
Effects and safety of Ding Kun Dan on lVF/lCSl-ET outcomes in patients with predicted poor ovarian response:A multicenter randomized clinical trial
2021-08-06 05:36SaihuaMaGuiminHaoJiayiSongZhimeiZhaoBaojuanWangXueruSongFengqinXuYanLiuTianXia
TMR Modern Herbal Medicine 2021年3期
Saihua Ma,Guimin Hao,Jiayi Song,Zhimei Zhao,Baojuan Wang,Xueru Song,Fengqin Xu,Yan Liu,Tian Xia*
1 Reproductive Center,First Teaching Hospital of Tianjin University of Traditional Chinese Medicine,Tianjin 300112,China;
2 Center of Reproductive Medicine,The Second Hospital of Hebei Medical University,Shijiazhuang 050000,China;
3 Center of Reproductive Medicine,General Hospital of Tianjin Medical University,Tianjin 300052,China;
4 Center of Reproductive Medicine,Tianjin First Center Hospital,Tianjin 300190,China.
Abstract Objective:To evaluate whether Ding Kun Dan(DKD)can improve the vitro fertilization/ intracytoplasmic sperm injection and embryo transfer(IVF/ICSI-ET)outcomes in patients with predicted poor ovarian response(POR)safely and effectively.Methods:Prospective,multicenter,randomized controlled trial;A total of 278 POR patients were randomized in DKD group or immediate treatment group.Both groups received IVF or ICSI as a standard treatment while in the DKD group,DKD was administrated for 3 months before the IVF/ICSI cycle.The primary outcome was the ongoing pregnancy rate.The secondary outcomes include clinical pregnancy rate,biochemical pregnancy rate,total gonadotropin(Gn)dosage and duration,estradiol(E2)and progesterone(P)levels on human chorionic gonadotropin(hCG)trigger day,cycle cancellation rate,number of oocytes retrieved,high-quality embryo rate and any adverse events.Results:Compared to the immediate IVF treatment group,oral administration of DKD for 3 months before IVF led to a significant increase in ongoing pregnancy rate(30.0% v.s.17.6%,P < 0.05),biochemical pregnancy rate(39.2% vs.25.2%,P < 0.05),clinical pregnancy rate(36.7% vs.22.7%,P < 0.05)and highquality embryo rate(40.8% vs.32.4%,P < 0.05),and a significant decrease in Gn duration(P < 0.05).However,no significant differences were found in total dosage of Gn,number of retrieved oocytes,cycle cancellation rate,E2 level and P level on hCG trigger days(P > 0.05).No serious adverse events occurred during the intervention period in either group.Conclusion:DKD is a safe and effective intervention to improve the IVF/ICSI-ET outcomes in patients with POR.
Keywords:Traditional Chinese medicine,Ding Kun Dan,Poor ovarian response,In vitro fertilization,Intracytoplasmic sperm injection
Background
Poor ovarian response(POR)refers to a poor response to gonadotrophins(Gn)stimulation in assisted reproductive technology(ART),which is characterized by a decreased production and quality of follicles/oocytes and an increased cancellation rate during in vitro fertilization / intracytoplasmic sperm injection and embryo transfer(IVF/ICSI-ET).POR accounts for a significant portion(9-24%)of patients undergoing ovarian stimulation for assisted reproduction[1].Diminished ovarian reserve(DOR)is an important cause of POR.However,some women younger than 35 years with predicted normal ovarian function may also present a diminished response to controlled ovarian hyperstimulation(COH),which is called unexpected poor ovarian responses(UPOR)accounting for 21.16% in IVF/ICSI-ET[2].The latest ART annual report from the Center for Disease Control shows that among women age 38 or younger,the percentage of ART cycles resulting in pregnancy was 29.5-35.9%,the percentage of ART cycles resulting in live births was 24.0-31.0%[3].While in the same year,a research lasting 15 years and involving 3391 POR participants reveal that the clinical pregnancy rate was 14% per oocyte retrieval,and the live birth rate per cycle was 9.6%,which were significantly lower than the average[4].Moreover,the cumulative live birth rate is likely to decrease significantly with age,which has a significant difference between older than 38 years and younger POR(10.5-13.5% vs 17.2-22%),and the cumulative live birth rate of women older than 43 year is as low as 4.4%,which is extremely unfriendly for advanced age women and planning to have a second child women.
