
Chest computed tomography findings of COVID-19 in children younger than 1 year: a systematic review
2021-07-15 01:41AlirezaGhodsiMonibaBijariSeyedAliAlamdaranAminSaberiElnazMahmoudabadiMohammadRezaBalaliSaraGhahremani
World Journal of Pediatrics 2021年3期
Alireza Ghodsi· Moniba Bijari· Seyed Ali Alamdaran· Amin Saberi· Elnaz Mahmoudabadi·Mohammad Reza Balali· Sara Ghahremani
Abstract Background The aim of this systematic review is to evaluate the chest computed tomography (CT) findings in infants with confirmed COVID-19 infection by providing a comprehensive review of the existing literature.Data sources A systematic search was conducted on PubMed and Embase from the onset of the COVID-19 outbreak to October 20, 2020, for studies that discussed the chest CT findings in infants younger than 1 year with COVID-19 infection.Results A total of 35 studies comprising 70 COVID-19 (58.5% boys) confirmed infants were included.The mean age of the included patients was 4.1 months with a range of 1 day to 12 months.Chest CT scans showed bilateral abnormalities in 34 patients, and unilateral lung involvement in 25 patients.Ground-glass opacities (GGO) (71.43%) were found to be the most prevalent chest CT manifestation, followed by peribronchial thickening (60%), linear or band-shaped opacities (32.8%), consolidation (28.57%), nodule (18.57%), effusion (7.14%) and focal lucency (7.14%).Conclusions GGO and peribronchial thickening were the most prevalent findings in the infants' chest CT scans.Linear or band-shaped opacities, consolidation, and pulmonary nodules are more common in infants than in adults.These findings suggest that the disease is more likely to be presented as an atypical pneumonia (peribronchial thickening and linear or bandshaped opacities) in this age group.Other chest CT scan manifestations can be classified as typical COVID-19 infection (peripheral GGO), lobar pneumonia (consolidation) and opportunistic infections (pulmonary nodules).
Keywords Computerized tomography · COVID-19 · Infant · SARS-CoV-2 · Systematic review
Introduction
SARS-CoV-2 primarily affects the respiratory system, and its main clinical manifestations are fever, cough, myalgia, and shortness of breath [1].Early diagnosis of the disease is of paramount importance, not only in symptomatic patients but also in asymptomatic ones that may be in their incubation period and act as a source of transmission.The gold standards for the diagnosis of COVID-19 infection are nucleic acid testing (NAT) or real-time reverse transcriptasepolymerase chain reaction (RT-PCR) [2].However, these two tests have relatively low sensitivity, i.e., high false-negative results [3].Moreover, the number of available kits for these tests is limited [4].Radiological examination plays a key role in the diagnosis of COVID-19 as well as in the diagnosis of other respiratory diseases.Among different imaging modalities, chest computed tomography (CT) has been the major imaging technique for the diagnosis and follow-up of patients with COVID-19 [5].There is some evidence that clinical symptoms along with CT findings are suggestive for COVID-19, even in the presence of a negative PCR test [6].The imaging findings of chest CT scan can be diverse and variable from one patient to another.Therefore, it is necessary to fully understand the COVID-19-associated CT scan findings for a more accurate decision-making process.
A systematic review comparing chest CT findings in children and adult populations concluded that children are more likely to have normal reports or atypical lung involvement [7].However, to the best of our knowledge, there is no study in which chest CT findings are compared among different age groups of the pediatric population.Infants below 1 year are considered a vulnerable group in this population, for whom there are very few studies in this regard, while several case reports, case series, and cross-sectional studies have reported CT scan findings of COVID-19 in children.Therefore, the present study aimed to systematically review the existing literature on specific CT scan findings of COVID-19 in young infants.
Methods
Study protocol
The present study's protocol follows the recommendations established by the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) statement [8].
Search strategy
Based on our research question of “What are the specific features of novel coronavirus infection in chest CT of infants?”, a systematic literature search was done using two major electronic databases: PubMed and Embase.We searched for studies published from December 1st, 2019 to October 20, 2020, using the following search terms: [“COVID-19” OR “coronavirus” OR “SARS-CoV-2” OR “2019-nCoV”] AND [“neonate” OR “infant” OR “newborn”] AND [“computed tomography” OR “CT-scan” OR “CT”].No language restrictions were set.Additional articles were added by a manual search of the reference lists of the selected articles and comprehensive review articles.
