
Tongue swelling as a manifestation of tongue metastasis from pulmonary sarcomatoid carcinoma: A case report
2021-08-03 01:08:02MengNiGuoAnumJalilJieYingLiuRuoYuMiaoTienAnhTranJianGuan
Meng-Ni Guo, Anum Jalil, Jie-Ying Liu, Ruo-Yu Miao, Tien Anh Tran, Jian Guan
Meng-Ni Guo, Anum Jalil, Jie-Ying Liu, Ruo-Yu Miao, Jian Guan, Department of Internal Medicine, AdventHealth Orlando, Orlando, FL 32804, United States
Tien Anh Tran, Department of Pathology, AdventHealth Orlando, Orlando, FL 32804, United States
Abstract BACKGROUND Sarcomatoid carcinoma is a rare subtype of non-small-cell lung cancer, commonly associated with locally advanced disease, early metastasis, and poor prognosis.Tongue metastasis from lung cancer is a rare condition that may occur in advanced stage of the disease.CASE SUMMARY The patient was a 70-year-old female with a history of resected pulmonary sarcomatoid carcinoma (PSC) who presented with subacute tongue swelling,imparting the clinical impression of a lingual abscess. However, histologic examination of the partial glossectomy revealed a high-grade, poorly differentiated spindle and epithelioid carcinoma consistent with metastatic PSC.CONCLUSION Although uncommon, clinicians should be cognizant of the possibility of a metastatic process to the tongue mimicking a benign or inflammatory process. A high index of suspicion for metastatic disease should be maintained when tongue swelling is observed in patients with a known history of PSC.
Key Words: Sarcomatoid carcinoma; Lung cancer; Tongue; Metastasis; Tongue swelling;Case report
INTRODUCTION
Sarcomatoid carcinoma is a rare biphasic tumor expressing both malignant mesenchymal (sarcomatoid) and epithelial (carcinomatous) components[1]. Pulmonary sarcomatoid carcinoma (PSC) is a poorly differentiated subtype of non-small-cell lung cancer (NSCLC)[2], commonly associated with aggressive clinical behaviors such as locally advanced disease, early metastasis, and poor prognosis. Tongue metastases are rare clinical events that may occur in advanced stage of the disease[3].
We herein report a rare case of tongue metastasis from a pleomorphic carcinoma, a subtype of PSC. To the best of our knowledge, this is the first documented case of tongue metastasis by this subtype of PSC.
CASE PRESENTATION
Chief complaints
A 70-year-old female presented with a 2-wk-history of tongue swelling and altered mental status.
History of present illness
Six months prior to admission, the patient underwent left upper lung lobectomy for pulmonary pleomorphic carcinoma, which is considered a subtype of PSC. The neoplasm was positive for mesenchymal-epithelial transition (MET) exon 14 skipping andPIK3CAmutations, with a programmed death-ligand 1 (PD-L1) positivity of 75%.The disease was staged as T4N1M0. She was started with capmatinib for stage IV PSC with MET exon 14 skipping mutation.
One month prior, she underwent left vocal cord injection for left vocal cord paralysis. Two weeks prior, she developed tongue swelling, dysphagia and odynophagia. A computed tomography (CT) of the neck with contrast was grossly unremarkable (Figure 1A), although visualization was limited due to dental streak artifact and motion artifact. The patient was started with methylprednisolone (Medrol)dose pack by her oncologist with capmatinib on hold as it was concerned that her tongue swelling could be an allergic reaction to capmatinib. However, her tongue swelling continued to worsen to the point that she was unable to take anything by mouth. She became more lethargic that prompted her presentation to the emergency department.
History of past illness
She had a prior medical history of atrial fibrillation, deep venous thrombosis, and bilateral hip osteoarthritis.
Personal and family history
She was a former 25 pack/year smoker, but had stopped smoking 25 years prior to this presentation.