The lower pregnancy rate,more Gn dosage and COH treatment impose more emotional,physical,and financial burdens for POR patients[5].Depressingly,for these patients,there is still no proven effective treatment.Attempts have been made to improve the ovarian response of POR patients,such as administration of androgen agonists or antagonists prior to COH,oral administration of contraceptives,estradiol or supplement of growth hormones and modified COH protocols such as minimal ovarian stimulation,antagonists or ovulation induction in the luteal phase[6,7].However,it is disappointing that the pregnancy rate is still far from being satisfactory.Therefore,Giovanale,et al.[8]propose that different treatment methods to standardize diagnosis and treatment of POR should be researched,and present that any treatment which could increase the pregnancy rate of POR should be attempted.
The traditional Chinese medicine(TCM)treatment for infertility has a long history in China.There is substantial evidence that TCM as a complementary therapy can significantly improve ovarian response and embryo implantation rate,leading to better pregnancy outcomes in POR patients undergoing IVF/ICSI-ET[9,10].Ding Kun Dan(DKD;Guangyuyuan Traditional Chinese Medicine Co.LTD.,China)is a well-known TCM first prescribed 200 years ago in the reign of Emperor Qianlong(1736-1796),and it is now widely used in the treatment of difficult and complicated gynecological diseases such as polycystic ovarian syndrome(PCOS)and infertility due to DOR[11,12].According to the clinical experience of our team,we find DKD could significantly improve the ovarian reserve and pregnancy rate of POR patients.Wei et al.[13].explore the influences of DKD combined with micro stimulation on the outcomes in patients with POR.They concluded that,comparing to micro stimulation,DKD combined with micro stimulation could significantly improve the levels of serum estradiol(E2)on human chorionic gonadotropin(hCG)trigger day,endometrial thickness,number of retrieved oocytes,fertilization rate,quality embryo rate,embryo implantation rate and clinical pregnancy rate,reduce total dosage and duration of Gn stimulation,cancellation rate of POR.However,this study still has some limitations such as shorter DKD treatment duration and smaller sample size.In order to address these limitations,we conducted a multicenter randomized clinical trial to evaluate the effect of DKD on IVF/ICSI-ET outcomes in a large sample of POR patients.
Methods
Participants
A total of 278 predicted POR patients were recruited from the Second Hospital of Hebei Medical University(Hebei,China),Tianjin Medical University General Hospital(Tianjin,China)and Tianjin First Center Hospital(Tianjin,China)from May 2017 to July 2019.The number of completed cases in each subcenter was 142,64,72.Informed consent was obtained from all patients.Eligible participants were randomly assigned to the DKD group(DKD for 3 months,then IVF/ICSI)or the immediate treatment group(immediate IVF/ICSI)in a 1:1 ratio by central randomization performed by an independent statistician from Tianjin CLINDA Medical Technology Co.,Ltd.Random numbers were generated by using dynamic randomization on an online computer,which generated a randomization schedule.Briefly,patients in the DKD group(n = 139)received IVF/ICSI-ET after the administration of DKD for 3 months,while patients in the immediate treatment group(n = 139)had immediate IVF/ICSI-ET,with no DKD treatment.These patients were observed for a further 3 months after IVF/ICSI-ET and if pregnant,were followed up to determine if there was an ongoing clinical pregnancy.
The inclusion criteria were as follows:(1)aged between 25 and 38 years;(2)normal and regular menstrual cycle(25-35 days);(3)diagnosed as being likely to have POR where at least two of the following three features must be present:the number of retrieved oocytes ≤ 5 with a conventional ovarian stimulation protocol in a previous cycle;antral follicle count(AFC)<7;and anti-Mullerian hormone(AMH)concentration< 1.1 ng/ml;(4)with a diagnosis of infertility:no pregnancy achieved after attempting pregnancy through regular unprotected intercourse for a year in women aged ≤ 35 or for 6 months in women aged > 35;(5)patients undergoing IVF/ICSI-ET;and(6)volunteering to participate and signed the informed consent.