Selection of studies
After removing the duplicates, two investigators (MB and AG) independently screened the titles and abstracts of the remaining studies for the inclusion criteria.We included all studies that investigated CT scan findings of confirmed COVID-19 infection [with reverse transcriptase-polymerase chain reaction (RT-PCR) testing] in infants under 1 year old.We included case reports and case series that reported chest CT imaging findings of infants with COVID-19 to widen our search.Considering the exclusion criteria, we excluded studies reported as editorials, abstracts or conference proceedings, opinion articles, multimedia files, or studies on non-human species.Moreover, studies on other coronavirusrelated diseases were excluded.We also excluded the articles which had reported on a mixed adult-child population in which imaging results could not be extracted for the infants' group.
Data extraction and synthesis
Data extraction was performed by two investigators (AG and MB) using a standardized data extraction form.A pediatric radiologist (AA) screened all available chest CT scans in the included articles and reported independently.The disagreements and inconsistencies were resolved by consensus.Then, we extracted the following information from each eligible study: the first author's name and related information, such as age, gender, lesion distribution (bilateral/unilateral, posterior/other, etc.), and chest CT findings (e.g., GGO, consolidation, peribronchial thickening).Moreover, the chest CT findings were classified as typical (GGO with or without superimposed consolidations in the posterior and periphery of both lungs), atypical (nodules, cavities, bronchiectasis, pleural or pericardial effusion, lymphadenopathies, halo sign, and reversed halo sign), and borderline (a combination of typical and atypical findings) [9, 10].All findings were assessed and categorized according to a certified radiologist.
Results
Literature search and screening
The initial search yielded 1140 potential studies.After removing 329 duplicates, 811 articles were reviewed, by title and abstract, of which 742 articles were excluded.The full text of the remaining 69 articles was studied, and 34 articles were also excluded due to the lack of specific information on infants.Finally, the remaining 35 independent studies were used in the present study.A summary of the article selection process using the PRISMA fl ow chart is shown in Fig.1.
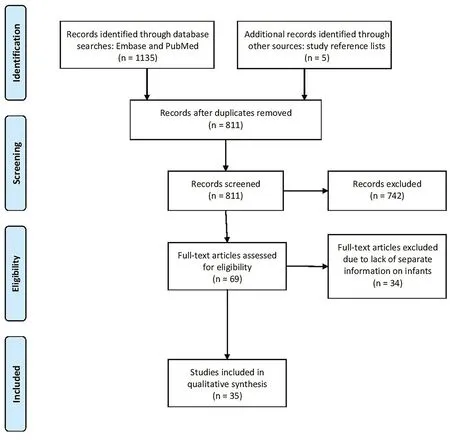
Fig.1 Flow chart of the search and study inclusion
Data extraction
Out of the 35 articles included in the study, 9 studies were cross-sectional [11- 19], 11 case reports [20- 30], and 15 case series [17, 19, 22, 31- 42].Among them, 28 studies were conducted in China, 4 studies in Iran, and 3 from Turkey, France, and Brazil.The largest study was a report by Sun et al.[16] in Wuhan, China, which included 36 infants with confirmed COVID-19 infection, but only 8 patients had chest CT scan results, which were included in our study.A total of nine variables were extracted from eligible studies (Supplemental Table 1).
Overall, 70 COVID-19-confirmed infants were studied.The mean age of the infants was 4.1 months, with a range of 1 day to 12 months.Further, 58.5% of the individuals were male, with a male to female ratio of 1.4:1.
Chest CT findings
Out of the 70 patients studied, 88.57% (62/70) had abnormalities in the chest CT findings, and 11.43% (8/70) had a normal chest CT scan.The lesions' distribution on chest CT scan was reported in 59 patients where 25 patients had unilateral lung involvement, and 34 had bilateral lesions.The distribution of the lesions in three infants was not reported [40].The chest CT images of 46 out of 70 patients were printed and re-examined and re-reported by an expert pediatric radiologist.For the remaining 24 patients, the original report of the chest CT scans which was published in the paper is presented.
The most common manifestation in chest CT scans was ground-glass opacity (GGO) in 50 (71.43%) patients, followed by peribronchial thickening (42 [60%]), linear or band-shaped opacities and subsegmental collapse (21 [32.8%]), consolidation (20 [28.57%]), and nodule (13 [18.57%]).Radiologic evidence of effusion and focal lucency was also reported in 5 (7.14%) and 5 (7.14%) patients, respectively (Fig.2).Regarding lung involvement, most patients had typical involvement (32/59), followed by borderline (17/59) and atypical (10/59) involvement.The patterns of the lesions and main chest CT findings are described in detail in Supplemental Table 1.
