.98±1.12, and 23.89±0.56 mm respectively. There was no significant difference of diopter and ΑL between mCNV group and HM group (P>0.05). The mean logMAR BCVA was 0.56±0.30,0.09±0.10, and 0.03±0.06 respectively (F=101.3,P<0.001).Pairwise comparison showed significant difference between mCNV group and the other two groups (P<0.05).
Comparison of mCNV Group, HM Group, and Normal Group
Superficial vessel density of retinaThe mean superficial vessel density of retina was 41.72%±5.04%, 44.39%±3.75%,48.63%±1.90% respectively (F=34.60,P<0.001). Pairwise comparison showed significant difference among three groups(P<0.05; Table 2, Figure 1).
Deep vessel density of retinaThe mean deep vessel density of retina was 46.21%±5.17%, 48.95%±4.57%, 51.21%±2.97%respectively (F=13.67,P<0.001). Pairwise comparison showed significant difference among three groups (P<0.05).
Area of foveal avascular zoneThe mean corrected area of FAZ was 0.328±0.098, 0.361±0.093, and 0.308±0.068 mm2respectively (F=3.15,P=0.048). Pairwise comparison showed significant difference between mCNV group and normal group(P<0.05).
A-circularity indexThe mean AI was 1.18±0.08, 1.13±0.05,and 1.13±0.03 respectively (F=7.58,P<0.001). Pairwise comparison showed significant difference between mCNV group and the other two groups (P<0.05).
The 300 μm width of the FAZ region densityThe mean FD was 43.78%±5.32%, 47.86%±6.07%, and 50.76%±3.39%(F=19.78,P<0.001). Pairwise comparison showed significant difference among three groups (P<0.05).
Comparison of Pre-anti-VEGF and Post-anti-VEGF in mCNV Group

Figure 1 Superficial (A) and deep retinal vascular plexuses (B), outer retina (C) on OCTA mCNV patient (A1, B1, C1): Female, 58 years old, -9 D, AL 26.90 mm. HM patient (A2, B2, C2): Male, 50 years old, -16 D, AL 26.56 mm. Normal person (A3, B3, C3): Female, 53 years old,-0.25 D, AL 24.49 mm. FAZc was corrected FAZ area.
BCVA logMARThe mean times of intravitreal injection were 1.88±0.87. Twenty two eyes were injected with ranibizumab,and 19 eyes were injected with conbercept. The mean logMAR BCVA was 0.56±0.30 at baseline and 0.41±0.27, 0.33±0.27,0.31±0.26, and 0.30±0.27 at 1, 2, 3, and 6mo follow-up,respectively (Figure 2). The difference between logMAR BCVA at baseline and at 1, 2, 3 and 6mo follow-up was statistically significant (F=6.848,P<0.05). The intravitreal anti-VEGF therapy improved the logMAR BCVA at 1-month(P<0.05), 2-month (P<0.05), 3-month (P<0.05), and 6-month follow-ups (P<0.05;Table 3).
Superficial vessel density of retinaThe mean superficial vessel density of retina was 41.72%±5.04% at baseline,41.57%±4.88%, 41.11%±6.22%, 42.93%±4.78%, and 41.08%±5.72% at 1, 2, 3- and 6-month follow-up, respectively.There was no significant difference before and after the treatment (F=0.803,P>0.05).
Deep vessel density of retinaThe mean deep vessel density of retina was 46.21%±5.17% at baseline and 44.76%±4.00%,45.51%±4.68%, 45.54%±4.36%, and 46.16%±5.85% at 1, 2, 3- and 6-month follow-up, respectively. There was no significant difference between them
Area of foveal avascular zoneThe mean FAZ area was 0.328±0.098 mm2at baseline and 0.315±0.088, 0.331±0.092,0.343±0.082, and 0.348±0.084 mm2at 1, 2, 3- and 6-month follow-up, respectively. There was no significant difference between them (F=0.878,P>0.05).
A-circularity indexThe mean AI was 1.18±0.08 at baseline and 1.15±0.06, 1.16±0.05, 1.17±0.08, and 1.16±0.04 at 1, 2, 3-and 6‐month follow‐up, respectively. There was no significant difference between them (F=1.13,P>0.05).
Foveal avascular zone regionThe mean deep vessel density of retina was 43.78%±5.32% at baseline and 44.67%±4.71%,45.82%±6.77%, 45.38%±5.64% and 44.50%±5.25% at 1, 2, 3-and 6‐month follow‐up, respectively. There was no significant difference between them (F=0.829,P>0.05).