The exclusion criteria were as follows:(1)coexisting endocrine and autoimmune diseases such as polycystic ovary syndrome,hyperprolactinemia,hyperandrogenism,thyroid dysfunction and diabetes;(2)co-existing reproductive system diseases such as endometriosis,endometrial tuberculosis,intrauterine adhesions,hysteromyoma(submucous myoma or nonsubmucous myoma with a diameter >4 cm and/or endometrial compression),uterine malformation(uterus duplex,bicornis,unicornis and mediastinum)and hydrosalpinx;(3)history of severe medical,surgical and mental diseases;(4)history of hereditary or acquired diseases in one or both members of the couple;(5)the woman having received hormone medicines such as contraceptive agents and glucocorticoids within the past three months;and(6)being allergic to drugs used in this study.
The study protocol was registered in the Chinese Clinical Trial Register(No.ChiCTR-IOR-17011697)and approved by the Ethics Committee of the First Affiliated Hospital of Tianjin University of Traditional Chinese Medicine(No.TYLL2017[K]004).The protocol was published in Trials[14].
Treatment
In brief,the patient was first seen by the clinic doctor,and if thought to be eligible for the trial was then reviewed by the principal investigator(PI)in each participating center.If eligible,and the patient agreed to participate,the patient was consented and randomized to either 3 months DKD,followed by IVF/ICSI-ET,or immediate IVF/ICSI-ET.The clinic doctor treated the patient for IVF/ICSI-ET,and the PI treated the patient with DKD.
Patients in the DKD group received oral administration of 7 g of DKD twice a day(morning and evening)from the first day of menstruation for three consecutive months.The dose of DKD could be reduced to 3.5 g twice daily if the patient experienced uncomfortable symptoms such as oral ulcers or swollen and sore gums.IVF/ICSI-ET was performed upon the completion of DKD treatment,and patients were followed up for three months if they were pregnant.Patients in the control arm did not receive DKD and had immediate IVF/ICSI-ET.They were also followed up for three months after IVF/ICSI-ET,and if pregnant followed up for a further 3 months.
IV F procedure
Both DKD and immediate treatment group received the Gn/antagonist protocol as follows.Patients were subcutaneously injected with 300U/d Gonal-F(rFSH,Merck Serono,Switzerland)from the third day of menstruation,and the dose could be adjusted by the treating physician according to the number of follicles and hormone levels.As the diameter of dominant follicles reached 13-14mm or the serum E2concentration was higher than 350pg/ml,0.25mg/d cetrorelix acetate(Merck Serono,Switzerland)or ganirelix acetate(ORGALUTRAN®,Merck Sharp &Dohme Ltd.,USA)was subcutaneously injected whilst continuing the rFSH daily injection.When more than one follicle with a diameter of ≥ 18 mm was detected,250μg of Ovidrel(rhCG,Merck Serono,Switzerland)was administered and oocytes were collected under transvaginal sonography guidance 34-36h later.
IVF or ICSI was performed according to the sperm quality.Embryo transfer was performed 2-3 days after oocyte collection,and remaining high-quality embryos were cryopreserved.A cycle which did not result in transferable embryos was considered as a cycle cancellation.Cleavage-stage embryos could be classified into three grades according to the number of cleavage-stage embryos,blastomere development and the ratio of fragmentation[15]:first-grade or highquality embryos are characterized by < 10%fragmentation,stage-specific cell size and no multinucleation;second-grade or fair-quality embryos are characterized by 10-25% fragmentation,stagespecific cell size for majority of cells and no evidence of multinucleation;and third-grade or poor-quality embryos are characterized by severe fragmentation(>25%),cell size without stage specificity and evidence of multinucleation.
After embryo transfer,patients were treated with 90mg of progesterone vaginal gel(Crinone gel®,8%,Merck Serono,Switzerland)daily or 10mg twice daily dydrogesterone(Duphaston®,Abbott Biologicals B.V.,Netherlands)orally.Serum human chorionic gonadotropin(β-hCG)was measured on the 14th day after embryo transfer,and a β-hCG level >25U/L indicated a biochemical pregnancy.If positive,the serum β-hCG was re-examined two days later.Transvaginal ultrasound was performed 4-6 weeks after embryo transfer,and the presence of gestational sac and fetal heart pulsation indicated clinical pregnancy.Transvaginal ultrasound was repeated if necessary to confirm a viable pregnancy.For patients with a positive pregnancy test,luteal support therapy was continued until gestational age of 12 weeks,at which time an ultrasound was performed to assess fetal viability.