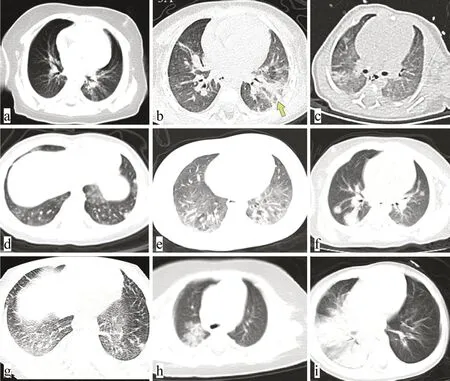
Fig.2 High-resolution CT (HRCT) patterns of COVID-19 in infants: a- c lobar grand glass opacities with strip-like appearance, d- f multinodular pattern with or without grand glass opacities or consolida-tion, g diffuse grand glass with septa thickening and unilateral rightsided pleural effusion, h, i round pneumonia and lobar consolidation
Discussion
The global number of COVID-19 cases is increasing daily, and more children are getting infected.Several guidelines consider a chest CT scan as an essential modality in the diagnosis and follow-up of COVID-19 patients [43- 45].Therefore, it is important to investigate the typical and atypical findings of chest CT scan in different age groups.
Children with COVID-19 infection tend to have milder clinical symptoms and better prognosis in comparison to adults [46- 48].In addition, the imaging findings in the pediatric population show less severe abnormalities [7, 49], which can be attributed to several factors.The angiotensinconverting-enzyme (ACE) 2 receptor, which mediates the entry of the COVID-19 virus to the respiratory epithelial cells by interacting with the spike protein of the virus, plays an important role in the pathogenesis of the disease.The number of these receptors is relatively lower in younger populations compared with adults.Moreover, the ACE2 receptors are mainly expressed in the lung tissues which may lead to milder symptoms and lesser multi-organ involvement, thus fewer critical cases among children.Besides, the ACE2 receptor is less mature and functional in children, making them less sensitive to the virus [50].In addition, the developing immune system in children results in a weaker response to the virus in comparison to adults, leading to milder symptoms and to less severe lung injury [4, 51].
Of note, it has been suggested that even within the pediatric population, there are some differences among age groups.Although numerous studies have investigated the chest CT scan findings in children infected with COVID-19, in its entirety, no study has yet focused on specific pediatric populations.Infants, children younger than 12 months, are a vulnerable group in whom the clinical features and imaging findings of the COVID-19 infection are not fully understood.Li et al.showed that in patients under 18 years old, with age increase, the disease symptoms get more severe, and the abnormal findings in chest CT scan are more prominent, indicating greater lung involvement [52].However, a largescale study on 2143 pediatric patients showed that the proportion of severe critical cases in infants was higher compared with their older counterparts, putting them at a higher risk of developing respiratory failure due to COVID-19 infection [53].However, in an analysis of the pediatric COVID-19 cases in the United States, the rate of hospitalization among the patients younger than 18 years other than infants was higher than that of infants [54].Studies seem to show controversial results regarding lung involvement in different pediatric age groups and regarding the severity of clinical and imaging findings in neonates compared to other pediatric age groups.Therefore, special consideration should be given to the determination of clinical features, imaging findings, treatment strategies, and preventive measures in this population.Accordingly, for the first time, we conducted a systematic review of the literature to provide a better understanding of abnormal chest CT scan findings in infants infected with COVID-19.
In our study, GGO was found to be the most prevalent manifestation in chest CT scans of confirmed COVID-19 infants, followed by peribronchial thickening, consolidation, linear or band-shaped opacities, and lung nodules.The majority of cases had bilateral abnormalities, more commonly in the subpleural regions of the lung periphery.In the cases with unilateral lung involvement, the lesions were mainly located in the upper lobe of the right lung.Our results are in line with previous studies in the pediatric population which found GGO and consolidation as the most prevalent CT scan findings in children [55- 59].In a systematic review of studies on chest CT scan findings in children with COVID-19 infection, GGO and consolidation were reported in 32.9% and 6.5% of the patients, respectively [60].In our systematic review, which is specifically limited to infants, GGO and consolidation were more frequent than the figures reported for the pediatric population in its entirety.Moreover, specific findings, such as peribronchial thickening, multiple lung nodules, and linear or band-shaped opacities, were more commonly reported in our included studies compared to adults and other pediatric age groups.
The presence of linear or band-shaped opacities in lung CT scans can be explained by increased septa and peribronchial thickening and the subsegmental collapse of the involved lung.As can be seen in other viral infections, such as that by the respiratory syncytial virus (RSV), the bronchial tree involvement presented as peribronchial thickening is more commonly observed in infants with COVID-19 infection than in adults.However, these observed differences should be interpreted with caution because we were not able to formally compare the frequency of different CT scan findings between infants and older children, which highlights the need for performing an original study specifically for this aim.In addition, about 11.5% of the PCR-positive patients included in our systematic review had a normal chest CT scan.They were mainly asymptomatic or had minimal upper respiratory symptoms and were suspected to have COVID-19 because of the positive history of contact with other members of the family who were known cases of COVID-19.It is worth noting that this is an underestimate of the frequency of normal chest CT scans; Patients with abnormal CT scan findings were more likely be reported.The exact pathophysiology for the explanation of these variations thus needs to be clarified in future studies.