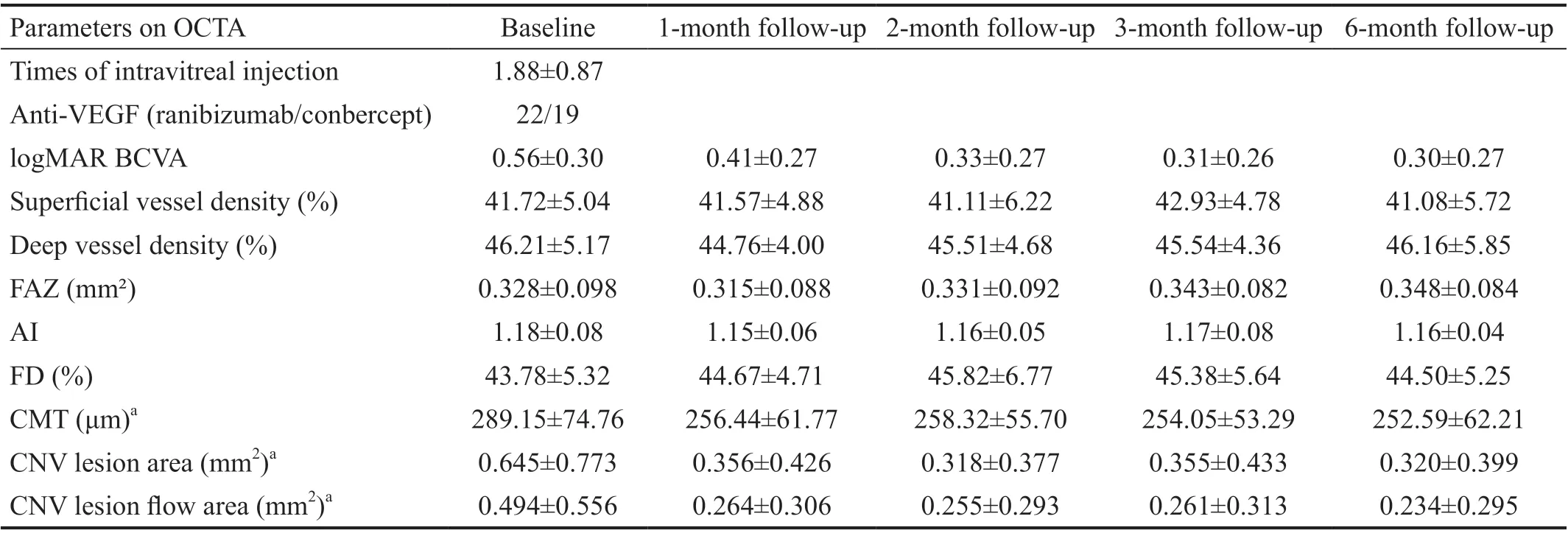
Table 3 Data of the mCNV patients
Central macular thicknessThe mean CMT was 289.15±74.76 μm at baseline and 256.44±61.77, 258.32±55.70,254.05±53.29, and 252.59±62.21 μm at 1, 2, 3‐ and 6‐month follow-up, respectively (Figure 3). The difference between the CMT at baseline and at each follow-up was statistically significant (F=2.489,P<0.05). However, there was no difference in the values of CMT between 1, 2, 3‐ and 6‐month follow-up.
Area and flow area of CNV lesionThe mean area of CNV lesion was 0.645±0.773 mm2at baseline and 0.356±0.426,0.318±0.377, 0.355±0.433, and 0.320±0.399 mm2at 1, 2, 3- and 6-month follow-up, respectively (Figure 4). The mean flow area of CNV lesion was 0.494±0.556 mm2at baseline and 0.264±0.306, 0.255±0.293, 0.261±0.313, 0.234±0.295 mm2at 1, 2, 3- and 6-month follow-up, respectively (Figure 5). The difference between the area (F=3.125,P˂0.05) and flow area(F=3.558,P<0.05) of the CNV lesion at baseline and at each follow‐up was statistically significant. However, there was no difference between 1, 2, 3‐ and 6‐month follow‐up. Αlthough the area of the CNV lesion reduced after injection, in most patients (95.12%), it didn’t disappear even when its activity had been controlled. The mean reduction ratio of lesions was 50.32% (7.07% to 100%). In only two cases, 100%lesion regression was observed (4.88%).