Outcomes
The primary outcome of the study was the ongoing pregnancy rate,defined by at least one intrauterine viable fetal heart beat at 12 weeks of gestation;and the secondary outcomes include biochemical pregnancy rate,clinical pregnancy rate,number of retrieved oocytes,high-quality embryo rate,cancellation rate,total dose and duration of Gn stimulation,E2and progesterone(P)level at the day of hCG injection,baseline levels of follicle-stimulating hormone(FSH),anti-Mullerian hormone(AMH)and antral follicle count(AFC).The safety indicators considered in this study include(1)possible adverse events following drug administration;(2)general physical examination,temperature(T),pulse(P),respiration(R)and blood pressure(BP);(3)blood and urine examination for liver function such as alanine aminotransferase(ALT)and aspartate aminotransferase(AST)levels,renal function such as creatinine(Cr)and urea nitrogen(BUN)levels,and(4)electrocardiogram(ECG),breast and gynecological color ultrasound.
Sample size
The minimum sample size required in this study was determined mainly based on the ongoing pregnancy rate.It is reported that the ongoing pregnancy rate is 12.5-15.8% with an average of 13% in POR patients[16-19].Based on our clinic experience,we assumed that DKD would lead to an increase in the ongoing pregnancy rate to 26%.The sample sized was calculated according to the following equation:
n=(Zα+Zβ)2[P1(1-P1)+P2(1-P2)]/(ε-δ)2
where α = 0.05 is the significance level,β is set to 0.8,Zα is set to 1.64,Zβ is set to 0.84,and the limit δ is set to 0.
Therefore,the study is expected to have an 80%power to detect a 13% increase of the ongoing pregnancy rate when 112 cases are included in each group.We expected a discontinuation rate of 20%,so,the final sample size of each group was determined to be 139.No limit was set to the number of participants in each center.
Statistical analysis
All statistical procedures were performed in this study using SAS 9.4 software.Categorical data were expressed as percentage(%)and compared using the χ2test;measurement data were expressed as mean ±standard deviations and compared using the t test.Twosided test was used,andP< 0.05 was considered as significance level.
Results
Baseline Characteristics
The CONSORT flow diagram is shown in Figure 1.Patient characteristics are presented in Table 1.Table 1 shows that there were no significant differences in age,body mass index(BMI),duration of infertility,baseline FSH,E2level,AMH level and AFC between the two groups(P> 0.05).

Figure 1.CONSORT flow diagram of the study.*Data were removed(the 39 patients who failed to received treatments)
Primary outcome
An ongoing pregnancy was achieved in 36 patients(30.0%)in the DKD group and 21 patients(17.6%)in the immediate treatment group(P< 0.05)(Table 2).
Secondary outcome
Compared to the immediate treatment group,oral administration of DKD for 3 months led to a significant increase in biochemical pregnancy rate(39.2% vs.25.2%,P< 0.05),clinical pregnancy rate(36.7% vs.22.7%,P< 0.05)and high-quality embryo rate(40.8%vs.32.4%,P< 0.05),and a significant decrease in Gn duration(P< 0.05).While,oral administration of DKD for 3 months led to a significant increase in natural pregnancy(9.2% vs.0.8%,P< 0.05)(Table 2),comparing to the control group.However,no significant differences were found in total dose of Gn stimulation,number of retrieved oocytes,cycle cancellation rate,E2level and P level on the day of hCG(P> 0.05)(Table 2).