Physical examination
On arrival, patient's peripheral capillary oxygen saturation (SpO2) was 84% on room air. Physical examination revealed that the tongue and floor of the mouth were severely edematous; the deep oral tongue felt firm to palpation; the overlying mucosa was intact and of normal color; the submental space was mildly full; and cervical lymphadenopathy was not palpable.
Laboratory examinations
Laboratory studies revealed polymorphonuclear leukocytosis with white blood cell count of 20.85 × 103/μL.
Imaging examinations
Repeated CT of the neck with contrast (Figure 1B) identified a 2.7 cm × 3.2 cm × 1.9 cm lesion, which were not clearly visible in the CT one week earlier.
FINAL DIAGNOSIS
Histologic examination of the tongue mass showed a high-grade, poorly differentiated spindle and epithelioid neoplasm (Figure 2) that was positive for cytokeratin AE1/AE3 and TTF-1, but negative for p40. With positive staining for TTF-1, the tongue mass was considered a metastatic pleomorphic carcinoma of pulmonary origin to the tongue.
TREATMENT
Given the rapid interval change, an abscess was favored, with a differential diagnostic consideration of a necrotic mass. Patient was intubated for airway protection and admitted to the intensive care unit. She was started on empirical antibiotics with vancomycin and piperacillin/tazobactam. She then underwent midline partial glossectomy that revealed a submucosal mass without involvement of the tongue surface. It extended into the base of the tongue and the floor of the mouth.
OUTCOME AND FOLLOW-UP
The patient was extubated after the surgery with satisfactory oxygen saturation on room air and mentation back to normal. She then underwent percutaneous endoscopic gastrostomy tube placement for her persistent dysphagia. She was discharged home in a stable condition. To date, the patient has been receiving chemo-immunotherapy with carboplatin, Nab-paclitaxel, and pembrolizumab, with regular follow-ups with her oncologist.
DISCUSSION
Sarcomatoid carcinoma is a biphasic tumor expressing both malignant mesenchymal(sarcomatoid) and epithelial (carcinomatous) components[1]. It can occur in various anatomical sites, most frequently in the head and neck, kidneys, and lungs. PSC is a very rare, poorly differentiated subtype of NSCLC, representing 0.1% to 0.4% of all lung malignancies[2]. According to the 2015 World Health Organization classification of lung tumors, PSC is sub-classified into five subtypes[4]: pleomorphic carcinoma,spindle cell carcinoma, giant cell carcinoma, carcinosarcoma, and pulmonary blastoma.
It is more common in men in their sixth decade of age[5]. It is linked to heavy smoking and asbestos exposure. Compared to conventional NSCLC, patients with PSC have shorter overall survival and higher recurrence rate. Distant metastasis appears more frequently than local relapse. Besides common metastatic sites for NSCLC, PSC also frequently metastasizes to the kidneys and gastrointestinal tract including the esophagus, small bowel, colon, and rectum[6].
Metastasizing to the oral cavity is uncommon, constituting 1%-3% of all oral malignancies[7]. Most metastases occur in the mandible, and oral soft tissue involvement is rare. The gingiva is the most frequent site for oral soft tissue metastases (57%),followed by the tongue (27%) and tonsils (8%). The most common cancers that metastasize to the oral cavity are tumors from the lung, breast, skin, gastrointestinal tract, liver, and male genitourinary tract[8]. Metastases of primary lung cancers to the tongue are rare, with an incidence varying between 0.2% to 1.6%[9]. In general,histologic analysis of primary lung cancers metastasizing to the oral cavity reveals adenocarcinoma or squamous-cell carcinoma.
Tongue metastasis usually present with a submucosal mass, commonly with intact overlying mucosa, but occasionally with ulceration or polypoid appearance. In one study[9], there were 12 cases of lingual metastases out of 5933 patients with different types of malignancies, with tongue base the most commonly affected site due to the relative immobility and rich vascular supply of lymphatics and blood. The tumor of our patient was submucosal, infiltrating the tongue muscles, and involving the tongue base, all of which are common features of metastasis.