T-testWe divided the patients into two groups according to the CNV area before treatment (>0.5 and ≤0.5 mm2).The reduction ratio in the two groups was compared using independentt-test (t=2.136,P=0.042). The reduction ratio in the group with pre-anti-VEGF CNV area >0.5 mm2was smaller than the other group.

Figure 2 The tendency of logMAR BCVA The error bars represent the variance of the mean value.
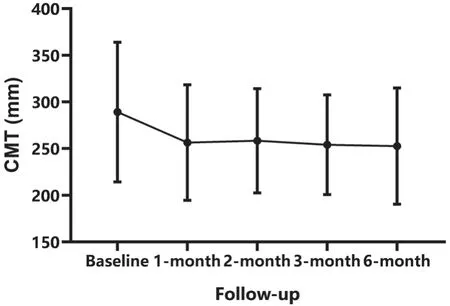
Figure 3 The tendency of CMT The error bars represent the standard deviation of the mean value.
Correlation AnalysisThe Pearson correlation analysis showed the negative correlation between the area of the CNV lesion and the reduction ratio (r=-0.380,P=0.042) and between the flow lesion area and the reduction ratio (r=-0.402,P=0.030). There is no significant difference between the reduction ratio and other factors, such as age, logMAR BCVA,and CMT before treatment and the improvement of BCVA.Figures 6 and 7 showed 2 cases of mCNV patients accepting anti-VEGF.
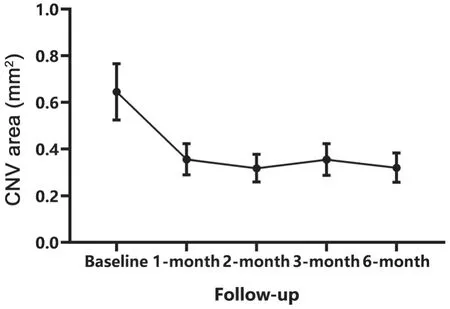
Figure 4 The tendency of the area of CNV lesion The error bars represent the variance of the mean value.
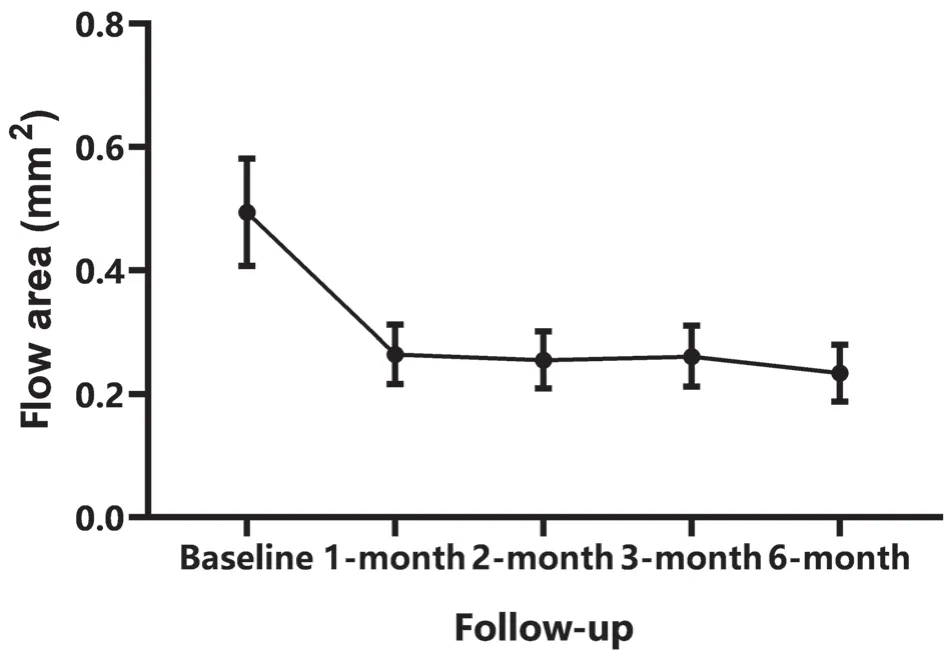
Figure 5 The tendency of the flow area of CNV lesion The error bars represent the variance of the mean value.