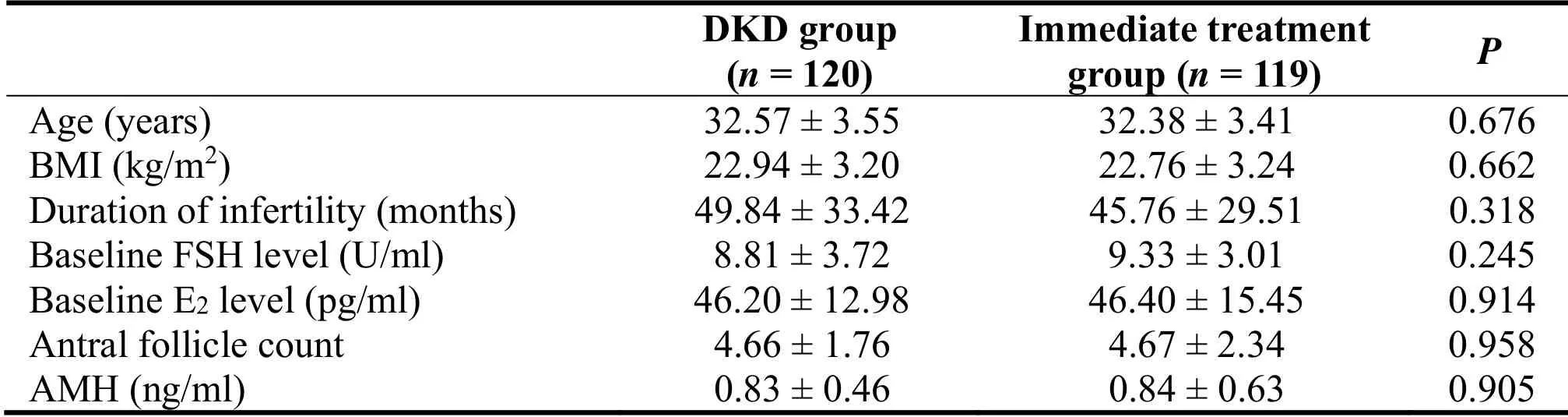
Table 1.Baseline characteristics of the DKD group and the Immediate treatment group
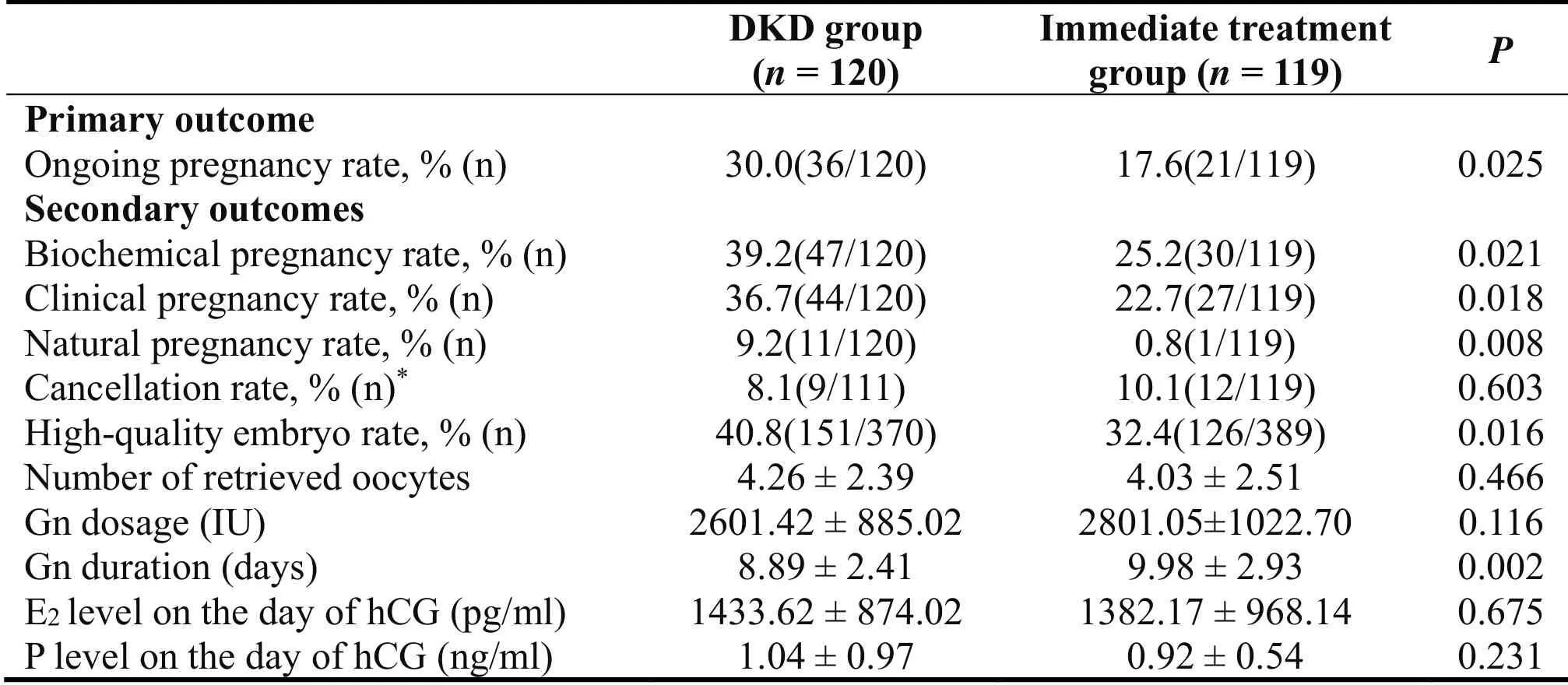
Table 2.Comparison of primary and secondary outcomes between the two groups

Table 3.Comparison of ovarian function before and after DKD treatment
There were no significant differences in baseline FSH and E2level before and after DKD treatment(P>0.05).However,the average AFC and AMH level increased significantly after DKD treatment(P< 0.05)(Table 3).