Due to its rarity and lack of specific gross characteristics, at the time of detection,tongue metastasis may be mistakenly diagnosed as abscess, edema, or hemorrhage[8].Common symptoms include pain, bleeding, discomfort, dysphagia, or dyspnea.Several imaging techniques, including ultrasonography, CT, and magnetic resonance imaging can be utilized for evaluation.
In our case, the patient presented with tongue swelling and associated dysphagia,odynophagia, and airway compromise. Clinically, it was initially considered an allergic reaction to her medication and later an abscess, while tongue metastasis was judged to be less likely. There were two factors that have compromised an initial accurate diagnosis. Firstly, the initial CT image could not be adequately viewed because of the artifacts from dental filling. The tongue lesion was only discovered on the following neck CT but not in the first one that was performed one week earlier.Secondly, the rapid progression of the disease, the presence of leukocytosis at presentation, and a history of recent invasive procedure to the adjacent anatomic area(injection for vocal cord paralysis), all of which place an acute pathologic process like abscess high on our list of differential diagnosis. Although clinical presentation with acute symptoms is uncommon for tongue tumors, it could occur due to necrosis or hemorrhage into the tumor. This case report provides two important lessons in patients presenting with space occupying lesions in unusual locations who already have pre-existing PSC. Firstly, accurate diagnosis by symptoms and image studies can be difficult, while pathology remains the most accurate diagnostic method. Secondly,the new lesion should be considered as the same pathologic process unless proven otherwise.
The literature on lung cancer metastasizing to the tongue is limited with only 12 cases reported from 1979 to 2020 (Table 1). Most primary pulmonary tumors were either squamous cell carcinoma or adenocarcinoma except for a single report of PSC.The patient was a 60-year-old man who had metastasis to the lateral border of the tongue two months after radical treatment for a spindle cell carcinoma, a subtype of PSC[10].
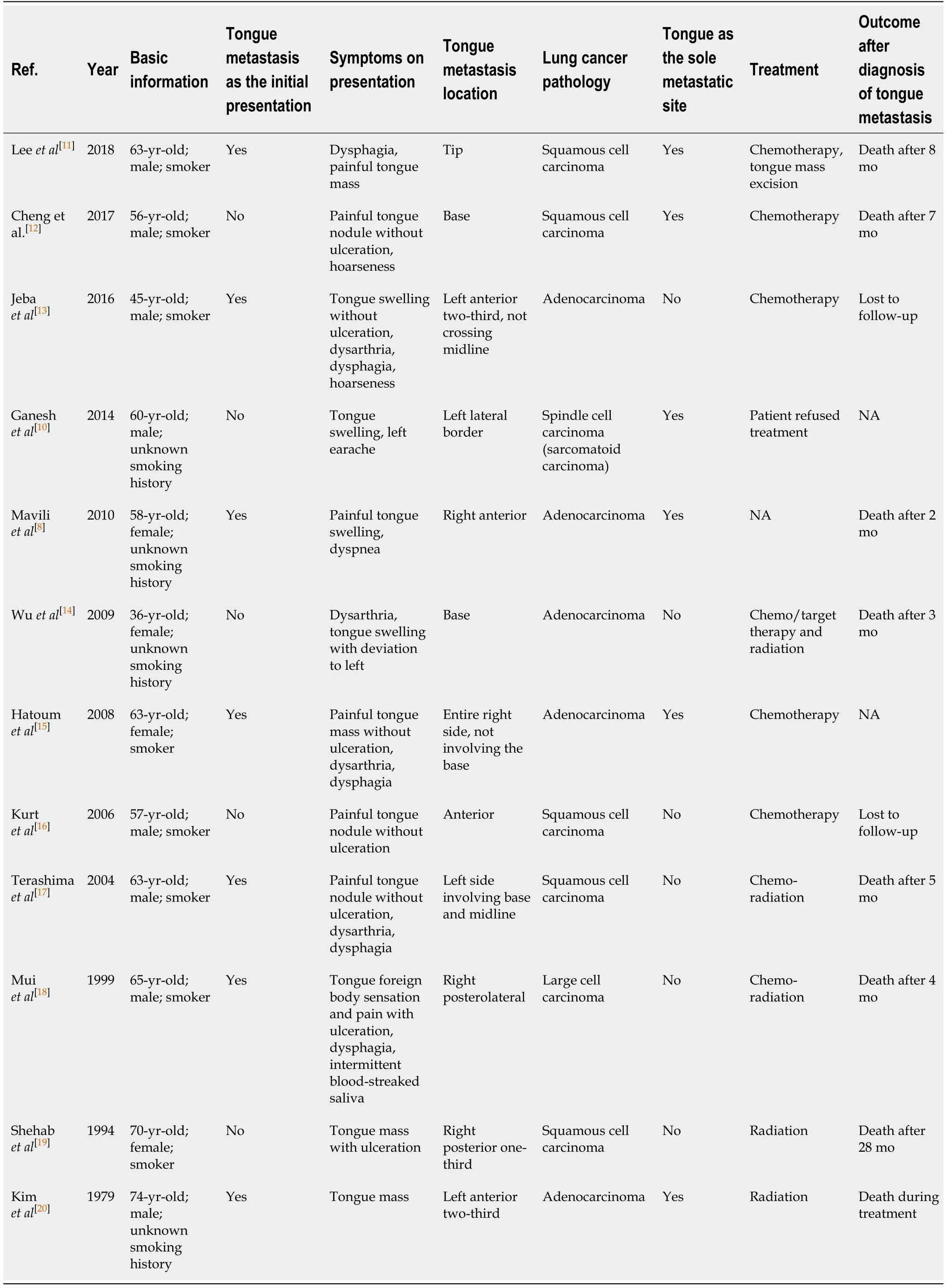
Table 1 Studies on lung cancer with tongue metastasis