Figure 6 A 33-year-old female with mCNV in the right eye, the refraction of myopia was -7.0 D and the logMAR BCVA was 0.1 The lesion disappeared completely after one intravitreal ranibizumab injection, and the logMAR BCVA was improved to 0.
DISCUSSION
In this study, we analysed the macular microvascular parameters on OCTA in mCNV patients which was divided into two parts. First, we compared mCNV group, HM group and normal group and found the logMΑR BCVΑ, superficial and deep vessel density and FD of mCNV group were lower than HM group and normal group, the superficial and deep vessel density and FD of HM group were lower than normal group. The FAZ area in HM patients was bigger than that in normal person, but there was no significant difference between mCNV and the other two groups. To some extent, FAZ in mCNV patients may turn smaller. The mean AI of mCNV group was statistically bigger than the other two groups which means the FAZ was more irregular. Second, we compared mCNV patients pre-anti-VEGF and post-anti-VEGF (including 1, 2, 3- and 6-month) and found logMAR BCVA get better, the CMT, the area and flow area of CNV lesion decreased, The reduction ratio of biggest lesion group (>0.5 mm2) was less than the smaller. but superficial and deep vessel density, the area of FAZ, AI and FD didn’t change in mCNV group after anti-VEGF treatment.
Our study further discovered that the superficial and deep vessel density and FD decreased more in mCNV group. Some scholars considered that breaks in RPE-Bruch’s membrane induced by the excessively long AL develop lacquer cracks which facilitates ingrowth of neovascular[14]. We guess the excessively long AL in mCNV caused lower vessel density.Choroidal ischemia up regulation the VEGF factors is also a hypothesis of the pathogenesis of mCNV[15]. Decreasing superficial and deep vessel density and FD may have the same effect on VEGF. However, there was no significant difference between in the superficial and deep vessel density and FD in mCNV group before and after treatment. The alterations in vessel density may exist before CNV emerged, if this assumption was true, it might mean the lower vessel density indicate the higher risk of mCNV. However, we can’t exclude the possibility of anti-VEGF inefficient on influencing the vessel density.
Lindermanet al[13]found not correcting for AL introduced errors up to 31% in FAZ area and described the correct methods which were used in our study. Sunget al[16]used Littmann’s formula to correct FAZ for AL and found FAZ was larger in high myopia patients. We concluded the same result.However, FΑZ in mCNV group have no significant difference with the other two groups. Tanet al[17]found FAZ area was affected by central retinal thickness and central choroidal thickness. CMT became thicker and central choroidal thickness became thinner in mCNV eyes. It may suggest that the FAZ area in mCNV group may turn smaller. CMT turned thinner after anti-VEGF treatment, the FAZ area didn’t change. We guess the FAZ destruction caused by the CNV lesion was irreversible. High myopia didn’t change the form of FAZ but the form of FAZ became irregular in mCNV group.

Figure 7 A 58-year-old female with mCNV in the right eye, the refraction of myopia was -9.5 D and the logMAR BCVA was 0.7 The lesion just became smaller but still existed after three times intravitreal conbercept injection, and the logMAR BCVA was improved to 0.15.
Previous studies reported the superficial and deep density decreased in high myopic patients compared with normal controls, which were consistent with the results in our study.Liet al[10]found microvascular density of superficial and deep vascular plexuses and annular zone decreased in high myopia eyes prior to permanent retinal damage compared to healthy controls and speculated that elongation of AL result in destruction in RPE cells and then caused decreasing in vessel density. Yanget al[11]came to the same conclusion and revealed the reduction in vessel density correlates with AL elongation.Superficial and deep macular vessel density is lower in high myopia compared with middle myopia and healthy control, as well as in middle myopia compared with healthy control[12].
In this study, anti-VEGF therapy is an effective treatment for mCNV which improved BCVA and reduced CNV lesions and CMT. However, anti-VEGF therapy could not eliminate the mCNV lesions completely in most cases (95.12%) 6mo after treatment. The mean reduction ratio of lesions of 41 patients was 50.32% (varying from 7.07% to 100%). CNV is affected by various factors, such as interleukin 8 (IL8); monocyte colonization protein (MCP),etc[18]. Simple anti-VEGF probably can’t block all the factors that induce CNV. New treatments, such as anti-VEGF associated with other factors antagonists, are needed to be studied in the future.