Adverse Events
No serious adverse events occurred during the intervention period in either group.Constipation occurred in two patients,stomach discomfort occurred in three patients,and sore throat occurred in one patient in the DKD group,which was improved upon reducing the DKD dose to 3.5g.Moderate ovarian hyperstimulation syndrome occurred in one patient in the immediate treatment group,which was resolved with conservative treatment.
Discussion
A poor ovarian response to exogenous Gn stimulation in COH can result in a reduction in the number of retrieved oocytes and transferrable embryos highquality embryos,a high cancellation rate and a low clinical pregnancy rate.POR remains an important cause of the failure of ART.The prognosis of POR differs substantially depending on the age and the number of retrieved oocytes[20].A higher age is associated with a lower number of retrieved oocytes[21],a higher frequency of aneuploidy of blastocyst[22]and a lower pregnancy rate[4].Oocyte maturity and quality are also important factors.Oocytes that have not developed through meiosis to MII are immature and are not able to be successfully fertilized,and if >25%of the oocytes were immature,then successful fertilization with clinical pregnancy would be greatly reduced[23].The quality of oocytes retrieved after COH can have an important effect on pregnancy outcomes,thus it is critical to improve the quality of oocytes in POR patients.
Our study demonstrated that treatment with DKD for 3 months prior to IVF,compared to immediate IVF then waiting 3 months did not negatively affect the chances of an ongoing pregnancy(the primary outcome),but likely improved it.Notably,the ongoing pregnancy rate was 30.0% in the DKD group,which was significantly higher than 17.6% in the immediate IVF group.Moreover,the biochemical pregnancy rate and clinical pregnancy rate were significantly increased in DKD group.Whilst the number of eggs retrieved were the same in both arms,ovarian function improved,as evidenced an increase in AFC,AMH level,highquality embryo rate,biochemical pregnancy rate,clinical pregnancy rate and ongoing pregnancy rate.Whilst the clinician was not blinded to the treatment arm,and so might have affected the AFC assessment,the embryologists were blinded to the DKD arm and pregnancy data are objective outcomes.
In our study,9 patients became pregnant naturally during the study period in the 3 months prior to IVF and 2 patients within the 3 months after IVF in the DKD group,compared to 1 patient within the 3 months after IVF in the immediate treatment group(9.2% vs.0.8%,P<0.05).DKD significantly provided the chance of natural conception for POR patients,which reduced the mental and financial burdens of these patients.
It has demonstrated that kidney-nourishing TCM drugs could improve ovarian function,ovarian response,and pregnancy outcomes of POR patients.Zhang et al.found that kidney-nourishing TCM drugs could decrease the level of FSH,increase the number of AFC of these patient[24].Furthermore,another two teams found kidney-nourishing TCM drugs could improve the number of AFC,oocyte maturation,fertilization and high-quality embryos,and raise embryo-transplantation rate,clinical pregnancy rate,and reduce cancellation rate of DOR patients[25,26].Wei et al.has demonstrated that using DKD for POR patient could improve the level of E2on HCG trigger day,endometrial thickness,the numbers of retrieved oocytes,fertilization rate,high-quality embryos rate,embryo-transplantation rate and clinical pregnancy rate,and decrease the Gn dosage,Gn duration and cancellation rate of these patients[13].Moreover,two other researches on DKD showed that it could significantly improve AMH levels,the number of AFC,ovulation rate and pregnancy rate in patients with DOR[27,28],which is consistent with the results of our study.