In a study by Merkus et al., lung CT scan showed no abnormalities in 35% of pediatric patients with COVID-19 infection who had no or minor symptoms, suggesting that lung CT scan is a weak screening tool in this population with a high rate of false negatives [61].Chest CT scan also can be normal in the early stages of the disease, and a mismatch can be observed between the severity of symptoms and lung involvement [62].Similarly, we saw that 11.43% of the included infants with COVID-19 symptoms had normal CT scans, although one of the cases developed abnormalities later in a follow-up image, suggesting a delay between respiratory symptoms and observable abnormal findings in CT scan.The same delay was reported in another study in which 5.3% of patients with confirmed COVID-19 infection who had a normal chest CT scan at baseline showed abnormal pulmonary findings 2-7 days after the onset of the symptoms [63].
It should be noted that one study reported an infant with pre-existing bronchopulmonary dysplasia (BPD) and a history of prematurity who was diagnosed with the multisystem infl ammatory syndrome in children (MIS-C), and the lung involvement seen in the CT scan was critical [23].In another infant with a past surgical history for nephroblastoma and congenital heart disease, the disease presentation was critical; co-infection of COVID-19 and mycoplasma was detected, and the lung CT scan findings showed multiple pneumonia-like changes including blurred lung markings and multiple patchy consolidations in both lungs [17].The presence of comorbidities is associated with poorer prognosis and increased mortality among both children and adults, so high-risk groups should be under more strict protections [46].
Our study has certain limitations.First, different CT scan protocols had been used in the included studies, which may be a potential confounder in the observed abnormalities.Second, our review was limited mostly to case reports and case series.Furthermore, no studies analyzed the difference between the chest CT findings in infants and in other age categories.Some studies indeed included infants with COVID-19 infection, but they did not report the individual data for the patients and provided only group-level statistics.In addition, most of the included studies were from China, limiting the generalization of our findings to other populations and highlighting the need for more evidence from other countries.
This study findings help to provide a better understanding of the variations of clinical features of COVID-19 disease and its associated chest CT findings in infants who are a vulnerable age group.Our results may thus assist pediatricians and radiologists with a more accurate diagnosis in this age group based on the chest CT scan.
In conclusion, this systematic review provides an analysis of the current literature on chest CT scan findings in COVID-19 pediatric patients younger than 1 year old.GGO and peribronchial thickening are the most prevalent findings in the chest CT scans of the included infants.Linear or band-shaped opacities, consolidation, as well as pulmonary nodules, are more common in infants in comparison to other populations.The high prevalence of peribronchial thickening and linear or band-shaped opacities in infantile COVID-19 infections suggests that the disease in this age group has the nature of atypical pneumonia, like other viral infections.In total, infantile COVID-19 infections can present with four manifestations of usual COVID-19 infections (peripheral GGO), atypical pneumonia (peribronchial thickening and linear or band-shaped opacities), lobar pneumonia (consolidation), and opportunistic infections, such as fungi (pulmonary nodules).Further studies are needed to evaluate chest CT findings in infants in more detail, and appropriate guidelines should be developed for the interpretation of the COVID-related chest CT scan changes concerning these observed differences.
Supplementary InformationThe online version of this article ( https:// doi.org/ 10.1007/ s12519- 021- 00424-1) contains supplementary material, which is available to authorized users.
Author contributionsAG, SG, and MB contributed to study design.AG, AS, SA, MB, and EM contributed to the systematic search, screening, and data abstraction.SG, MB, MRB, AG, and EM contributed to writing the first draft.All the authors revised and approved the manuscript.
FundingThe authors received no specific funding for this work.
Compliance with ethical standards
Ethical approvalThis article does not contain any studies with human participants or animals performed by any of the authors.All the data involved in this study were extracted from published articles.
Conflict of interestAll the authors declared that they have no confl ict of interest.
 World Journal of Pediatrics2021年3期
World Journal of Pediatrics2021年3期
- World Journal of Pediatrics的其它文章
- Genetic etiologies associated with infantile hydrocephalus in a Chinese infantile cohort
- Maternal mental health and well-being during the COVID-19 pandemic in Beijing, China
- Causes of severe neonatal hyperbilirubinemia: a multicenter study of three regions in China
- Hedgehog signaling pathway gene variant influences bronchopulmonary dysplasia in extremely low birth weight infants
- Distinctive clinical and laboratory features of COVID-19 and H1N1 infl uenza infections among hospitalized pediatric patients
- Associations between measures of pediatric human resources and the under-five mortality rate: a nationwide study in China in 2014