There were two cases (4.88%) who reached complete disagreement of CNV lesions at 6-month follow-up. In both cases, the CNV lesions at baseline were relatively small (0.076 and 0.222 mm²) and the patients were young (26 and 33 years old). We speculate that the size of lesions and the age of patients may be the factors related to the complete regression of the lesions. According to the Pearson correlation analysis,we found that the smaller lesions would regress more (r=-0.380,P=0.042). According to independentt-test, the reduction ratio in the group with pre-anti-VEGF CNV area >0.5 mm² was smaller than the other group.
Previous research studies on the treatment for CNV secondary to AMD by OCTA found that anti-VEGF therapy only prunes subtle small newly growing vessels and does not achieve vascular normalization[19-20]. Chenget al[8]researched mCNV and found attenuation in capillaries and small caliber feeder vessels but not in large caliber feeder vessels treated by intravitreal Ranibizumab. Caiet al[21]found vascular lesion and capillary density decreased after intravitreal ranibizumab in mCNV eyes on OCTA. We guess the reasons for larger lesions leading to a lower reduction ratio are as follows: 1)larger lesions more likely have bigger feeder vessels that are more difficult to clear up; 2) larger lesions are more likely to be old lesion which feeder vessels have been formed that are difficult to regress. There is no correlation between the lesion area and age. Maybe those two young persons had a better consciousness of visiting clinic leading to earlier treatment and better prognosis. Besides, we didn’t find other factors that are related to the regression rate; thus, further studies are needed.In this study, the BCVA of patients improved but without relationship with the reduction ratio. We suspected that the BCVΑ was affected by various factors, such as age, ΑL, former fundus condition, duration of mCNV,etc. We didn’t perfectly control these variables of the patients enrolled in our study. It is not enough to prove that VA and reduction ratio are irrelevant.We also analysed the other parameters measured by OCTA to investigate the efficiency of anti‐VEGF. The CNV lesion area,the flow area of CNV lesion and CMT reduced mostly at the first month after injection and was stable in the following 5mo,which indicates that the anti‐VEGF therapy is mainly effective during the first month. The FΑZ, superficial vessel density and deep vessel density didn’t change before and after treatment.There are some limitations to this study. The number of patients enrolled was relatively small. The type of anti-VEGF therapy used was not identical for all the patients, the efficiency of ranibizumab and conbercept might be different.Thus, further studies may expand the number of samples and carry out control studies of ranibizumab group and conbercept group.
In conclusion, macular vessel density decreased, FAZ turned smaller and more irregular in mCNV eyes. Anti-VEGF therapy is efficient for mCNV but unable to changing vessel density and FAZ and eliminate CNV lesions completely in most cases,the the mean reduction ratio is 50.32%, the bigger mCNV lesions have lower reduction ratio. Further studies are needed to find new treatments to cure mCNV.
ACKNOWLEDGEMENTS
Authors’ contributions:Mao JB and Shao YR contributed to the conception and design of the study, data collection, analysis and interpretation of data, writing the article, final approval of the article. Yu JF, Deng XY, Liu CY, Chen YQ, Zhang Y,Xu ZK, Wu SL contributed to data collection, analysis and interpretation of data, final approval of the article. Shen LJ contributed to the conception and design of the study and final approval of the article.
Foundation:Supported by Medical and Health Platform Project of Zhejiang Province (No.2021KY810).
Conflicts of Interest: Mao JB,None;Shao YR,None;Yu JF,None;Deng XY,None;Liu CY,None;Chen YQ,None;Zhang Y,None;Xu ZK,None;Wu SL,None;Shen LJ,None.
 International Journal of Ophthalmology2021年8期
International Journal of Ophthalmology2021年8期
- International Journal of Ophthalmology的其它文章
- Mid-term results of patterned laser trabeculoplasty for uncontrolled ocular hypertension and primary open angle glaucoma
- Combined ab-interno trabeculectomy and cataract surgery induces comparable intraocular pressure reduction in supine and sitting positions
- Comparison of the SlTA Faster–a new visual field strategy with SlTA Fast strategy
- Evaluating newer generation intraocular lens calculation formulas in manual versus femtosecond laser-assisted cataract surgery
- Conjunctival flap with auricular cartilage grafting: a modified Hughes procedure for large full thickness upper and lower eyelid defect reconstruction
- Improvement of human embryonic stem cell-derived retinal pigment epithelium cell adhesion, maturation, and function through coating with truncated recombinant human vitronectin