However,the mechanisms through which DKD improves pregnancy outcomes of POR patients remain to be elucidated.Li et al.found that DKD was targeted at reproduction related regions using infrared imaging[29].Ren et al.investigated the distribution of LH cells that are closely related to the sexual reflex in the grey matter of rats using immunohistochemistry SP method,and found that DKD could inhibit the apoptosis of LH cells in the midbrain,maintain their normal function,and stimulate female rats to have sex impulse and behaviour during the ovulation period,which can be responsible for the increased pregnancy rate in POR patients[30].Chen et al.found that DKD played a preventive and therapeutic role in ovulatory dysfunction in PCOS rat model by reducing the expression of transforming growth factor-beta 1(TGFβ1),connective tissue growth factor(CTGF)and androgen receptors(AR)in ovarian tissues[31].In addition,DKD could also increase the expression of endometrium homoeobox gene A10(HOXA10)and improve the endometrial receptivity in rats[32].Huang et al.showed that DKD can facilitate embryo implantation by influencing the expression of estrogen target genes[33].Clinical trials suggested that DKD could reduce the pulsatility index(PI)and resistance index(RI)of uterine artery and improved uterine perfusion and endometrial thickness,leading to an increase in the clinical pregnancy rate[34,35].
DKD involve a large number kidney-nourishing TCM drugs which have great potential in delaying the aging of rat ovary[36].It has been shown that kidneynourishing TCM drugs have great potential in delaying the aging of rat ovary,recovering the abnormal estrous cycle,reducing ovarian index,improving the abnormal secretion of sexual hormones,inducing the expression of vascular endothelial growth factor(VEGF)in ovary and regulating the expression of Bcl-2,Bax and caspase 3 that are related to the apoptosis in ovary[37].For IVF,kidney-nourishing TCM drugs can promote the maturation of oocytes and the recovery of ovarian function through the brain-derived neurotrophic factor(BDNF)signal pathway,and they can also recover the reduced levels of BDNF,CDC2,cyclin B,GSH1 and P38 and increase the response of oocytes to IVF,resulting in an increase in the implantation rate,live birth rate and placental weight[38].These studies may provide some insights into the mechanisms through which DKD can improve the reproductive outcomes of POR patients.
A potential limitation of this study is that it is not a placebo-controlled and double-blind study.Mohamed et al.showed that 96% of POR patients refused to participate in the clinical trial that included a placebo group[39].Given that the reproductive ability of POR patients decreases progressively with time[40],it is understandable for patients diagnosed with POR to refuse the 3-month placebo treatment.Thus,patients in the immediate treatment group were immediately subjected to IVF cycles.
Conclusion
In conclusion,DKD increased the ongoing pregnancy rate in POR patients,and may have promising applications in the treatment of POR,and possibly other patients undergoing IVF/ICSI-ET,which would be worth exploring.We hope that this report will stimulate further interest in the study of DKD and IVF.
Acknowledgements
This study was supported by the National Natural Science Foundation of China Nos.81774351,the Tianjin Health &Family Planning Commission(Tianjin scientific research project of priority area of traditional Chinese medicine,Nos.2018008)and Shanxi Guangyuyuan TCM Co.,Ltd.The funders had no role in study design,data collection and analysis,decision to publish,or preparation of the manuscript.We thank all the patients who participated in this study and all the medical staff involved in DKD program.We thank Tianjin CLINDA Medical Technology Co.,Ltd.for the technological support with the statistical analysis.
 TMR Modern Herbal Medicine2021年3期
TMR Modern Herbal Medicine2021年3期
- TMR Modern Herbal Medicine的其它文章
- Combination of XianGui capsule and LCZ696 inhibits doxorubicininduced heart failure in mice
- Pharmaceutical care of a patient with antibiotic-associated encephalopathy
- Research of the clinical efficacy of Qiming Granule in treatment of diabetic nephropathy by meta-analysis
- Progress of ubiquitin-proteasome system in the pathophysiology of heart failure and the intervention of traditional Chinese medicine
- Extraction and antibacterial potential of traditional medicinal plant Cypreus compressus