Surgical treatment of PSC is the main therapeutic strategy for resectable tumors. The effects of chemotherapy and radiotherapy are limited in advanced stages. MET mutation and PD-L1 overexpression are associated with a particular propensity for sarcomatoid carcinoma[21]. A higher frequency of MET exon 14 mutations has been reported in PSCs compared to other NSCLC, with a prevalence ranging between 22%and 32%[22,23]. Capmatinib is a highly selective MET inhibitor with antitumor activity in NSCLC. In May 2020, oral capmatinib received its first global approval in the United States for the treatment of metastatic NSCLC with MET exon 14 skipping mutation.Our patient was started on this new medication but failed to achieve a good response.PD-L1 is expressed in this type of tumors in 70%-90% of cases. There are several case reports demonstrating good response in PSC patients treated with immunotherapy[24,25], and our patient is now switched to combined chemo-immunotherapy.
CONCLUSION
Tongue metastasis from PSC is an uncommon phenomenon. To the best of our knowledge, the current case is the first case report in the literature of a primary pulmonary pleomorphic carcinoma metastasizing to the tongue and the second case report of tongue metastasis from PSC. A high index of suspicion for metastatic disease should be maintained in patients with a known history of PSC when tongue swelling or radiologic image indicating a lesion in the tongue, especially near the tongue base,is observed, and appropriate investigations should be undertaken.
 World Journal of Clinical Oncology2021年4期
World Journal of Clinical Oncology2021年4期
- World Journal of Clinical Oncology的其它文章
- Lenvatinib-induced multiorgan adverse events in Hurthle cell thyroid cancer: A case report
- Hepatocellular carcinoma with biliary and neuroendocrine differentiation: A case report
- Positron emission tomography complete metabolic response as a favorable prog-nostic predictor in esophageal cancer following neoadjuvant chemotherapy with docetaxel/cis-platin/5-fluorouracil
- Cytotoxic CD8+ T cells and tissue resident memory cells in colorectal cancer based on microsatellite instability and BRAF status
- Oncogenic driver mutations in non-small cell lung cancer: Past,present and future
- GOECP/SEOR radiotherapy guidelines for thymic epithelial tumours